
Key Takeaways
- Counting channel checkboxes rewards generalists and produces parallel campaigns instead of an integrated journey; evaluate whether the vendor treats one patient across channels as one person with one intent 4.
- Lead volume inflates easily without correlating to patient growth; require acquisition to be defined as a scheduled and attended visit, with cost per attended new-patient visit reported by service line and location 3.
- Content built around high-margin service lines signals optimization for the operator's P&L rather than the patient; audit vendor output for condition explainers and decision-support material patients actually search for 5.
- Disconnected pixels, CRMs, and EHR records make reporting a popularity contest; require unified identity resolution across ad platforms, web, call tracking, and intake, plus written answers on governance, bias, and data ownership 9.
- Comparing campaign quality misses the variable that decides two-year outcomes: the operating model behind the campaigns. Start diligence with pricing basis, staffing structure, and reporting rollup before judging creative 2.
The Pricing Model Hides the Real Problem
Most patient acquisition companies are built for single-site practices and then resold to multi-location operators as if the math still works. It does not. A per-location retainer that makes sense for one clinic becomes a coordination liability across twenty, because the cost line scales with site count while the outcomes line flattens against the ceiling of what fragmented execution can produce.
Operations leaders running five, fifty, or two hundred sites already see the symptoms: inconsistent local landing pages, duplicate ad accounts, three call-tracking systems, an account manager per region, and quarterly business reviews that recap activity instead of attribution. The vendor's pricing model is the tell. When fees are anchored to locations rather than to an integrated growth program, the operating model behind the invoice is single-site by design.
The right evaluation question is not which firm runs the sharpest paid search or produces the most service-line content. It is whether the partner's data, journey design, and execution capacity operate at the account level across the full footprint. Peer-reviewed work on omnichannel health care makes the point directly: the goal is improved engagement, access, and cost outcomes through integrated channels, not a stack of siloed campaigns 4. The sections below diagnose where shortlists go wrong and what filters actually separate vendors that survive a multi-site footprint from those that quietly add headcount to the operator's side of the table.
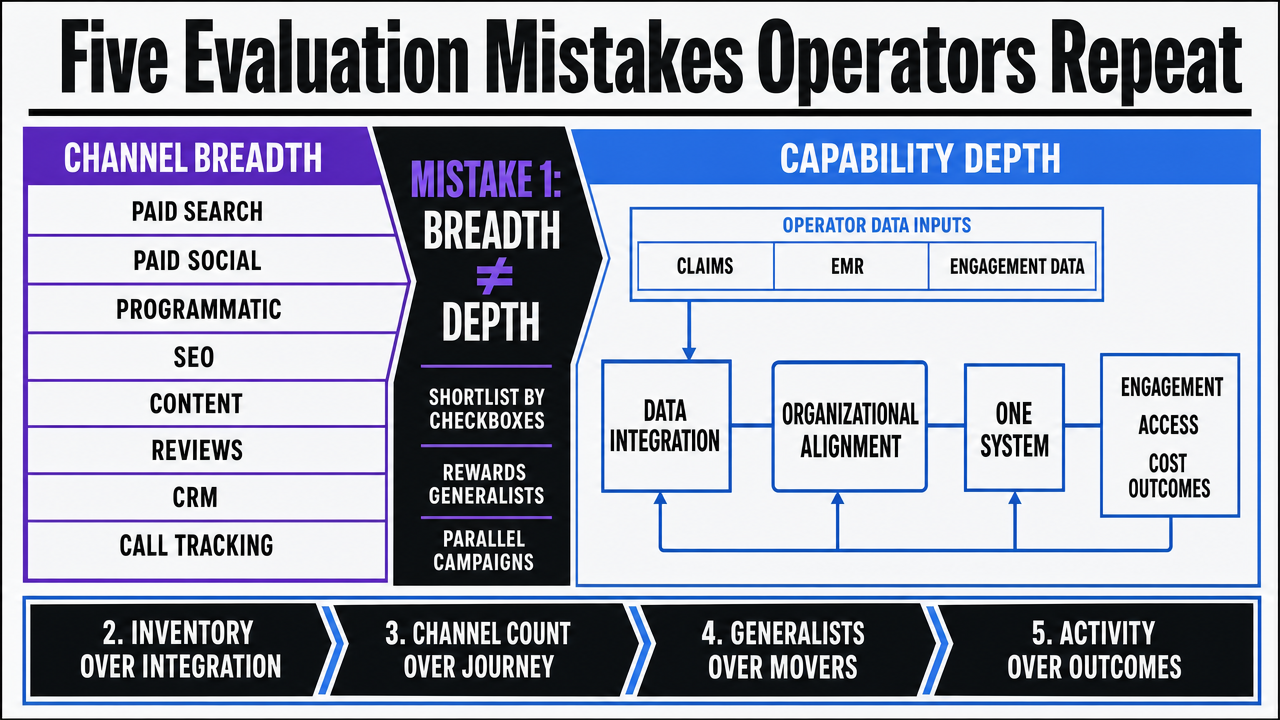
Five Evaluation Mistakes Operators Repeat
Treating Channel Breadth as Capability Depth
Vendor decks tend to lead with channel logos: paid search, paid social, programmatic, SEO, content, reviews, CRM, call tracking. The shortlist gets compiled by counting checkboxes. That math rewards generalists and penalizes the partners that actually move patient volume across a multi-site footprint.
Breadth without integration produces parallel campaigns, not a journey. Peer-reviewed work on omnichannel health care is explicit: the goal is improved engagement, access, and cost outcomes through channels that operate as one system, which requires data integration and organizational alignment, not channel inventory 4. McKinsey's omnichannel analysis reinforces the same point from the operator side, noting that leading organizations integrate structured claims and EMR data with unstructured engagement data to design coherent customer strategies 9.
The diagnostic question is not what channels the vendor runs. It is whether a patient who searches a procedure on mobile, clicks a paid ad, returns through organic three days later, and then calls a regional intake line is treated as one person with one intent, or as four anonymous events sitting in four reporting tabs.
Confusing Lead Volume with Patient Acquisition
Lead volume is the easiest metric to inflate and the least correlated with patient growth. A vendor reporting 4,000 form fills against a urology service line can be hiding a 12% qualified rate, a 40% no-show on booked appointments, and a complete blind spot on whether the patient ever converts to a billable encounter. The acquisition cost calculation on the deck is real. The acquisition is not.
Patient acquisition is a clinical access event, not a marketing event. The marketing literature is direct about this distinction, framing effective strategy as aligning communication with service quality and identifying latent patient needs that translate into appropriate utilization, not raw inquiry counts 3. Operators evaluating vendors should require a definition of acquisition that terminates at a scheduled and attended visit, with attribution that survives the handoff from ad platform to call center to EHR.
If the partner cannot report cost per attended new-patient visit by service line and location, the reporting layer is measuring activity, not outcomes. That gap shows up later as a budget that grows faster than panel size.
Ignoring Patient-Centeredness in the Vendor's Strategy
A vendor's content strategy reveals what the vendor thinks patients are. Pages built around procedure margins and high-reimbursement service lines, with little decision-support content for the conditions patients actually search, signal a partner optimizing for the operator's P&L rather than the patient's question. The peer-reviewed marketing literature flags this directly, noting that healthcare marketing can prioritize profitable services over population needs and that ethical criteria belong inside vendor evaluation 3.
Patient-centeredness is not a brand value. It is a measurable content posture. Research on online health information seeking finds that patients act as consumers, gathering information through search, literature, and direct-to-consumer channels before they ever contact a provider 5. Vendors that produce credible condition explainers, comparison content, and access information win the visit. Vendors that produce service-line ad copy and call it content do not.
Operators should audit a vendor's existing client output for content that answers patient questions the operator has not been paid to answer yet.
Underweighting Data Integration and Governance
Data integration is where most patient acquisition relationships quietly fail. The vendor runs ads against their pixel, the call center logs leads in a separate CRM, the EHR records the visit, and no system reconciles the three. Reporting becomes whichever number the loudest stakeholder trusts.
McKinsey's omnichannel work names the requirement plainly: leading organizations integrate structured claims and EMR data with unstructured engagement data to build multidimensional views of customers and inform strategy 9. The companion analysis on omnichannel engagement adds that capturing value from this integration depends on a clear plan, integrated customer data, and analytics talent, all of which are organizational, not technological 2.
Governance carries equal weight. AI-driven personalization can unlock insights from previously inaccessible data and operate at a scale traditional segmentation cannot match, but the same analysis flags data privacy, algorithmic bias, and the need for governance as live concerns 1. Operators should ask vendors how patient data flows between systems, who owns the models, how bias is monitored, and what happens to the data when the contract ends.
Buying Campaigns Instead of an Operating Model
The most expensive mistake is structural. Operators compare campaign quality across vendors when the variable that determines two-year outcomes is the operating model behind the campaigns. A boutique that runs excellent paid search for one clinic will not run excellent paid search for forty without adding account managers, project coordinators, and quarterly business reviews that consume operator time.
McKinsey's omnichannel research is direct that agile operating models, integrated data infrastructure, and continuous execution capacity are the capabilities that separate leaders from laggards 9. The medtech analysis extends the point, noting that organizations struggle to capture value from omnichannel investments when operating models, talent, and data remain siloed 2. A vendor that bills per location, staffs per region, and reports per campaign has chosen an operating model that cannot deliver coordinated execution at scale, regardless of how sharp any individual tactic looks in the pitch.
The right evaluation lens is the inverse of the standard one. Start with the vendor's operating model, then judge whether the campaigns are a natural output of it or a heroic exception to it.
 Visualize the five recurring evaluation mistakes as a clear, scannable framework that mirrors the subsections operators must avoid
Visualize the five recurring evaluation mistakes as a clear, scannable framework that mirrors the subsections operators must avoid
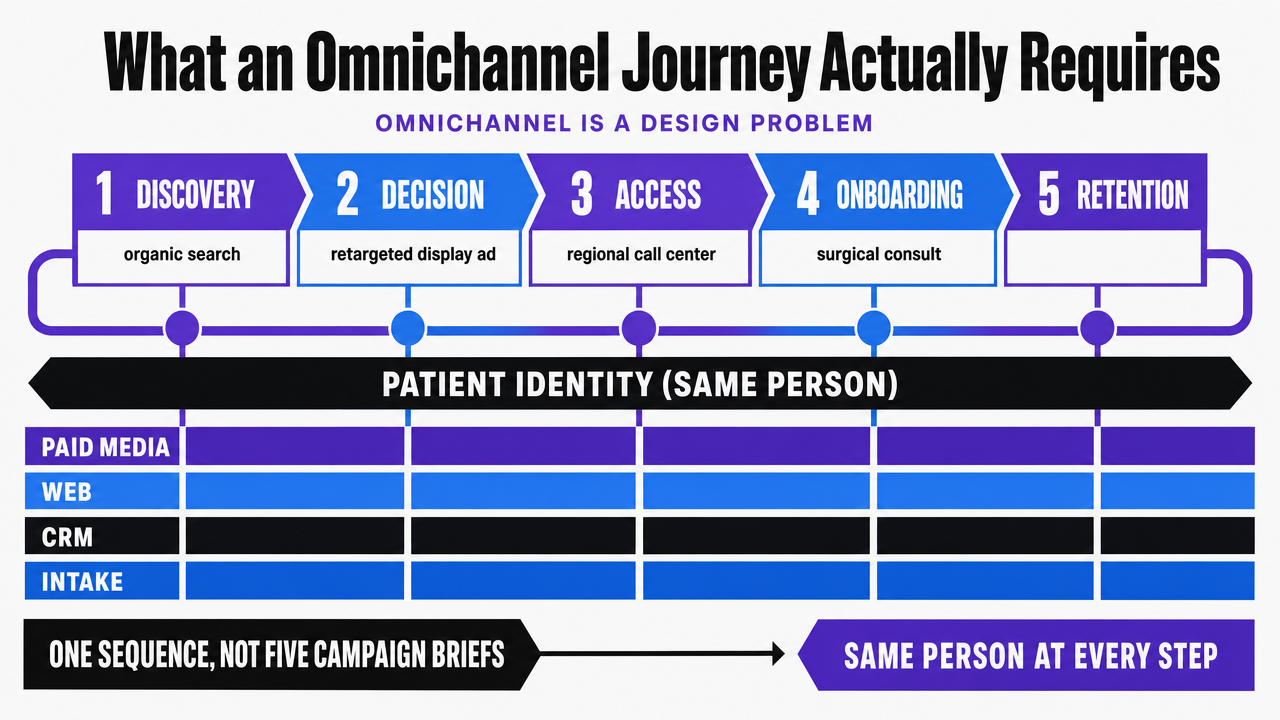
What an Omnichannel Journey Actually Requires
Operators evaluating patient acquisition partners should treat omnichannel as a design problem, not a media-mix problem. The peer-reviewed overview of omnichannel interaction in health care defines the goal directly: improve patient engagement, increase access to care, and reduce costs while improving quality 4. That definition forces three commitments most vendors avoid.
The first is journey continuity across the full lifecycle. Discovery, decision, access, onboarding, and retention are one sequence, not five campaign briefs. A patient who finds a knee replacement explainer through organic search, returns through a retargeted display ad, books through a regional call center, and arrives at a surgical consult is the same person at every step. Vendors that cannot reconcile that identity across paid media, web, CRM, and intake produce a journey with seams the patient feels and the operator pays for.
The second is data integration as the precondition, not the deliverable. McKinsey's omnichannel work frames the requirement as integrated structured and unstructured data informing engagement strategy, supported by analytics talent and a clear plan 2. Operators should ask vendors how identity resolves between ad platform, website, call tracking, and EHR-adjacent systems, and what the failure mode looks like when it does not.
The third is content built for patient decision-making, not service-line promotion. Research on online health information seeking shows patients gather information through search, literature, and direct-to-consumer channels before contacting a provider 5. The vendor's content library is the artifact that proves whether the journey is designed for the patient or for the quarterly campaign calendar.
 Show the patient journey continuity across discovery, decision, access, onboarding, and retention as one connected sequence, supporting the section's argument that omnichannel is a design problem
Show the patient journey continuity across discovery, decision, access, onboarding, and retention as one connected sequence, supporting the section's argument that omnichannel is a design problem
Test AI-Driven Patient Acquisition at Scale
Experience coordinated, multi-location patient marketing execution with real, publishable content before making a commitment.
The AI Capability Filter That Actually Matters
AI shows up on every vendor deck. Most of it is automation rebranded. The capability that actually moves outcomes is narrower and easier to test than the marketing language suggests.
McKinsey's analysis of AI in healthcare consumer experience is specific about what AI does that prior tooling could not: it unlocks insights from previously inaccessible data and enables consumer engagement and personalization at a scale traditional segmentation cannot reach 1. That framing produces four concrete filters operators can apply during diligence.
- First, personalization at scale, meaning the system adapts messaging, channel, and timing per patient based on observed behavior, not per campaign based on a quarterly brief.
- Second, integrated data, meaning the AI consumes structured and unstructured signals from web, ad platforms, call tracking, and engagement systems in one model rather than acting on a single channel's data in isolation.
- Third, governance, meaning explicit answers on data privacy, model ownership, audit trails, and what happens to trained models at contract termination.
- Fourth, bias controls, meaning the vendor can describe how the model is monitored for performance drift across demographics, service lines, and geographies.
The same McKinsey analysis flags data privacy, algorithmic bias, and governance as live concerns that scale with AI deployment, not legacy issues that disappear with better tooling 1. Operators should treat a vendor's inability to answer the governance and bias questions as disqualifying, regardless of how strong the personalization pitch sounds. A capability that cannot be governed cannot be operated at the account level across a multi-site footprint.
The Digital Foundation No Vendor Should Skip
Before any AI capability or omnichannel pitch deserves serious evaluation, the vendor's grasp of the base layer should be tested. The peer-reviewed digital marketing analysis for private practice is direct about what that layer contains: a modern website, search visibility, online reviews, and patient communication tools form the digital front door that influences provider choice 10. Any partner that cannot show competence on each of these elements is not ready to run a multi-site program, regardless of the technology stack behind the proposal.
For multi-location operators, the foundation question shifts from quality to consistency. One excellent website does not solve the problem when forty location pages render different hours, three review profiles point to the same address, and the call-to-book path differs by region. Operators should ask vendors to demonstrate how location data, schema, review aggregation, and intake routing stay synchronized as sites open, close, or rebrand.
The same source notes that older patient segments remain less digitally engaged, which means a digital-only foundation can underserve population mix in certain service lines 10. A vendor that treats the digital front door as the entire building is solving the wrong problem.
See How Leading Patient Acquisition Platforms Scale Without Added Overhead
Connect with a strategist to review benchmarks, automation workflows, and reporting frameworks used by multi-location healthcare groups for efficient, cost-controlled patient acquisition.
If You Manage Multiple Locations: The Coordination Tax
Why Per-Location Retainers Scale Linearly and Outcomes Don't
This section narrows from general vendor evaluation to the economics that only multi-site operators face. A retainer priced per location is a sensible unit of measure for a single clinic, where the work and the site are the same object. Apply that same unit to a group with twenty sites and the pricing scales linearly while the outcomes do not.
The reason is that patient acquisition value at scale comes from cross-site assets, not site-by-site activity. A condition explainer that ranks for a metro-wide search term serves every location in the metro. A reputation workflow that standardizes review response across the footprint produces consistency no single-site retainer can replicate. A unified identity graph that resolves a patient across paid media, web, and intake is built once and reused everywhere. McKinsey's omnichannel work makes the underlying point: value comes from integrated data, agile operating models, and a clear plan, not from replicated tactical effort 9.
When the vendor's pricing line grows in lockstep with site count, the operator is paying twenty times for work that should compound. The coordination tax sits in the gap between what was billed and what was actually leveraged across the group.
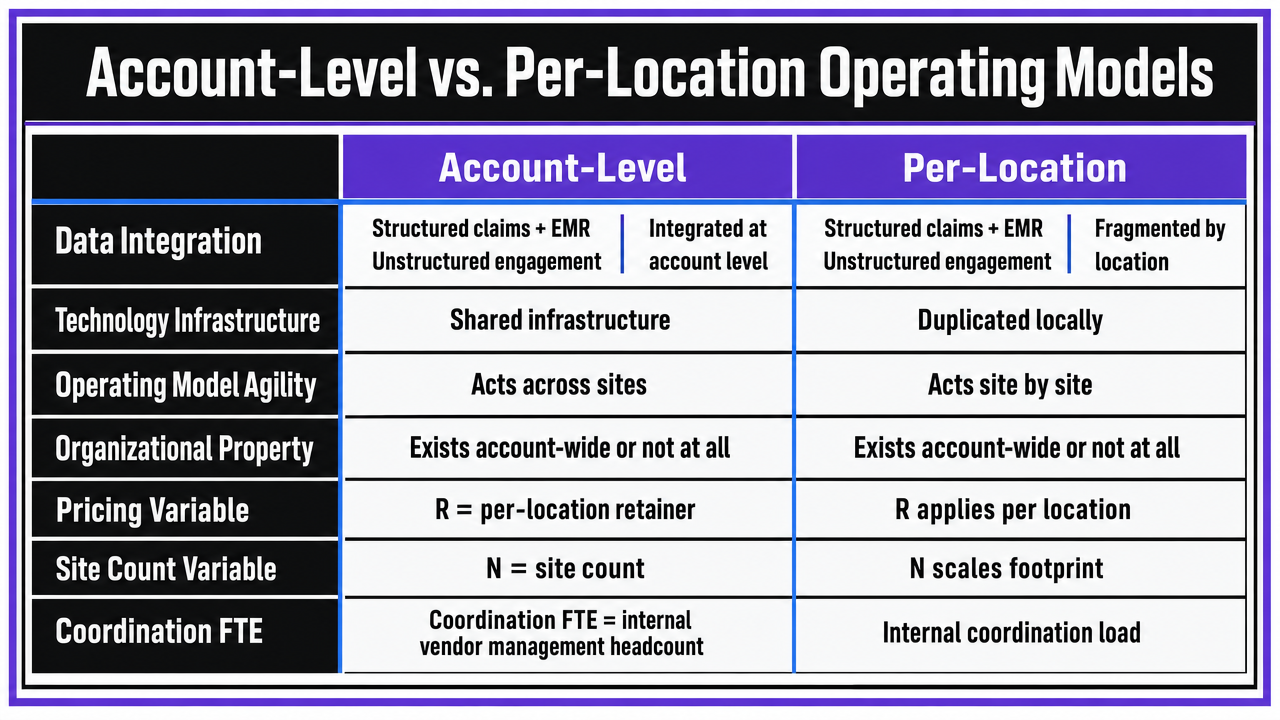
Account-Level vs. Per-Location Operating Models
The structural difference between the two models shows up most clearly when laid out across the operational dimensions that determine multi-site performance. McKinsey's omnichannel analysis identifies the capabilities that separate leaders: integration of structured claims and EMR data with unstructured engagement data, robust technology infrastructure, and agile operating models that can act on that integration 9. Those capabilities are organizational properties, which means they either exist at the account level or they do not exist at all.
The comparison below uses operator-supplied variables rather than invented benchmarks.
R : represents the per-location retainer the operator already pays.
N : represents site count.
Coordination FTE : represents the internal headcount the operator dedicates to managing the vendor relationship.
| Operational dimension | Per-location retainer model | Account-level integrated model |
|---|---|---|
| Pricing basis | R × N (scales linearly with sites) | Account-level fee (scales sublinearly with sites) |
| Scope coverage | Channels per site, gaps between sites | Full footprint, all channels, one plan |
| Data integration | Per-site pixels and reports | Unified identity across ad, web, call, intake |
| Coordination layer | Account managers per region plus operator FTE | Single approval surface, no regional handoffs |
| Execution latency | Brief, review, approve, launch per site | Continuous execution against one strategy |
| Scaling behavior | Cost and complexity rise with each new site | New site inherits existing assets and workflows |
The table is not a pricing argument. It is a structural one. A vendor that bills per location has chosen an operating model in which integration is the operator's problem, not the partner's deliverable. A vendor operating at the account level has chosen the inverse. Operators evaluating replacement or consolidation should require the partner to describe which model they actually run, then verify the answer against how the contract is priced, how the team is staffed, and how reporting rolls up.
 Render the comparison table from the article as a clean side-by-side operating model comparison, supporting the section's structural argument
Render the comparison table from the article as a clean side-by-side operating model comparison, supporting the section's structural argument
Connecting Acquisition to Retention and Clinical Outcomes
Most patient acquisition vendors stop measuring at the booked appointment. The operator's general ledger does not. A patient acquired through paid search who no-shows the first visit, attends once and never returns, or cycles back through the emergency department within thirty days is a marketing cost without a clinical or financial return. Partners that cannot speak to the lifecycle past the lead handoff are operating on a definition of success the operator cannot use.
The clinical literature draws the connection directly. The StatPearls review on hospital readmissions identifies improved transitions of care, patient education, and structured follow-up as the multifaceted strategies that move the readmission rate, which means communication infrastructure sits inside the outcome, not adjacent to it 6. A DNP evaluation of automated text and phone follow-up after discharge tied the same outreach mechanics that acquisition vendors already operate to measurable changes in patient satisfaction scores and thirty-day readmissions 7. A companion project on revised discharge processes added that stratifying patients by readmission risk and standardizing communication produces gains in both satisfaction and utilization 8.
The evaluation question for operators is whether the acquisition partner can extend the same identity graph, content engine, and outreach automation past the first visit into onboarding, recall, and post-discharge follow-up. A vendor whose technology ends at the conversion event has built half a system. A vendor whose journey design treats the patient as the same person before and after the appointment is the one whose acquisition spend compounds into retention.
Scale Patient Acquisition Without Linear Cost Increases
Access AI-driven patient acquisition workflows designed for multi-location healthcare operators—enabling seamless expansion, centralized oversight, and measurable efficiency gains, all without adding headcount or increasing coordination overhead.
A Working Shortlist Method for Replacement or Consolidation
Operators replacing an incumbent or consolidating a fragmented vendor stack benefit from a shortlist method that filters on operating model first and creative output last. The sequence matters because creative quality is the easiest variable to test in a pitch and the least predictive of two-year performance across a multi-site footprint.
- The first pass is structural disqualification. Any vendor that prices per location, staffs account managers per region, or cannot describe how identity resolves between ad platform, web, call tracking, and intake systems exits the list. McKinsey's omnichannel analysis names integrated data, robust technology infrastructure, and agile operating models as the capabilities that separate leaders, which means the absence of any one of them is a structural defect, not a gap to negotiate around 9.
- The second pass is evidence of patient-centered output. Operators should request the vendor's existing content library and audit it for condition explainers and decision-support material, not service-line ad copy, given that patients gather information through search and direct-to-consumer channels before contacting a provider 5.
- The third pass is governance. AI, automation, and data ownership questions get answered in writing before any pilot scope is drafted 1.
Closing the Vendor Question
The vendor question is not which firm runs the best campaign. It is which operating model survives the operator's footprint without quietly adding coordination headcount on the operator's side. Pricing basis, data integration, governance, and lifecycle reach are the variables that decide the two-year outcome. Channel logos and case studies are not.
Operators ready to test an AI-native, account-level alternative against the incumbent stack can evaluate Vectoron as one of the candidates that prices and staffs at the account level rather than per location.
Frequently Asked Questions
References
- 1.Harnessing AI to reshape consumer experiences in healthcare.
- 2.How medtechs can meet industry demand for omnichannel engagement.
- 3.The impact of marketing strategies in healthcare systems.
- 4.An Overview of Omnichannel Interaction in Health Care Services.
- 5.Patient-Centered Care and Healthcare Consumerism in Online Health Information Seeking.
- 6.Reducing Hospital Readmissions.
- 7.Impact of an Automated Text and Phone Call Post-Discharge Follow-Up System on Patient Satisfaction and Hospital Readmissions.
- 8.Improve Readmissions and Patient Satisfaction Scores with a Revised Discharge Process.
- 9.Omnichannel engagement in medtech: The time is now.
- 10.Digital Marketing for Private Practice: How to Attract New Patients.