Key Takeaways
- Creative breaks at scale because coordination, compliance queues, and brand drift compound non-linearly with each new location, making production capacity — not creative talent — the binding constraint.
- Account-level execution replaces per-location retainers by running one brief, one brand source of truth, and programmatic DMA, service-line, and clinician voice layers applied to a master asset.
- HIPAA authorization 5, FTC substantiation 6, and AMA truthfulness standards 3belong in the brief as sourced inputs, not as final-stage review gates that throttle time-to-market.
- Hold creative accountable to booked-appointment CAC by service line, contribution margin per patient, and system-level LTV-to-CAC, with Performance Max, Advantage+, and local SEO carrying acquisition.
Why creative breaks at the 10th location
A creative system that works at five locations almost always fails at fifteen. The brief that produced one winning orthopedics campaign in a single DMA now has to produce variants for nine markets, four service lines, and three clinician archetypes — each governed by HIPAA marketing authorization rules, FTC substantiation standards, and AMA truthfulness norms before it can run. The work itself does not get harder. The coordination around it gets exponentially harder.
This is where most multi-location healthcare operators hit the wall.
McKinsey's research on consumer-led healthcare growth finds that organizations capturing disproportionate share are those that deliver integrated, end-to-end experiences rather than disconnected local campaigns 2. Healthcare consumers now expect the same coordinated digital experience they get from retailers and banks 1. A patient researching dermatology in Charlotte and then traveling to a sister clinic in Raleigh notices when the brand, intake flow, and creative tone shift between visits. So does the algorithm scoring the group's Performance Max campaigns.
The reflex response — hire more per-location agencies, add account managers, build market-specific creative — compounds the problem. Each new retainer adds a coordination layer. Each per-market brief adds drift from the system brand. Each isolated review cycle slows time-to-market while compliance backlogs grow.
The groups that scale creative past the tenth location stop treating it as a creative discipline and start treating it as a production and governance system. The rest of this article maps that system.
The production math behind multi-location creative
Asset volume scales non-linearly with locations and service lines
The asset count is the first thing that breaks. A single-market orthopedics campaign might ship with six core creative units: two video cuts, two static social variants, a landing page, and a paid search ad group. Move that same brief to a 25-location group running four service lines — orthopedics, sports medicine, joint replacement, spine — and the production load is not 25 times larger. It is closer to 600 finished assets before localization layers are applied.
The multiplier compounds across four axes:
- location count
- service line count
- channel format requirements
- lifecycle stage (awareness, consideration, conversion, retention)
A group running Performance Max, Meta Advantage+, YouTube, and local landing pages already needs format variants for each channel. Add metro-specific photography, clinician callouts, and language variants, and the matrix expands again.
This is why per-location creative production fails on math alone. Each new market does not add one campaign's worth of work; it adds a row across every existing column. McKinsey's consumer-led growth research finds that the operators capturing outsized share are those running integrated, end-to-end programs rather than disconnected local efforts 2. The asset volume problem is what makes that integration economically necessary, not just strategically preferable. Production capacity, not creative talent, becomes the binding constraint.
Per-location retainers versus account-level execution
The traditional agency response to asset volume is to add agencies. One per region, sometimes one per location. The cost stack that results is what most multi-location healthcare CFOs eventually flag.
Consider the structural comparison across a 10, 25, and 50 location operator, expressed in coordination variables rather than invented dollars:
| Cost component | Per-location retainer model | Account-level execution |
|---|---|---|
| Monthly retainer count (10 / 25 / 50 locations) | 10 / 25 / 50 separate retainers | 1 program fee |
| Annual retainer billings | Retainer × N × 12 | Single annual program cost |
| Coordination touchpoints (weekly status calls) | 10 / 25 / 50 standing meetings | 1 standing meeting |
| Brand system instances maintained | N parallel interpretations | 1 source of truth, localized |
| Asset versioning multiples | N × service lines × channels | 1 master × automated localization |
| Internal FTE equivalents to manage agencies | ~1 FTE per 8–12 locations | ~1 FTE total at program level |
| Compliance review queues | N parallel queues | 1 centralized queue |
| Time from brief approval to in-market | Bounded by slowest agency | Bounded by single production cycle |
The non-linear cost is in the rows that scale with N:
- coordination touchpoints
- brand system instances
- FTE management overhead
- compliance queues
A 50-location group running per-location retainers is not paying 50 times more for creative. It is paying 50 times more for the operational scaffolding around creative, while the creative output itself grows less consistent.
Account-level execution inverts the curve. One brand system, one compliance queue, one production cycle, with localization handled downstream of the master asset. McKinsey's work on consumer-led healthcare strategy supports the economic logic: groups delivering coordinated end-to-end experiences capture disproportionate growth, while those running parallel local programs absorb the coordination cost without the integration benefit 2. The decision a VP of Marketing is making is not creative versus creative. It is whether the cost of N parallel systems is justified by any measurable lift over a single account-level system. In practice, it rarely is.
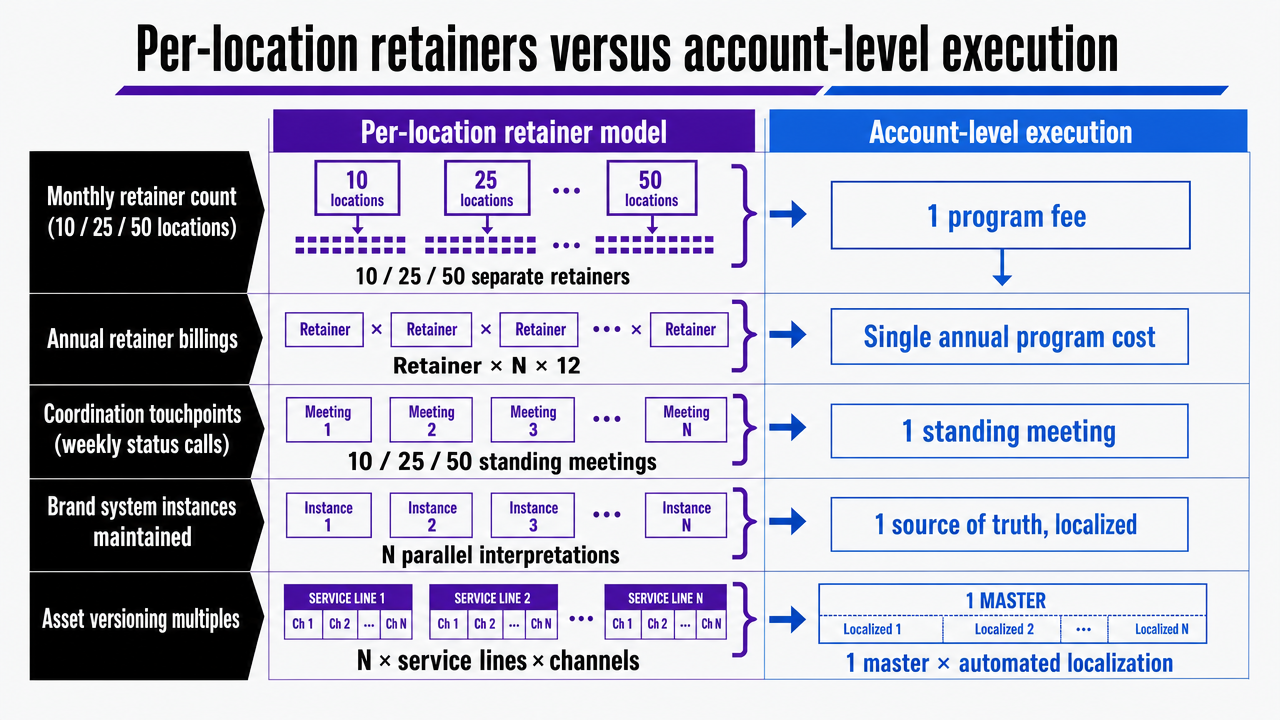 Visualize the structural comparison table contrasting per-location retainer model versus account-level execution across coordination variables that the section explicitly enumerates
Visualize the structural comparison table contrasting per-location retainer model versus account-level execution across coordination variables that the section explicitly enumerates
One brand system, localized at the metro and service-line level
Why brand consistency drives behavior, not just recall
Brand consistency in multi-location healthcare is often defended as a recall argument: patients should recognize the logo, the color system, the tagline across markets. That framing understates the operational value.
The systematic review of health branding finds that brand elements drive behavioral choice by building consumer relationships and identification with branded health behaviors and their benefits — not just by improving aided recall scores 7. For a dermatology group running campaigns in eight metros, that distinction matters. A consistent brand system increases the probability that a patient who saw a Meta awareness unit in Phoenix and later searched for a clinic in Tucson recognizes the same operator and converts, rather than treating each location as a separate provider decision.
McKinsey's consumer-led growth analysis makes the same point from the demand side: groups delivering integrated end-to-end experiences capture disproportionate growth, while fragmented brand presentation forfeits the compounding effect of system-wide awareness 2. A patient who has interacted with three touchpoints across two locations and one service line is materially closer to booking than three patients with one touchpoint each.
Brand consistency is the mechanism that lets isolated impressions accumulate into a behavioral signal. Treat it as a conversion-economics input, not a design preference.
Localization layers: DMA, service line, and clinician voice
Consistency is not uniformity. The operators who run the same creative file across every market lose the conversion lift that comes from local relevance. The ones who let each market reinvent the brand lose the compounding effect described above. The working model sits between the two, organized as a layered system rather than a series of one-off adaptations.
Three localization layers carry most of the load:
- DMA layer. Metro-specific photography, landmarks, and references where they materially affect resonance. Phoenix and Minneapolis patients respond to different environmental cues. Local SEO landing pages, Performance Max asset groups, and Meta Advantage+ creative variants inherit this layer.
- Service-line layer. Orthopedics, dermatology, behavioral health, and urgent care each have distinct patient intents, decision timelines, and claim conventions. The brand voice stays constant; the message hierarchy shifts. A spine campaign leads with diagnostic specificity. A behavioral health campaign leads with access and confidentiality.
- Clinician voice layer. Where individual physicians appear in creative, the AMA's truthfulness and non-misleading standards apply at the asset level 3. Clinician-specific quotes, credentials, and outcome references are sourced once at the brief stage and reused across the markets where that clinician practices, rather than re-cleared per campaign.
Each layer is a transformation applied to the master asset, not a parallel production track. A 25-location group running four service lines does not produce 100 campaigns. It produces one campaign with three localization layers applied programmatically, with compliance and brand checks running once on the master and again on the localized output.
Test unified healthcare advertising across all locations
Execute and measure real multi-location campaigns with full reporting for seven days, risk-free.
Compliance as a creative input, not a review-stage blocker
Most multi-location creative programs treat HIPAA, FTC, and AMA standards as a final review gate. Legal reads the asset, flags the problems, and the campaign loops back through production. At one location, that loop is annoying. At fifty, it is the single largest source of time-to-market drag.
The operators who solve this stop reviewing for compliance and start briefing for it. Each constraint enters the work as a brief input with a named owner and a sourced artifact, not as a checklist applied after the file is built.
Three standards carry most of the weight:
- HIPAA marketing authorization (HHS). The Privacy Rule requires written patient authorization before PHI is used or disclosed for marketing, with narrow exceptions 5. Upstream, this becomes a brief field: every asset that references a real patient, outcome, or testimonial ships with a signed authorization on file, identified by patient ID and asset ID. Targeting logic that segments audiences based on diagnosis or treatment status is scoped at the brief stage against the same boundary. Reviewers stop hunting for PHI exposure because the brief makes it impossible to introduce.
- FTC substantiation (Health Products Compliance Guidance). The FTC requires competent and reliable scientific evidence behind health claims, applied across products and increasingly to service advertising 6. Upstream, this becomes a claim substantiation file attached to the brief. Every outcome statement, comparative claim, or efficacy reference points to a specific source — clinical literature, peer-reviewed data, or internal outcomes data with documented methodology. If the substantiation does not exist at brief stage, the claim does not enter the creative.
- AMA truthfulness and non-misleading standards. The AMA Code requires physician advertising to be truthful, understandable, and free of language that creates unjustified expectations 3. The Code's broader framework on professional communications reinforces that system-level campaigns inherit the same standard as individual physician ads 4. Upstream, this becomes a clinician sourcing rule: credentials, board certifications, outcome references, and personal quotes are verified once at the brief stage, stored against the clinician's profile, and reused across every market where that clinician practices.
The downstream effect on production is the point. A 25-location group running four service lines does not send 100 assets through four parallel compliance queues. It sends one brief through one upstream review, then ships the localized output through a lighter confirmation pass that checks for variance, not original risk. Compliance shifts from a bottleneck applied to finished work to a constraint shaping the work as it forms — which is the only version of the workflow that scales without doubling legal headcount per ten new locations.
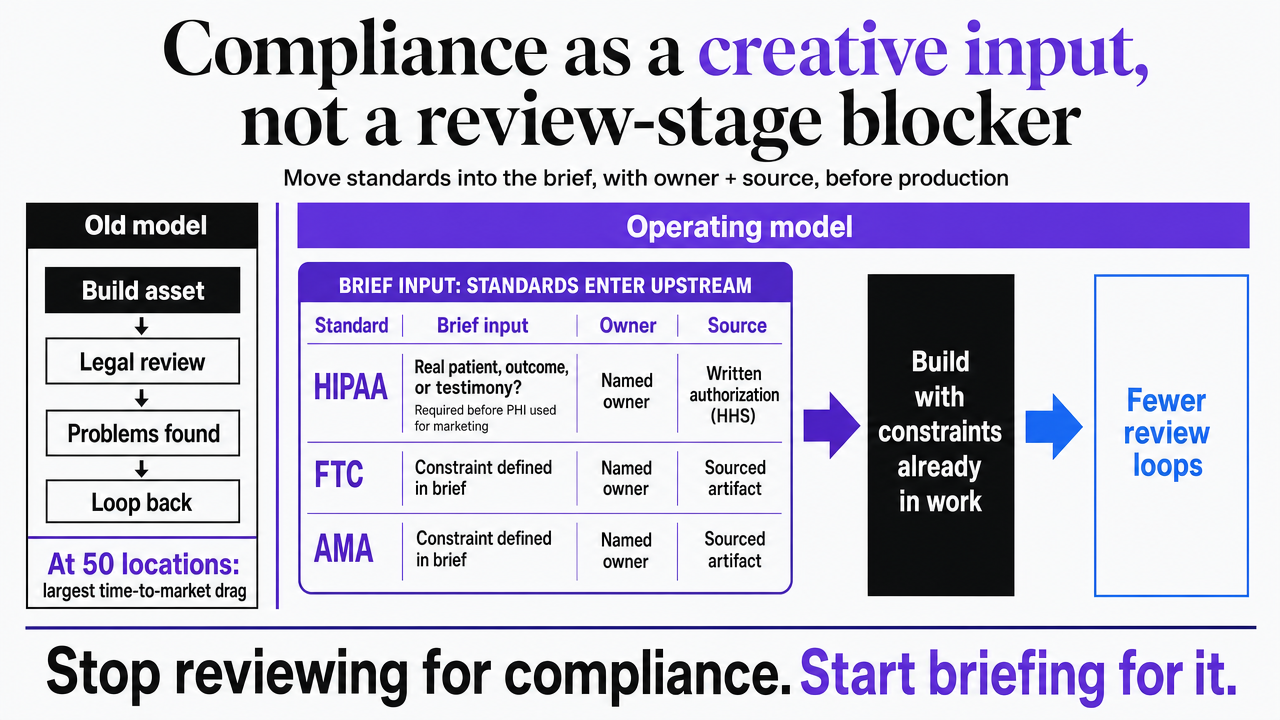 Visualize the three regulatory standards as upstream brief inputs rather than downstream review gates, mapping the section's compliance governance model
Visualize the three regulatory standards as upstream brief inputs rather than downstream review gates, mapping the section's compliance governance model
How generative AI is shifting patient research and what creative now has to do
Patient research no longer starts on Google. A growing share of it starts inside a chatbot, where the patient describes a symptom set in plain language and asks for guidance on what kind of provider to see and where to find one nearby. Deloitte's 2024 U.S. consumer survey on healthcare generative AI found that roughly 37% of consumers had used generative AI for health reasons, a meaningful but still minority share that reflects active experimentation rather than mass adoption 9. The same firm's 2025 Connected Consumer survey, which is not healthcare-specific, found that 53% of connected consumers were experimenting with or regularly using generative AI overall, up from 38% the prior year 10. The gap between the two figures is the operational signal.
General digital behavior is running ahead of healthcare-specific behavior, and the lag is narrowing.
For multi-location creative, this changes the job description of awareness and consideration assets. A patient who has already asked a chatbot about rotator cuff pain arrives at a paid impression with a working vocabulary, a shortlist of provider types, and often a draft of clarifying questions. The awareness unit that wins is not the one that introduces the condition. It is the one that confirms the patient's working hypothesis, surfaces the specific service line, and shortens the distance to a booking decision at a named location.
Three creative shifts follow from that change in patient state:
- Specificity beats education. Generic condition-awareness creative competes with a chatbot that already explained the condition for free. Service-line specificity — modality, recovery timeline, clinician credential — does work the AI cannot do without provider data.
- Named-location proof points carry the click. When a patient has already narrowed to a provider type, the next decision is geographic. Creative that pairs the service line with a specific clinic, wait time, or scheduling option converts higher than national brand creative routed to a local landing page.
- AI-themed creative requires substantiation. Campaigns that reference AI triage, virtual intake, or algorithmic scheduling inherit the FTC standard already covered in the compliance section 6. Trust in healthcare AI remains fragile in the Deloitte data 9, so the creative cost of overstating an AI capability is higher than the lift from mentioning it.
The planning consequence for a VP of Marketing is to move budget from top-of-funnel education toward mid-funnel specificity, and to instrument the handoff from chatbot-influenced search behavior into booking flows. The patient is arriving later in the journey than the legacy funnel assumes.
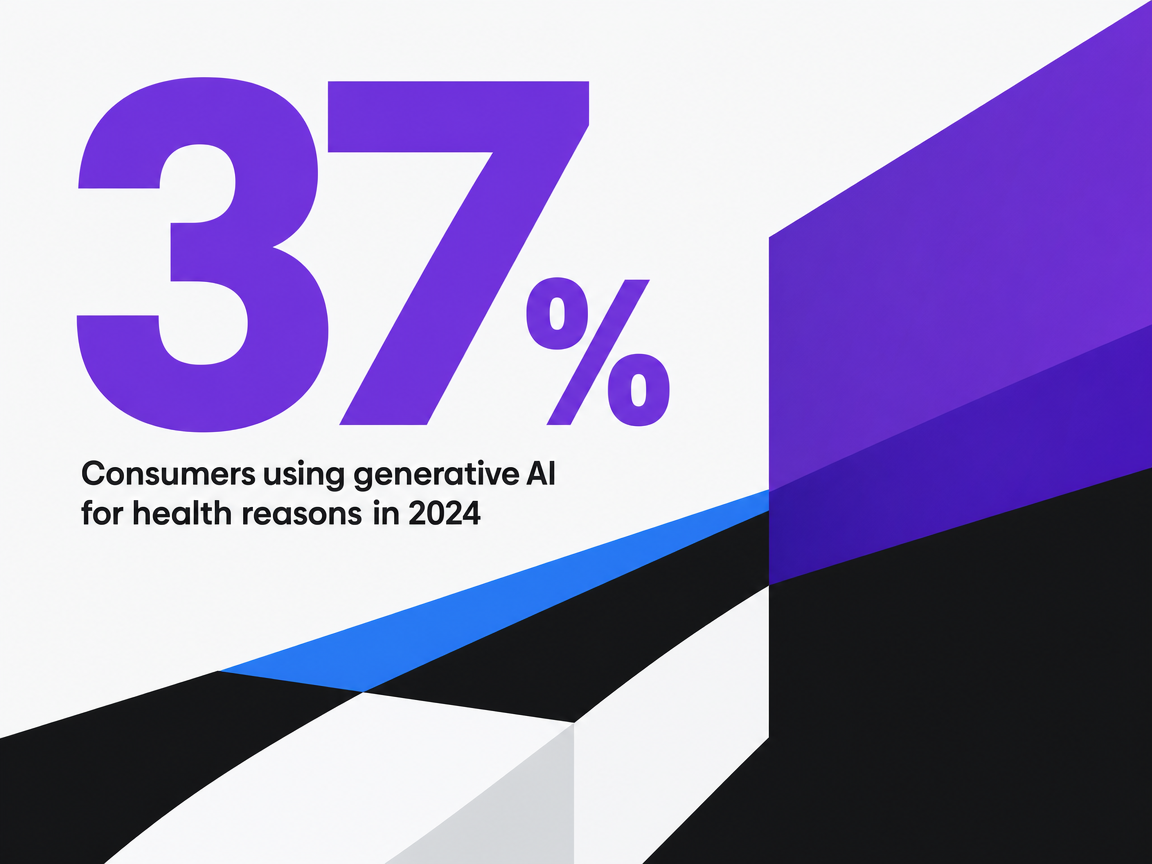 Consumers using generative AI for health reasons in 2024
Consumers using generative AI for health reasons in 2024
Consumers using generative AI for health reasons in 2024
Channel mix decisions for multi-location campaigns
Performance Max, Meta Advantage+, and local SEO at account scale
Paid acquisition for a multi-location group runs on three load-bearing channels: Performance Max, Meta Advantage+, and local SEO. Each rewards account-level structure and punishes per-location fragmentation.
Performance Max compounds in value as the asset library deepens. A 25-location group feeding one campaign 50 headlines, 20 descriptions, 15 video cuts, and metro-tagged location extensions gives the algorithm enough signal to optimize across service lines and geographies. Twenty-five sub-scale campaigns, one per location, starve the model. The structural decision is to run one account-level Performance Max program with asset groups segmented by service line, then let location extensions and feed-driven landing pages handle geographic relevance.
Meta Advantage+ follows the same logic. Advantage+ Shopping and Advantage+ Audience need volume to escape learning phase. A consolidated account-level campaign with creative variants tagged by service line and DMA reaches statistical significance weeks faster than parallel per-location campaigns competing against each other in the same auction.
Local SEO is the inverse problem. Here, per-location specificity is the point. Each Google Business Profile, location landing page, and review surface needs unique content, but the content system that produces them sits at the account level. McKinsey's consumer-led growth research finds that integrated end-to-end experiences capture disproportionate share 2. Local SEO is where that integration becomes visible to the patient mid-search.
Social as engagement, not as a primary acquisition channel
Organic social earns its budget line as a retention and engagement channel, not as a primary acquisition channel. The peer-reviewed literature on patient engagement through social media documents real value in education, peer support, and ongoing relationship-building between visits 8. None of that maps cleanly to booked-appointment economics.
Pew's data on U.S. social media usage shows that YouTube and Facebook still reach the broadest cross-sections of adults, with smaller platforms skewing by age and interest 11. That 2021 baseline is dated, but the directional point holds: reach exists, intent does not. A patient scrolling Facebook is rarely in a booking state.
The operational consequence for a multi-location group is to fund social against engagement metrics — saves, shares, profile follows, video completion — while holding Performance Max, Advantage+, and local SEO accountable for booked appointments and CAC. Misclassifying social as an acquisition channel inflates its budget and obscures where conversions actually originate.
See How Leading Healthcare Groups Coordinate Creative Campaigns Across Locations
Request a walkthrough of unified, AI-driven healthcare advertising execution—covering content, PPC, and backlinks—from a single account-level strategy, purpose-built for complex, multi-site organizations.
Measuring creative against account-level acquisition economics
Creative that cannot be tied to booked appointments and contribution margin does not survive a CFO review. The measurement problem in multi-location healthcare is that most groups report creative performance at the wrong altitude: impressions and engagement per campaign, conversion rates per landing page, CAC per location. Each metric is correct in isolation and misleading in aggregate.
The account-level alternative pins creative to four metrics, measured once across the full footprint:
- Blended CAC by service line, not by location. Orthopedics CAC across 25 markets is the unit a VP of Marketing can act on. Per-location CAC mostly reflects market density, not creative quality.
- Conversion rate from impression to booked appointment. Not form fill, not call. Booked appointment, joined to the EHR or scheduling system so cancellations and no-shows enter the denominator.
- Contribution margin per acquired patient, by service line. A behavioral health intake and a joint replacement intake carry different downstream economics. Creative budget allocation collapses without that distinction.
- Lifetime value to CAC ratio at the system level. A patient who books dermatology and later returns for orthopedics is a single LTV record, not two. Cross-service-line retention is where account-level brand investment earns its return 7.
McKinsey's consumer-led growth analysis finds that integrated end-to-end measurement is what separates groups capturing disproportionate share from those running parallel local programs 2. The practical consequence is governance: one analytics environment, one attribution model, one weekly review that ranks creative against booked-appointment economics rather than channel-level vanity metrics. Creative that survives that review gets more budget. Creative that does not gets cut, regardless of which market produced it.
An account-level operating model: brief once, execute everywhere
The sections above describe components. The operating model is what ties them together so a 25-location group runs one program instead of twenty-five.
Five elements define the model in practice:
- One brief, one brand source of truth. Strategy, claim substantiation, clinician sourcing, and brand system live in a single repository. Every market draws from it. No parallel interpretations.
- Compliance embedded upstream. HIPAA authorization boundaries 5, FTC substantiation files 6, and AMA truthfulness checks 3enter the brief as inputs, not as final-stage gates.
- Localization as transformation, not reproduction. DMA, service-line, and clinician variants are layers applied to a master asset, produced once and propagated programmatically across Performance Max asset groups, Meta Advantage+ creative sets, and local SEO landing pages.
- One measurement environment. Booked-appointment CAC by service line, contribution margin per patient, and system-level LTV-to-CAC ratio reviewed weekly across the full footprint. McKinsey's consumer-led growth analysis ties this integrated measurement directly to disproportionate share capture 2.
- One execution cycle. Brief, produce, localize, ship, measure — running on a single cadence instead of N agency calendars.
Vectoron's platform is built around this account-level model for multi-location healthcare operators that have outgrown per-location retainers. The decision a VP of Marketing is weighing is not which agency to hire next. It is whether the next ten locations will be added to one operating system or to ten more coordination problems.
Frequently Asked Questions
References
- 1.Marketing in healthcare: Improving the consumer experience.
- 2.Driving healthcare growth with a consumer-led strategy.
- 3.Advertising & Publicity | AMA Code of Medical Ethics.
- 4.The Code of Medical Ethics of the American Medical Association.
- 5.Marketing | HHS.gov.
- 6.Health Products Compliance Guidance.
- 7.Systematic review of health branding: growth of a promising practice.
- 8.Patient Education and Engagement through Social Media.
- 9.Building and maintaining health care consumers' trust in generative AI.
- 10.2025 Connected Consumer: Innovation with trust.
- 11.Social Media Use in 2021.