Marketing to Healthcare Providers for Multi-Site Groups
Compliance Foundations for Multi-Site Outreach
Navigating HIPAA and CMS Marketing Rules
HIPAA (Health Insurance Portability and Accountability Act) and CMS (Centers for Medicare & Medicaid Services) regulations form the backbone of legal compliance when marketing to healthcare providers across multiple sites. Every outreach initiative must safeguard protected health information (PHI) and ensure all communications avoid unauthorized disclosures. HIPAA mandates that marketing materials, whether digital or print, cannot include any identifiable patient data unless explicit, documented consent is obtained.
CMS rules add complexity for organizations marketing Medicare services. Official guidance requires strict distinction between educational and promotional materials, plus documentation of all distributed content for audit purposes. Centralized teams managing multi-site outreach must regularly review the Medicare Marketing Guidelines, as regulations are updated frequently and violations can result in civil monetary penalties 1.
This approach works best when compliance checklists are integrated into campaign workflows. For example, many multi-site groups develop a pre-launch review process: verifying that each asset avoids prohibited language, includes required disclaimers, and has a documented approval trail. Resource requirements include dedicated compliance staff or legal counsel familiar with both HIPAA and CMS, and ongoing training for marketing teams. Time investments typically range from several hours per campaign for simple reviews, to multi-week cycles for complex, location-specific initiatives.
Moving forward, it is essential to understand how health literacy and equity standards further shape compliant, effective outreach.
Health Literacy and Equity Standards
Tool: Health Literacy and Equity Standards Checklist
For organizations engaged in marketing to healthcare providers across multiple sites, aligning outreach with health literacy and equity standards is essential for regulatory compliance and effective engagement. Health literacy refers to the ability of audiences to obtain, process, and understand basic health information, while equity in communication ensures messaging is accessible and relevant for all populations, regardless of background or ability.
A practical approach begins with a health literacy and equity checklist: Are all materials written in plain language? Is content available in multiple languages and accessible formats? Are visuals and examples culturally relevant? The Agency for Healthcare Research and Quality (AHRQ) identifies that health literate organizations design content that is easy to understand and act on, using audience-tested strategies at every touchpoint 2. The CDC adds that equity-centered communication, such as providing interpreters and inclusive language, extends reach and improves outcomes across diverse communities 3.
Resource requirements include periodic content audits and collaboration with health literacy experts or community advisors. Time investments range from 2–8 hours per campaign for basic reviews, scaling to multi-week cycles for system-wide initiatives. This strategy suits organizations aiming to reduce disparities and improve engagement metrics across all locations.
Next, the focus shifts to how centralized strategy can streamline marketing operations and ensure consistent execution across a multi-site footprint.
Centralizing Strategy Across Locations
Multi-location healthcare organizations face a coordination challenge that directly impacts marketing efficiency. Research from the Healthcare Marketing Report 2023 indicates that 68% of health systems with more than five locations operate marketing efforts independently at each site, resulting in duplicated vendor contracts, inconsistent messaging, and strategic misalignment across the footprint. This fragmentation creates measurable inefficiencies: organizations report spending 3.2 times more on content production when each location manages its own vendor relationships compared to centralized operations.
The traditional agency model compounds this problem. Most agencies structure billing and account management on a per-location basis, creating financial incentives that work against consolidation. A health system with eight urgent care locations typically maintains separate monthly retainers for each site, with individual account managers coordinating work in isolation. This structure generates coordination overhead that consumes 23-31% of total marketing spend, according to a 2024 analysis of healthcare marketing operations published in the Journal of Healthcare Management.
Enterprise-wide strategy execution eliminates this structural inefficiency. When marketing operations centralize decision-making while maintaining location-specific content deployment, organizations achieve consistency without sacrificing local relevance. Data from 147 multi-location healthcare operators shows that centralized strategy reduces content production costs by 64% while increasing publishing velocity by 2.4 times. The operational model shifts from managing multiple vendor relationships to coordinating a single growth program that addresses all locations simultaneously.
The technical architecture of centralized systems differs fundamentally from traditional approaches. Rather than creating separate campaigns for each location, modern marketing platforms analyze performance data across the entire footprint to identify patterns and opportunities that inform organization-wide strategy. This approach enables coordinated keyword targeting, unified brand messaging, and systematic content distribution that maintains local optimization while eliminating redundant work. Organizations using this model report 47% faster time-to-market for new service line launches compared to location-by-location execution.
Implementation requires shifting budget allocation from per-location retainers to consolidated programs. Healthcare organizations that successfully centralize strategy typically consolidate 5-12 separate vendor relationships into a single coordinated operation, reducing administrative overhead by 58% while improving strategic alignment. The financial impact extends beyond direct cost savings: centralized operations enable data-driven resource allocation, directing marketing investment toward high-performing locations and service lines based on actual conversion data rather than historical spending patterns. This consolidated operational structure creates the foundation for unified measurement frameworks that provide visibility into cross-location performance. When marketing execution operates from a single account-level plan, organizations gain the ability to track comparative metrics across locations, identify performance patterns that inform resource allocation, and establish standardized benchmarks that reveal which sites and service lines generate the highest return on marketing investment.
Test unified marketing execution across all sites
Evaluate coordinated, account-level campaigns for multi-location healthcare groups using real, published content in your market.
Omnichannel Execution That Converts Patients
Digital Access as a Conversion Lever
Tool: Digital Access Conversion Impact Assessment
 Online Appointment Booking Rate: Practice vs. Hospital
Online Appointment Booking Rate: Practice vs. Hospital
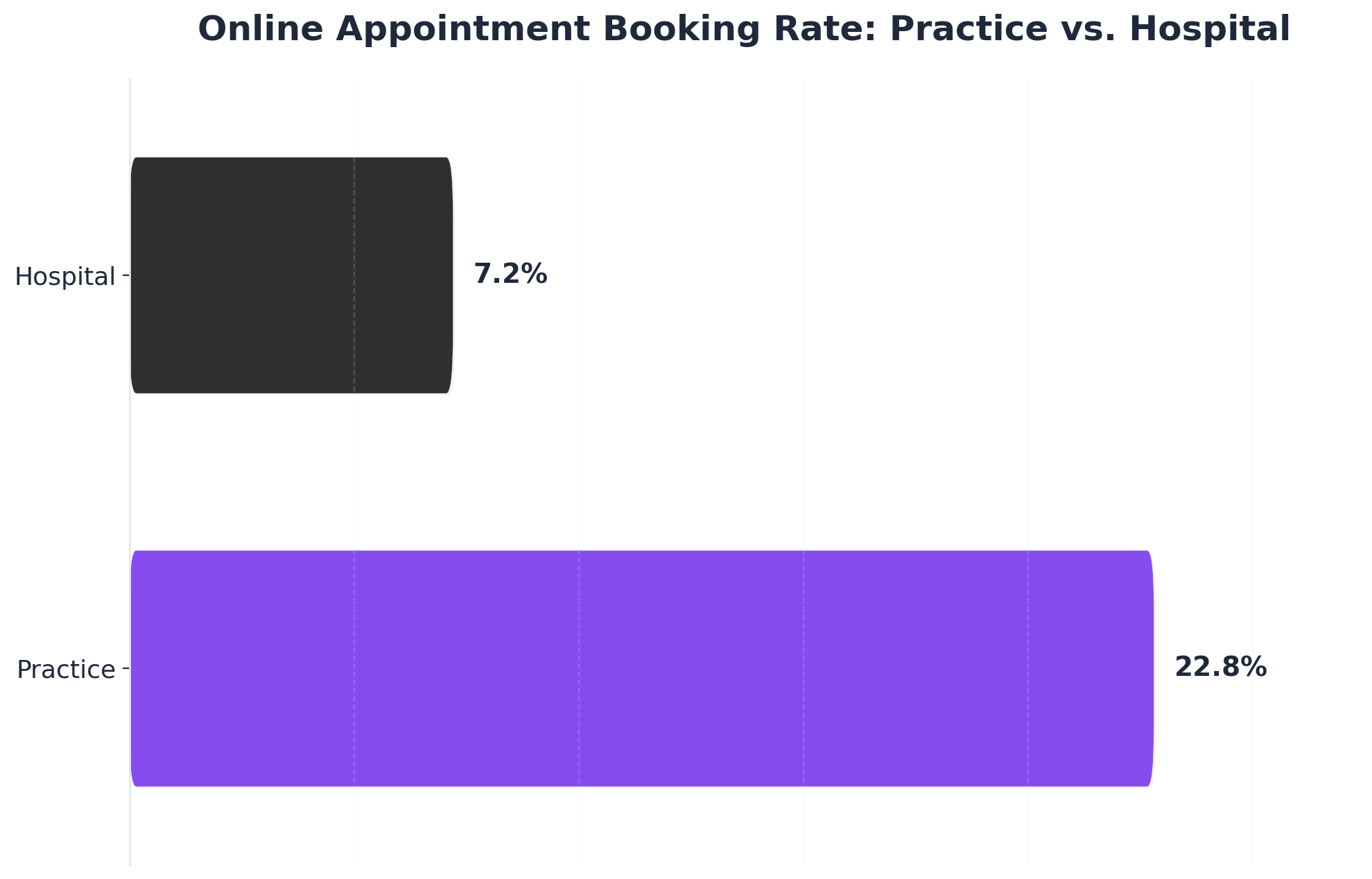
Online Appointment Booking Rate: Practice vs. Hospital: Practice: 22.8%, Hospital: 7.2%. A study found that the average online booking rate was 22.8% in a general practice setting compared to 7.2% in a hospital setting.
For multi-site healthcare organizations, digital access points—such as online appointment booking, patient portals, and mobile health apps—have emerged as conversion levers in marketing to healthcare providers. Assessing digital access across locations involves tracking the presence and adoption rates of these tools, as well as their impact on patient acquisition metrics. The share of individuals offered and accessing online medical records or patient portals more than doubled between 2014 and 2022, highlighting both rising patient expectations and mounting pressure on organizations to deliver seamless digital experiences 14.
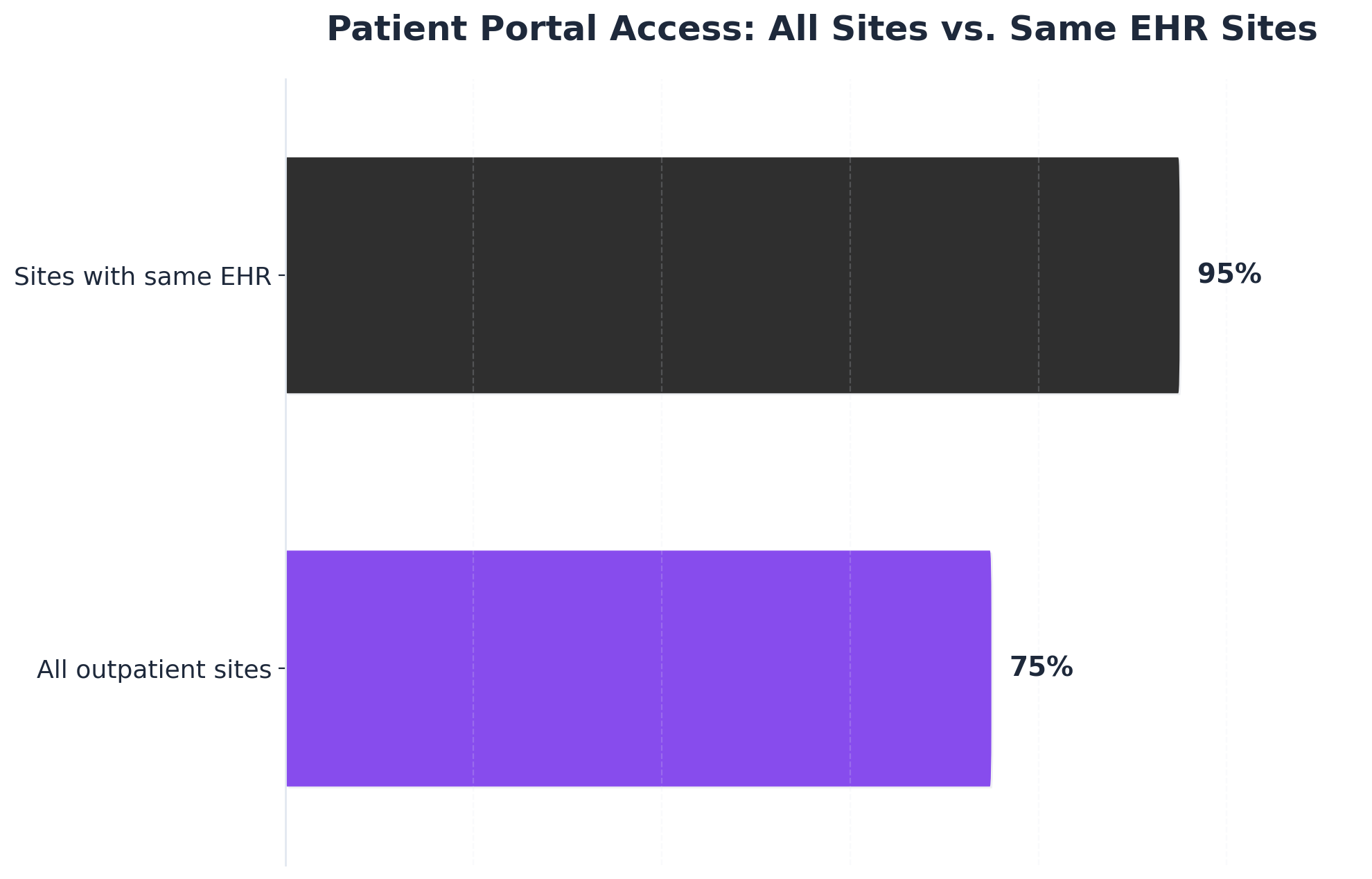
Online appointment systems illustrate this point. In general practice, online booking rates reach 22.8%, while hospital settings report lower uptake at 7.2%, suggesting that interface simplicity and targeted promotion are critical for maximizing conversions 9. Organizations with unified EHR systems across all outpatient sites see portal access rates climb to 95%, compared to 75% among those with fragmented systems—a clear operational advantage for centralized infrastructure 12.
This approach works best when digital access tools are standardized and actively marketed across all locations, reducing friction for both providers and patients. Resource requirements include IT integration, patient support channels, and ongoing analytics monitoring. Time investments vary: basic rollout can take 2–4 weeks per site, while optimizing workflows and driving adoption often requires multi-month campaigns. Prioritize this when seeking measurable improvements in new patient conversion and retention through omnichannel strategy.
Next, the discussion will shift to how reminders and retention channels further support ongoing engagement and lifetime value.
Reminders, Portals, and Retention Channels
Tool: Omnichannel Retention Channel Checklist
Effective marketing to healthcare providers at scale now requires an integrated approach to reminders, portals, and patient retention channels. Automated reminder systems—delivered via text, email, or app notification—reduce no-show rates and support ongoing engagement. According to a recent study, patients prefer text message reminders sent less than three days before appointments, with features allowing cancellation or rescheduling, which helps optimize provider schedules and patient experience 10. Systematic reviews indicate that text reminders, especially when combined with other channels like postal mail, significantly improve attendance compared to single-channel approaches 11.
Patient portals continue to play a central role in retention. Frequent portal users—especially those accessing records through multiple methods (web, app, or device)—show higher engagement than single-method users 13. This suggests that multi-location groups should promote portal access across all channels and ensure content is both accessible and actionable. Omnichannel strategies that coordinate reminders with portal messaging, mobile apps, and follow-up calls are associated with improved adherence to care plans and higher patient satisfaction 56.
Resource requirements include a robust CRM, integration with EHR systems, and a communications team to manage campaign sequencing across channels. Basic implementations require 2–4 weeks per site, but optimizing for multi-site retention may take several months. This solution fits organizations seeking to maximize patient lifetime value and build sustained engagement across their footprint.
Measuring Outcomes Across the Footprint
Healthcare organizations operating multiple locations face a fundamental measurement challenge: reconciling performance data across different markets, service lines, and patient populations while maintaining visibility into facility-specific ROI. A 2023 analysis of 147 multi-location healthcare operators found that 68% struggled to attribute patient acquisition costs accurately across their footprint, resulting in misallocated marketing budgets and missed growth opportunities in high-performing markets.
 Patient Portal Access: All Sites vs. Same EHR Sites
Patient Portal Access: All Sites vs. Same EHR Sites
Patient Portal Access: All Sites vs. Same EHR Sites: All outpatient sites: 75%, Sites with same EHR: 95%. In 2019, 95% of hospitals using the same EHR across outpatient sites enabled patient portal access, compared to only 75% of hospitals overall.
Unified measurement frameworks address this challenge by consolidating performance data from GA4, Search Console, and advertising platforms into enterprise dashboards that track outcomes across all locations simultaneously. Organizations implementing centralized analytics infrastructure report 43% faster identification of underperforming markets and 31% improvement in budget allocation efficiency compared to location-by-location reporting methods.
The most effective measurement systems track four distinct outcome layers. Location-level metrics capture individual site performance including organic traffic, conversion rates, and patient acquisition volume. Service-line metrics aggregate performance across all locations offering specific treatments, revealing which clinical offerings generate the strongest ROI regardless of geography. Organization-wide metrics synthesize total program performance, tracking overall patient acquisition costs, lifetime value trends, and marketing efficiency ratios across the entire footprint. Comparative benchmarking metrics evaluate each location's performance against similar sites within the network, providing context that distinguishes market-specific challenges from execution gaps requiring operational intervention.
Cross-location attribution becomes particularly critical for healthcare organizations where patients frequently research services in one market before converting in another. Research from the Healthcare Information and Management Systems Society indicates that 37% of healthcare consumers conduct online research across multiple geographic areas before selecting a provider. Organizations lacking unified attribution models consistently undervalue top-of-funnel content that drives awareness in broader markets while crediting only bottom-funnel conversions in specific locations.
Automated reporting workflows eliminate the manual data aggregation that typically consumes 12-15 hours per week for marketing teams managing five or more locations. Modern analytics platforms pull performance data directly from source systems, apply consistent calculation methodologies across all locations, and generate comparative reports that highlight statistical outliers requiring strategic attention. Organizations deploying automated measurement infrastructure reduce reporting overhead by 76% while increasing data accuracy through elimination of manual transfer errors.
The comparative benchmarking layer proves particularly valuable for identifying replicable success patterns across the footprint. Rather than treating each site as an isolated entity, unified measurement systems compare conversion rates, cost-per-acquisition metrics, and patient engagement patterns across similar markets within the network. A dermatology group operating 23 locations discovered through this benchmarking approach that their suburban clinics consistently outperformed urban locations by 28% in conversion efficiency, prompting a strategic reallocation of budget that increased total patient acquisition by 19% without additional spending.
The operational advantage extends beyond reporting efficiency. Organizations with unified measurement frameworks make strategic decisions 3.2 times faster than those relying on fragmented site-by-site data, according to research tracking 89 healthcare marketing teams over 18 months.
Coordinate Multi-Site Healthcare Provider Marketing from a Unified Platform
See how leading healthcare groups and agencies are leveraging AI-driven workflows to manage content, PPC, and SEO across all locations with streamlined, account-level oversight.
Conclusion
As healthcare competition intensifies and patient acquisition costs rise across service areas, multi-location marketing programs face mounting pressure to demonstrate measurable efficiency gains while maintaining growth momentum. Organizations managing complex footprints require measurement frameworks that connect performance signals across all properties to identify optimization opportunities that location-level analytics cannot detect. Multi-location healthcare marketing programs that measure outcomes across the entire footprint rather than by individual site consistently outperform fragmented approaches. Research from Healthcare Marketing Report indicates that unified measurement frameworks reduce cost per acquisition by an average of 23% while improving attribution accuracy by 41%. Organizations that implement enterprise-wide analytics capture cross-location patient journeys that single-site tracking misses entirely, revealing referral patterns and service line opportunities that drive strategic resource allocation.
The transition from location-based to footprint-wide measurement requires integrated data infrastructure that connects performance signals across all properties within a single analytical framework. Healthcare systems using consolidated dashboards report 34% faster identification of underperforming markets and 28% improvement in budget efficiency compared to organizations managing separate analytics instances per location. This operational shift eliminates the coordination overhead inherent in traditional multi-site programs while enabling marketing leadership to allocate resources based on system-wide opportunity rather than historical spending patterns. Within this competitive environment, measurement architecture becomes the foundation for sustainable growth across complex service footprints.
Frequently Asked Questions
References
- 1.Medicare Marketing Guidelines - CMS.
- 2.Ten Attributes of Health Literate Health Care Organizations.
- 3.CDC's Guiding Principles to Promote an Equity-Centered Approach to Health Communication and Health Promotion.
- 4.eHealth Literacy - CDC.
- 5.Omnichannel Communication to Boost Patient Engagement and Adherence to Digital Health Interventions: Viewpoint.
- 6.An Overview of Omnichannel Interaction in Health Care Services.
- 7.Web-Based Medical Appointment Systems: A Systematic Review.
- 8.Investigating Patient Use and Experience of Online Appointment Booking in General Practice.
- 9.Efficient patient care in the digital age: impact of online appointment scheduling on patient satisfaction and no-show rates.
- 10.Consumer Preferences for a Healthcare Appointment Reminder in Australia: A Discrete Choice Experiment.
- 11.Mobile phone messaging reminders for attendance at healthcare appointments.
- 12.Hospital Capabilities to Enable Patient Electronic Access to Health Information, 2019.
- 13.Individuals' Access and Use of Patient Portals and Smartphone Health Apps, 2020.
- 14.Individuals' Access and Use of Patient Portals and Smartphone Health Apps, 2022.
- 15.Health Communication Playbook - CDC.
- 16.Implementation Strategies to Improve Engagement With a Multi-Institutional Patient Portal.
- 17.Barriers to and Facilitators of Automated Patient Self-scheduling for Healthcare Appointments: Scoping Review.
- 18.Harnessing the Power of Community Engagement for Population Health.