
Key Takeaways
- Healthlink Dimensions exemplifies the boutique clinical-writer model, delivering high-accuracy long-form work with named reviewer trails but hitting throughput ceilings beyond a handful of sites.
- Wpromote Health represents editorial-led storytelling that fits academic medical centers competing on reputation, yet struggles to replicate flagship pieces across dozens of localized service pages.
- Cardinal Digital Marketing bundles paid and organic under one retainer, useful for high-CPC specialty acquisition, but content velocity competes with media management for the same writer hours.
- Smith & Jones anchors hospital-system brand campaigns where positioning drives downstream content, fitting regional systems but breaking on unit economics at portfolio-scale page production.
- AI-native account-level platforms pair generative throughput with credentialed clinical review, governing every location and channel from one plan rather than per-asset briefs 8, 9.
- Influence Health combines automated production with CRM-style engagement workflows across health system footprints, matching the field's shift toward integrated, relationship-driven programs 15.
- Freelance marketplaces and hybrid production offer attractive per-asset economics under 30–40 monthly assets, but coordination, governance, and version control break predictably as programs scale 3.
Why content vendor choice is now a revenue decision
Provider selection now happens upstream of the first phone call. A systematic review of online health information seeking concluded that pre-visit search and content consumption are ubiquitous and shape patient knowledge, decision support, and self-management before any clinical encounter 2. For a multi-location operator, that means the assets a content vendor produces, schedules, and updates are sitting between every paid click and every booked appointment.
The implication for budgeting is uncomfortable. Hospital-choice research shows patients actively want outcomes and experience information when comparing providers, not generic service descriptions 10. A vendor that ships keyword-stuffed location pages while ignoring outcomes content is not producing a marketing deliverable — it is producing a revenue gap.
The acquisition surface has also widened beyond the blog. Digital marketing across web, social, search, and campaign channels is now central to patient attraction and retention across hospital services 1. Vendor selection, then, is less about article quality and more about whether the production model can populate the full funnel — pre-visit education, comparison content, portal onboarding, and post-booking reminders — across every site under one program.
The four operational dimensions VPs actually budget against
Medical accuracy review depth as a real differentiator
Most vendors list "physician-reviewed" on a capabilities deck. Few can describe what that review actually does. A 2024 narrative review of trustworthy patient education identified governance of conflicts of interest and content integrity as core requirements for digital and AI-mediated education, not stylistic preferences 3. That distinction matters when a single inaccurate dosage reference or outdated procedure description can surface across forty location pages.
The differentiator is process granularity. Does the vendor route content through a credentialed clinician at outline, draft, and post-publish stages, or only at final sign-off? Are conflicts of interest with pharmaceutical sponsors disclosed in the editorial workflow itself, as the review explicitly calls for 3? Vendors that cannot describe their review cadence in operational terms — reviewer credentials, turnaround SLA, escalation paths for ambiguous claims — are running checkbox compliance rather than clinical governance.
Multi-location execution model and coordination drag
This dimension is where most vendor relationships quietly fail. Healthcare marketing has shifted from promotion-centric campaigns to strategy- and relationship-driven programs that require segmentation, experience design, and integrated communication across the patient journey 15. A vendor structured around one-off campaign deliverables cannot execute that model across 25 or 80 sites without recreating the entire coordination burden internally.
The operational question is simple. Does the vendor produce against a single account-level plan with location variants generated downstream, or does it require a separate brief, intake call, and approval cycle per site? The first model scales linearly with footprint. The second creates an N-by-N coordination matrix that consumes the VP's team in status meetings and asset routing rather than strategic work. The cost shows up as elapsed time-to-publish, not as a line item on the invoice.
Channel breadth across content, SEO, PPC, video, and portal assets
Patients do not acquire themselves through blog posts alone. The evidence base distributes unevenly across formats, and a vendor's production stack should reflect that distribution.
- A systematic review found robust evidence that video-based tools improve patient knowledge across multiple chronic illnesses, with effects on behavior and utilization for some conditions 6.
- A separate review of patient portals associated portal use with improved health outcomes and increased preventive care utilization 13.
- SMS reminders are an established mechanism for improving appointment-keeping once patients are inside the funnel 7.
- Social media is described as essential for patient communication but uneven in its quality and equity effects 5.
Translated to vendor evaluation: a shop that produces only written articles is covering roughly one corner of the evidence-supported acquisition surface. Vendors that can also script and produce video, build portal-hosted education modules, and integrate SMS sequences are addressing the formats with the strongest outcome evidence. The infographic below maps directional evidence strength to format, which is the underlying logic for treating channel breadth as a budget criterion rather than a nice-to-have.
Pricing structure: retainer, account-level, or per-asset
Pricing structure dictates incentive alignment more than headline rate. Three shapes dominate the market: monthly retainers tied to a fixed scope, per-location or per-site multipliers layered onto a base fee, and account-level platform pricing that covers all sites and service lines under one program. Each rewards different vendor behavior.
Retainers reward scope protection — the vendor delivers exactly what was contracted and treats expansion as a renegotiation. Per-location billing rewards location proliferation and creates a direct conflict when an operator consolidates underperforming sites. Account-level pricing rewards throughput and program outcomes because the vendor's revenue scales with the operator's footprint, not with billable hours per asset. Research on healthcare marketing strategy has framed this shift toward relationship- and strategy-centric models as the operational logic behind always-on content programs 11. The VP question is whether the contract structure penalizes the behavior the strategy requires.
Production models, not vendor logos: the four-tier framing
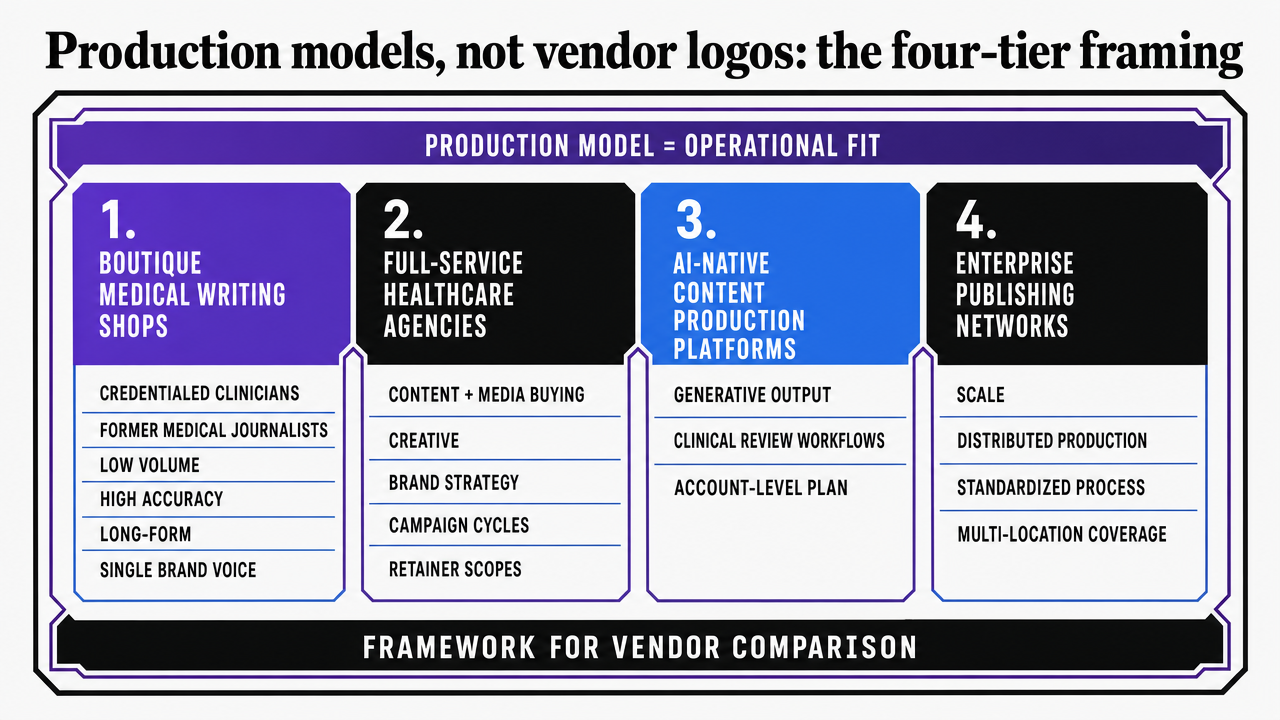
Most vendor comparisons collapse under a single ranking because they treat content companies as interchangeable boxes that ship articles. The more useful cut is by production model, since that determines whether the vendor can actually execute the operational dimensions above. Four models dominate the market a multi-location operator is realistically shopping in.
- Boutique medical writing shops staff credentialed clinicians and former medical journalists who produce a low volume of high-accuracy long-form work, typically for a single brand voice.
- Full-service healthcare agencies bundle content with media buying, creative, and brand strategy, structured around campaign cycles and retainer scopes.
- AI-native content production platforms pair generative output with clinical review workflows and execute against an account-level plan rather than per-asset briefs, an arrangement that aligns with the field's documented shift from promotion-centric to strategy- and relationship-centric marketing 15.
- Freelance marketplaces and hybrid production stitch together independent medical writers, editors, and SEOs under an operator-managed program.
The seven vendors profiled next are exemplars of these four tiers, not a ranked leaderboard.
 Visualize the four production model tiers introduced in this section as a comparison framework, since the section explicitly defines four distinct vendor archetypes with different operating characteristics
Visualize the four production model tiers introduced in this section as a comparison framework, since the section explicitly defines four distinct vendor archetypes with different operating characteristics
Trial the Platform Driving Systematic Patient Growth
Experience real-time content execution and patient acquisition results across multiple locations during your trial period.
Boutique medical writing shops
Healthlink Dimensions and the clinical-writer specialist model
Healthlink Dimensions sits in the tier of small shops staffed primarily by credentialed clinicians, former medical journalists, and pharmacy-trained editors. The production logic is human-first: every asset moves through a named clinical reviewer with a documented credential trail, and turnaround is measured in weeks rather than days. That depth aligns with the governance criteria a 2024 narrative review identified as core to trustworthy patient education, including disclosure of conflicts of interest and editorial integrity controls built into the workflow itself 3.
The constraint is throughput. A boutique that produces 8 to 15 long-form assets per month can credibly serve a single hospital brand or a specialty group with three to five sites. The same shop applied to a 40-location DSO produces a backlog within the first quarter, and location variants either get skipped or generated by junior staff without the clinical review the brand was paying for. Operators shopping this tier should price the model against asset volume per service line, not against the marquee writing samples in the pitch deck.
Wpromote Health and editorial-led storytelling at one brand
Wpromote Health and similar editorial-led shops trade clinical depth for narrative craft. The output is closer to long-form health journalism than to procedural patient education, which fits academic medical centers and destination-care brands that compete on reputation rather than service-line volume. Patient research supports the editorial angle in the right context: hospital-choice studies show patients want outcomes and experience information when comparing providers 10, and a well-reported physician profile or outcomes feature can move that information further than a templated service page.
The mismatch shows up in multi-location work. Editorial production cycles assume a single brand voice and a small set of flagship pieces per quarter, not 200 localized service pages with consistent schema and updated clinical references. Operators evaluating this tier should ask for the shop's process for replicating a flagship piece across 25 markets — the answer usually reveals whether the engagement is a content program or a brand campaign in disguise.
Full-service healthcare agencies
Cardinal Digital Marketing for integrated paid plus organic
Cardinal Digital Marketing represents the full-service healthcare agency tier built around paid-plus-organic integration rather than editorial depth. The output model bundles SEM management, programmatic display, and content production under a single account team, with creative and analytics layered into the same retainer. For specialty groups running aggressive paid acquisition against high-CPC keywords, the appeal is media efficiency: the same team that bids on the auction also writes the landing page copy it sends traffic to.
The operational tension surfaces in content velocity. Full-service agencies allocate writer hours against the same retainer that funds media management, which means content production competes for capacity with campaign optimization. When a paid campaign needs a new vertical of service-line landing pages, the content roadmap stretches. Healthcare marketing research has documented the shift away from promotion-centric tactics toward integrated, relationship-driven programs 11, and Cardinal-style agencies sit closer to the older model. Operators should benchmark monthly content throughput separately from media spend, because the two numbers move independently inside the same invoice.
Smith & Jones for hospital-system brand campaigns
Smith & Jones operates in the hospital-system bracket where content production is subordinate to brand campaign architecture. Engagements typically begin with positioning work, market research, and identity development, and content flows downstream from that strategic frame as service-line launches, physician profiles, and community-health storytelling. The model fits regional health systems consolidating acquired practices under a single master brand, where message coherence matters more than asset volume.
Multi-location DSOs and MSOs encounter friction here for a different reason than at Cardinal. Brand-campaign agencies price against strategic engagements rather than ongoing throughput, so the unit economics break once the program shifts from launching a brand to publishing 300 location-specific service pages per quarter. Patients comparing hospitals do want experience and outcomes content 10, which Smith & Jones-tier shops produce well — but they produce it at flagship cadence, not at portfolio scale.
See How Leading Healthcare Networks Streamline Patient Acquisition Content
Connect with experts to explore unified, AI-driven content operations for multi-location healthcare marketing—designed to deliver measurable efficiency and cross-location consistency at scale.
AI-native content production platforms
The account-level production stack and clinical oversight pairing
AI-native platforms invert the staffing assumption of the boutique and full-service tiers. Generative production handles outline, draft, schema, and location-variant work at machine throughput, while credentialed reviewers concentrate their hours on the steps where human judgment changes the asset: clinical claims, source verification, and edge cases involving contraindications or off-label uses. The clinical literature already validates the pairing. A 2024 JMIR protocol describing an AI chatbot for condition-specific patient information found that stakeholder-engaged design — patients, clinicians, and subject-matter experts shaping the system — is what makes scalable AI-delivered health content appropriate and trustworthy 8. The same logic applies upstream of the chatbot, at the content production layer that feeds web pages, portal modules, and campaign assets.
The operational claim that distinguishes this tier is account-level execution. One brand intelligence extract, one strategy plan, and one approval queue govern every location, service line, and channel under the program. Reviews of AI deployment in hospitals and clinics describe the same direction of travel for patient-facing tools: AI is being used to personalize interactions at a scale human teams cannot match, paired with validation and governance to manage bias and accuracy 9. The vendor question reduces to whether the platform's clinical review layer is built into the production workflow or bolted on after the fact.
Influence Health as a comparable AI-native operator
Influence Health represents the adjacent operator in this tier — a platform-led model that combines automated content production with CRM-style patient engagement workflows across health system footprints. The output covers service-line pages, campaign landing assets, and patient communication sequences under a unified data layer, which fits hospital networks consolidating marketing technology onto fewer vendors. The strategic frame matches what healthcare marketing scholarship has described as the field's move from promotion-centric tactics toward integrated, relationship-driven programs 15.
Vectoron occupies the same tier with a sharper account-level posture: a single plan covers content, SEO, PPC, and backlink execution across every site without per-location billing or account-manager overhead. Operators evaluating either should pressure-test the clinical review workflow against the governance criteria above, not the demo polish.
Freelance marketplaces and hybrid production
Marketplaces like Contently, Skyword, and direct-hire networks of independent medical writers occupy the fourth tier. The model is operator-assembled: a marketing leader sources clinicians, SEO specialists, and editors as individual contributors and coordinates them under an in-house program manager. Unit economics look attractive at small volumes — a credentialed nurse writer at $0.50 to $1.00 per word can outperform a boutique on a per-asset basis.
The model breaks on coordination, not quality. Once a program exceeds roughly 30 to 40 assets per month across multiple service lines, the program manager's time is consumed by briefing, routing, and clinical review chasing rather than strategy. Patient education governance — disclosure of conflicts, source verification, version control across location variants — has to be rebuilt manually for each contributor 3. Hybrid stacks work for operators with strong in-house editorial leadership and a stable specialist roster. They fail predictably when the program manager turns over or the footprint doubles.
If you manage 10 or more locations: the consolidation economics
Cost-structure shape across three execution models
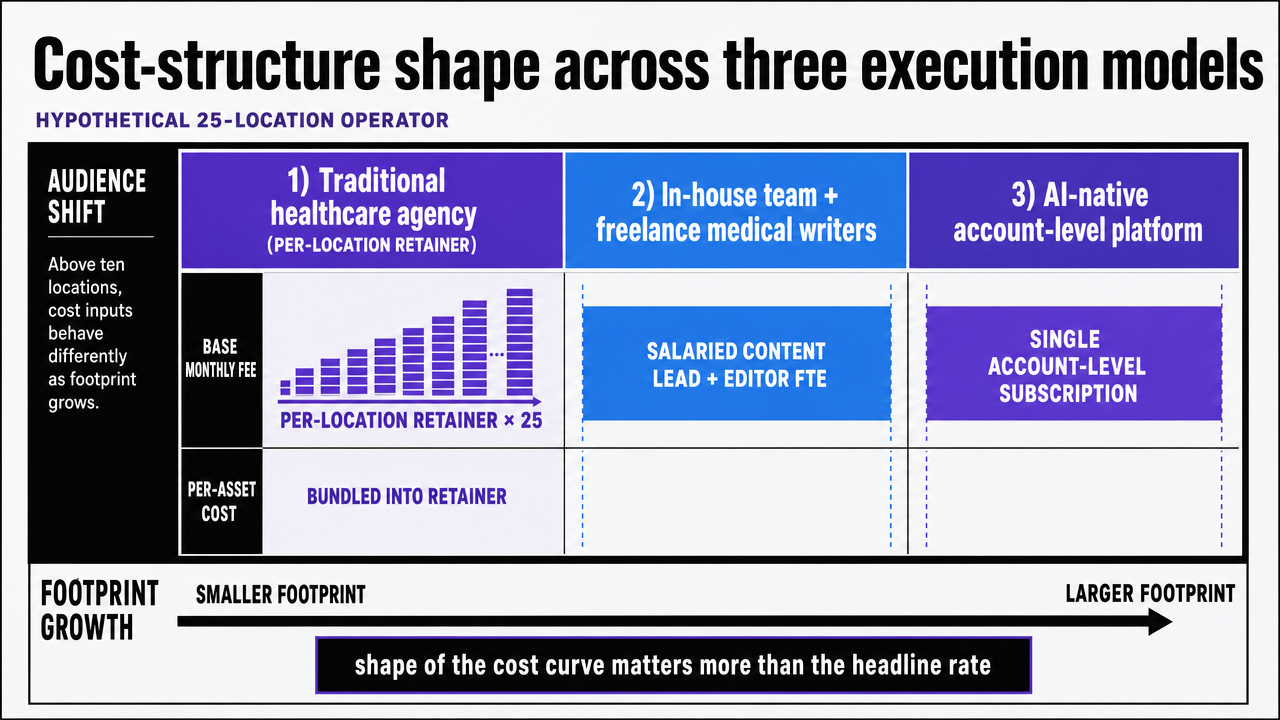
The audience shifts here. Single-site practices and small specialty groups can run any of the four vendor tiers without the unit economics breaking. Operators above ten locations face a different math problem: the same monthly invoice line items behave differently as the footprint grows, and the shape of the cost curve matters more than the headline rate.
The table below compares three execution models for a hypothetical 25-location operator. Figures are variables, not quotes — the point is to show which inputs move with footprint and which do not.
| Cost input | Traditional healthcare agency (per-location retainer) | In-house team plus freelance medical writers | AI-native account-level platform |
|---|---|---|---|
| Base monthly fee | Per-location retainer × 25 | Salaried content lead + editor FTE | Single account-level subscription |
| Per-asset cost | Bundled into retainer scope | $0.50–$1.00 per word + editor hours | Included in account plan |
| Account-manager overhead | 1 AM per 8–12 locations (vendor-side, billed through retainer) | 1 program manager FTE (operator-side) | None (Command Center workflow) |
| Review-cycle elapsed time | 10–21 days per asset across vendor and clinical reviewer | 14–30 days depending on freelancer availability | Days, governed by approval queue cadence |
| Cost behavior as footprint grows | Linear with location count | Step function at each FTE hiring threshold | Flat against location count; scales with channel scope |
The strategic frame for reading the table is the field's documented move from promotion-centric campaigns to relationship- and strategy-driven programs 11, reinforced by the historical shift away from episodic vendor engagements toward integrated execution 15. Operators above ten sites are buying a cost curve, not a deliverable.
 Visualize the three-model cost-structure comparison table presented directly in this section, reinforcing how each cost input behaves as footprint grows
Visualize the three-model cost-structure comparison table presented directly in this section, reinforcing how each cost input behaves as footprint grows
Where per-location billing and account-manager overhead actually break
Per-location billing breaks at the consolidation event. When an operator closes three underperforming sites or acquires a twelve-clinic group, the retainer renegotiation cycle stretches across two to three months and freezes content production during the exact window the new footprint needs published service pages. The vendor's revenue model rewards location count, which puts the contract in direct conflict with portfolio optimization decisions the operator makes every quarter.
Account-manager overhead breaks earlier and quieter. Once a program crosses roughly fifteen locations, the AM layer absorbs status meetings, brief routing, and approval chasing that should be running through a queue. Healthcare marketing scholarship has framed the move toward integrated, always-on execution as the operational answer to exactly this coordination tax 11. The VP-level signal is elapsed time-to-publish drifting from days to weeks while invoice totals climb — capability theater masking coordination drag.
See Unified Content Execution Outperform Traditional Medical Content Companies
Access an AI-driven platform that coordinates content, PPC, and backlinks for all locations from a single plan—track measurable patient acquisition impact without manual coordination or agency delays.
A decision framework keyed to footprint and service-line complexity
Footprint size and service-line count, not vendor reputation, should drive the tier selection. Three reference cases capture most of the operator population.
Single-brand academic medical centers and destination-care programs with one to three service lines competing on reputation should weight editorial depth and outcomes storytelling. A boutique medical writing shop or editorial-led agency produces the right asset mix at the right cadence, and the volume stays inside the throughput ceiling. Patients researching hospitals reward exactly this content type when comparing providers 10.
Specialty groups and small DSOs in the three-to-ten location range with two or three service lines are the awkward middle. Boutiques cannot keep up with location variants, and AI-native platforms can feel oversized for the asset volume. A hybrid stack — in-house editorial lead plus a vetted freelance bench — usually wins on unit economics, provided the program manager has documented governance for clinical review 3.
Multi-location operators above ten sites, or any operator running four or more service lines, should default to the AI-native account-level tier. The cost curve flattens against footprint, channel breadth covers the formats with the strongest outcome evidence, and the strategic posture matches the field's move toward integrated, relationship-driven programs 11.
Evaluating a shortlist without falling for capability theater
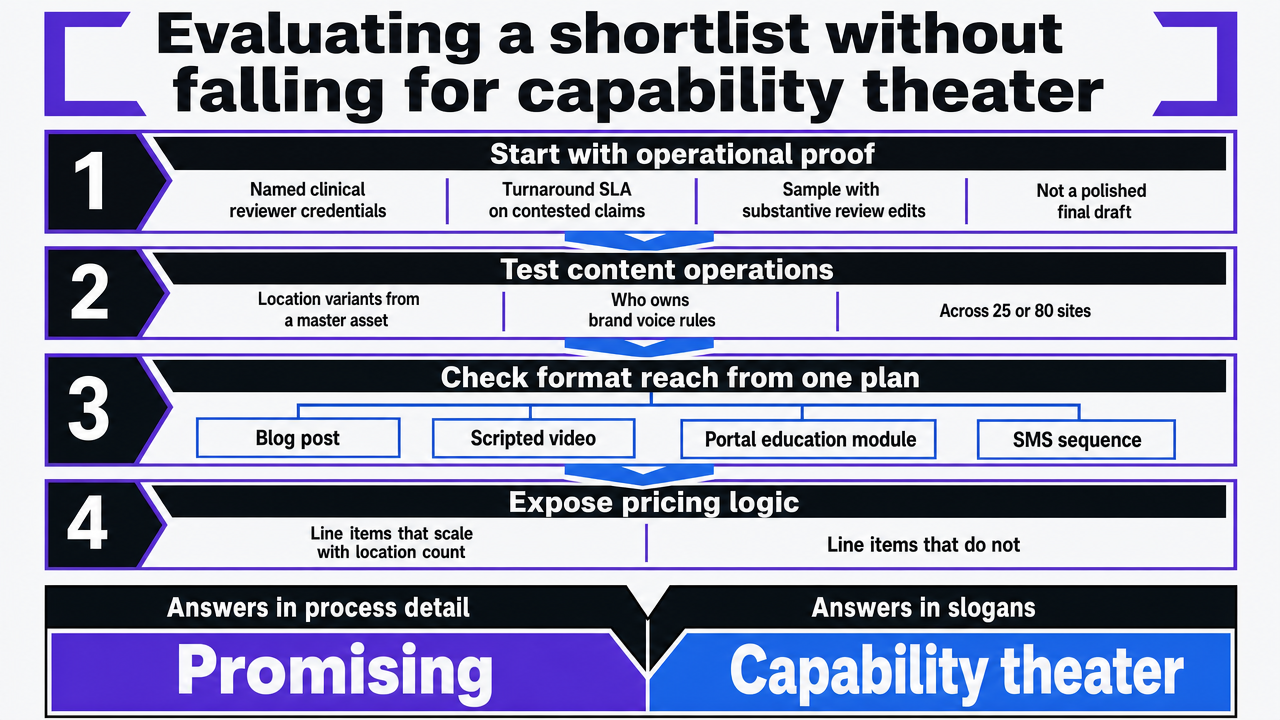
Shortlist evaluation usually collapses into a demo beauty contest. The fix is a short list of operational questions that cannot be answered with a slide.
- Ask for the named clinical reviewer's credentials, the turnaround SLA on contested claims, and a sample of an asset that came back from review with substantive edits — not a polished final draft.
- Ask how location variants are produced from a master asset and who owns the brand voice rules across 25 or 80 sites.
- Ask whether the production model can ship a scripted video, a portal education module, and an SMS sequence from the same plan that produces the blog post, since the evidence base for those formats is stronger than for written articles alone 6, 13, 7.
- Ask which line items on the invoice scale with location count and which do not.
Vendors that answer in process detail are running a program. Vendors that answer in adjectives are running a pitch.
 Visualize the section's checklist of operational evaluation questions as a process-style decision framework, since the section explicitly walks through a sequence of vendor-vetting steps
Visualize the section's checklist of operational evaluation questions as a process-style decision framework, since the section explicitly walks through a sequence of vendor-vetting steps
Frequently Asked Questions
References
- 1.The impact and challenges of digital marketing in the health care industry.
- 2.Online Health Information Seeking Behavior: A Systematic Review.
- 3.Approaches to Reach Trustworthy Patient Education: A Narrative Review.
- 4.Patient Education and Engagement through Social Media.
- 5.Social Media and Health Care, Part I: Literature Review of Social Media Use by Health Care Providers.
- 6.Video-Based Educational Interventions for Patients With Chronic Illnesses: Systematic Review.
- 7.Using text message reminders in health care services: A narrative literature review.
- 8.Adapting and Evaluating an AI-Based Chatbot Through Patient and Stakeholder Engagement to Provide Information for Different Health Conditions.
- 9.The Role of AI in Hospitals and Clinics: Transforming Healthcare in the Era of Digitalization.
- 10.National Evaluation of Patient Preferences in Selecting Hospitals: What Information Do Patients Want When Choosing a Hospital?.
- 11.The impact of marketing strategies in healthcare systems.
- 12.Digital Health Literacy: A Systematic Review of Interventions and Their Impact on Health Outcomes.
- 13.A systematic review of the effectiveness of patient education through patient portals.
- 14.Patient Education | Digital Healthcare Research.
- 15.The Origin and Evolution of Marketing in Healthcare (chapter contents).