Key Takeaways
- Robotic automation in healthcare spans three categories with distinct scaling profiles: sublinear RPA for back-office work, compounding AI digital workforce tools for clinical-adjacent tasks, and capital-bound surgical robotics.
- Revenue cycle automation is the strongest first move for multi-site operators, with 74% of hospitals already running some form of RCM automation and 46% using AI within it 2.
- Surgical robotics should be evaluated as a service-line differentiator, not a cost-saving lever, since direct hospital costs often exceed laparoscopic alternatives without a reimbursement premium 6, 12.
- Sequence investments from standardized back-office RPA, to clinical-adjacent AI paired with redesigned roles, to capital robotics tied to case-mix and competitive strategy, supported by unified governance.
Three Automation Categories, Three Scaling Profiles
The global health workforce faces a projected shortage of 18 million workers by 2030 13. McKinsey Health Institute suggests closing this gap could reduce global disease burden by 7% and add $1.1 trillion to GDP 16. Automation is a key strategy when headcount cannot meet demand. However, "robotic automation in healthcare" encompasses three distinct technologies, each with unique scaling characteristics.
Robotic process automation (RPA) handles structured back-office tasks such as claims processing, eligibility checks, scheduling, and EMR monitoring 9. Once standardized, an RPA bot can operate across multiple sites with minimal additional cost. AI digital workforce tools, including predictive models, conversational agents, and ambient documentation, address clinical-adjacent areas where decisions are more complex but offer significant capacity gains. For instance, predictive AI adoption in U.S. hospitals increased from 66% to 71% between 2023 and 2024 3. Physical robotics, primarily surgical platforms, represents a different category. Each unit is a capital investment, tied to specific procedures, and often incurs higher direct costs than laparoscopic alternatives without corresponding reimbursement 6, 12.
Conflating these technologies leads to misallocated capital. Operators who differentiate by scaling profile—sublinear for RPA, compounding for AI digital workforce, and capital-bound for surgical robots—can optimize their investments. The following sections explore each layer and propose a sequencing framework for multi-site deployment.
The Back-Office Layer: RPA Where Standardization Already Exists
Revenue Cycle as the Proven Anchor Use Case
Revenue cycle management (RCM) is a mature area for back-office automation. American Hospital Association data indicates that 46% of hospitals and health systems use AI in their RCM operations, and 74% have deployed some form of revenue-cycle automation, including rules-based bots, machine learning, or combined AI/RPA stacks 2. This level of penetration is unmatched in other operational domains within U.S. hospitals.
The structural nature of RCM tasks drives this adoption. Eligibility verification, prior authorization checks, claim scrubbing, denial routing, payment posting, and patient statement generation are high-volume, rules-driven, and largely consistent across different sites. A bot performing eligibility checks at one clinic can perform the same function at many others. Generative AI further extends automation into tasks requiring human judgment, such as drafting appeals, summarizing documentation for coders, and triaging denials by root cause 2.
For multi-site operators, RCM offers a clear economic case due to three factors:
- work units are transactions with measurable cycle times,
- errors are visible in denial rates and days in A/R, and
- staffing models are often centralized, reducing the site-specific change management burden common in clinical deployments.
The AHA notes that generative models require guardrails and human validation to prevent bias and errors in payment integrity 2. This is a governance consideration, not a barrier to implementation.
EMR Monitoring and Cross-Site Uptime
A high-leverage RPA use case, often less visible, is EMR monitoring. A 2025 study describes RPA bots that simulate end-user interactions to continuously test critical EHR functions, detect failures, and provide operational metrics without altering core systems 11. These bots log in, navigate scheduling, open charts, place orders, and report back. This proactive monitoring alerts operations to issues before clinicians are impacted.
This is particularly valuable for multi-site operators using a shared EMR tenant across various locations like clinics, ambulatory surgery centers, and imaging centers. A configuration change can affect one site differently from another. Manual testing across such a footprint is impractical, whereas synthetic transaction bots scale efficiently with near-zero marginal cost per additional site once the script library is established.
The primary constraint is brittleness. RPA-based monitoring relies on stable user interfaces and requires ongoing maintenance when vendors update UIs 11. Operators who manage their bot library as production infrastructure—with versioning, ownership, and a maintenance budget—can realize uptime benefits. Neglecting maintenance leads to silent bot failures and loss of the early warning system.
Where RPA Stalls: Process Variance Across Sites
RPA's effectiveness is directly tied to process standardization. A HICSS analysis of healthcare RPA case studies concluded that bots deliver significant gains in well-structured workflows, but benefits are limited when underlying processes are highly variable or poorly standardized 10. For multi-location operators, this means if Site A uses fax for referrals, Site B uses a web form, and Site C has a custom EMR workflow, a single bot cannot cover all three without costly, site-specific customization.
The solution is upstream: process standardization must precede automation. Deploying RPA into varied processes results in a portfolio of fragile bots that struggle with local exceptions. The same study also cautions against framing RPA solely as a headcount reduction strategy, as this can hinder staff acceptance and adoption. Benefits framed around error reduction and redeploying staff to higher-value work are more effective 10.
Therefore, the operational sequence should be inverted from typical vendor pitches. First, identify and automate the three workflows that are already standardized across all sites. Use the resulting savings to fund the standardization work necessary for automating the next tier of processes. Skipping standardization is a common reason why RPA programs fail to scale beyond pilots.
The AI Digital Workforce Layer: Clinical-Adjacent Capacity
Predictive AI Adoption Has Moved Past Pilot Stage
Predictive AI is becoming mainstream in U.S. hospitals. Office of the National Coordinator data shows overall hospital adoption rose from 66% in 2023 to 71% in 2024 3. The fastest-growing operational use cases—billing procedure automation (36% to 61%) and scheduling facilitation (51% to 67%)—are those that compound across multi-site footprints 3. These are not clinical decisions but pattern recognition problems with measurable error rates, explaining their rapid AI penetration compared to direct clinical applications.
The compounding effect is significant. A scheduling model trained on one site's no-show patterns, payer mix, and provider templates can be retrained for a new site's data in weeks, rather than rebuilt. Each additional location contributes training data without a proportional increase in software cost. A 2024 review highlights that combining AI with bot infrastructure enables systems to handle unstructured inputs and probabilistic decisions beyond the scope of pure rules-based automation, expanding the range of automatable work 9.
The ONC brief also notes that as AI adoption increased, so did hospital focus on performance monitoring, bias mitigation, and oversight frameworks 3. Operators should view the 2023-2024 adoption deltas as indicators of validated use cases versus those still carrying significant model risk.
Recovering Nursing and ICU Capacity
Clinical-adjacent automation offers quantifiable value, particularly in nursing. A McKinsey analysis of U.S. inpatient nursing workloads estimates that 10-20% of a typical 12-hour shift could be optimized through technology, and with broader care-model redesign, time savings could reach 15-30% 15. This efficiency could close the projected nursing workforce gap by up to 300,000 inpatient nurses 15, representing a tangible capacity gain for healthcare organizations.
Intensive care units (ICUs) show a similar pattern. A 2025 study on AI interventions in ICUs found that well-designed tools reduce stress, optimize workflows, and enable clinicians to manage larger patient loads safely, directly addressing staffing crises that limit ICU throughput 8. Ambient documentation, early-warning systems for deterioration, and automated handoff summaries each save minutes per shift, accumulating into significant hours across a unit.
Successful implementation is crucial. McKinsey's work emphasizes that time savings depend on implementation quality and frontline engagement, warning that poorly designed automation can exacerbate burnout 15. The ICU study similarly notes that poorly designed AI systems can increase cognitive load or introduce new safety risks if usability and oversight are inadequate 8. Capacity recovery is achieved through effective deployment, not merely through purchase.
The Work-Shift Risk Most Vendors Ignore
Vendors often present AI digital workforce tools as a direct reduction in workload. However, qualitative evidence suggests a more complex reality. A 2023 study of an autonomous clinical conversational assistant revealed mixed staff experiences. While some clinicians reported reduced administrative load and improved workflow, others experienced increased complexity and new demands, such as more triage decisions, exception handling, and system supervision 5.
This pattern indicates a work shift rather than work disappearance. When an AI agent handles the routine 70% of a task, the remaining 30% becomes a higher-density workload for the human in the loop. If staffing models, role definitions, and shift designs are not adjusted, the apparent capacity gain can manifest as fatigue and frustration instead of increased throughput 5. The American Hospital Association reinforces this, stating that AI-driven workforce transformation requires deliberate engagement with staff to prevent resistance and align deployments with strategic goals 1.
The operational implication is clear: every clinical-adjacent AI deployment should be paired with a redesigned role specification, an updated shift composition, and a measurement plan that tracks workload distribution alongside cycle-time savings. Neglecting this step can lead to capacity gains eroding within two quarters.
Test Robotic Automation Impact on Healthcare Marketing
Experience end-to-end automated marketing execution at scale across your locations during your free trial period.
The Physical Robotics Layer: Surgical Systems as Strategic, Not Cost-Saving
Physical robotics occupies the opposite end of the scaling spectrum from RPA. Each surgical platform is a capital asset linked to a specific service line, procedure mix, and operating room. There is no compounding effect across sites; adding a robot at a second hospital requires purchasing another unit, training a new team, and amortizing additional instrument and service contracts. The financial model resembles opening a new cath lab more than deploying a software bot.
The financial case is often weaker than marketing suggests. A 2024 Baylor College of Medicine review found that robotic procedures are frequently more costly for hospitals than traditional laparoscopic surgery, with insurer reimbursement often lower despite the higher cost 6. A 2023 review across specialties reached a similar conclusion: robotic approaches in urologic surgery, for example, are associated with shorter lengths of stay but higher direct hospital costs than open procedures, and current payment models generally do not offer a premium for robotic techniques 12. While shorter lengths of stay and fewer complications are clinical benefits, they do not inherently close the margin gap.
The strategic case for robotic platforms is more compelling. They serve as service-line differentiators in competitive markets, attract surgeons trained on the technology, and drive patient volume in specialties where patients actively seek robotic options. Decisions regarding additional units should be based on case-mix, surgeon pipeline, and local competition, rather than an RPA-style efficiency model. The financial realities review explicitly states that many robotic programs struggle to achieve positive margins without strict case selection and operational optimization 6. These programs should be managed as strategic assets with disciplined utilization targets, not as cost-saving levers.
Comparing the Three Layers Side by Side
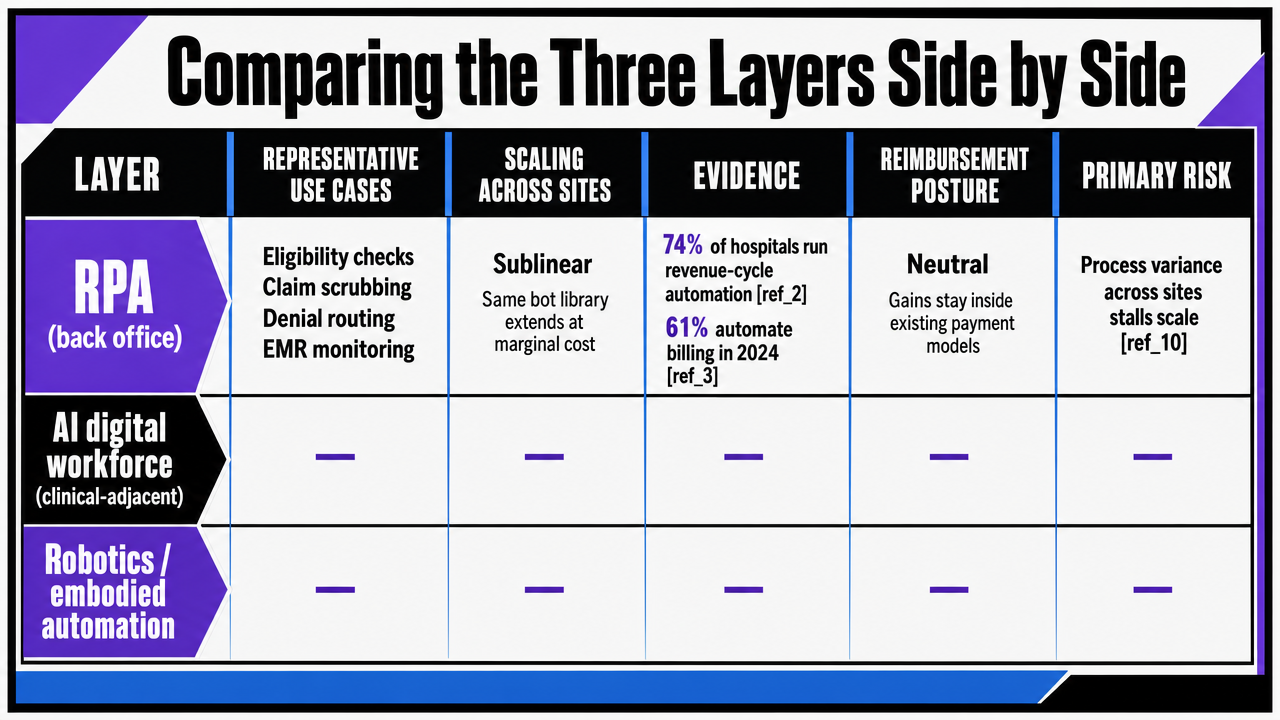
The three automation layers exhibit distinct scaling math, evidence bases, and reimbursement implications. The table below summarizes these characteristics to help operators evaluate each layer without conflation.
| Layer | Representative use cases | Scaling behavior across sites | Sourced evidence of capacity or adoption | Reimbursement posture | Primary risk |
|---|---|---|---|---|---|
| RPA (back office) | Eligibility checks, claim scrubbing, denial routing, EMR monitoring | Sublinear; same bot library extends to additional sites at marginal cost | 74% of hospitals run some form of revenue-cycle automation 2; 61% automate billing procedures in 2024 3 | Neutral; cycle-time and accuracy gains accrue inside existing payment models | Process variance across sites stalls scale 10 |
| AI digital workforce (clinical-adjacent) | Predictive scheduling, ambient documentation, ICU early-warning, conversational assistants | Compounding; models improve as each site adds training data | 46% of hospitals use AI in RCM 2; 15-30% of nursing time recoverable via tech and redesign 15 | Positive on throughput; supports larger patient loads without proportional hiring 8 | Work shift onto remaining staff if roles are not redesigned 5 |
| Physical robotics (surgical) | Robotic-assisted urologic, gynecologic, and general surgery | Capital-bound; each site requires a separate platform, team, and service contract | Shorter LOS and fewer complications versus open procedures 12 | Often unfavorable; higher direct cost without a reimbursement premium 6, 12 | Margin erosion without strict case selection 6 |
Reading across the rows, the operational takeaway is clear. RPA and AI digital workforce investments compound across a footprint, absorbing volume without proportional cost. Surgical robotics justifies its investment through case-mix strategy, not unit economics.
 Visualize the three-layer comparison table that is central to the article's framework, showing scaling profiles, evidence, and reimbursement posture side by side
Visualize the three-layer comparison table that is central to the article's framework, showing scaling profiles, evidence, and reimbursement posture side by side
See How Leading Healthcare Operators Automate Multi-Site Marketing at Scale
Connect with experts to evaluate AI-driven marketing automation proven to reduce coordination costs and streamline content production for complex, multi-location healthcare networks.
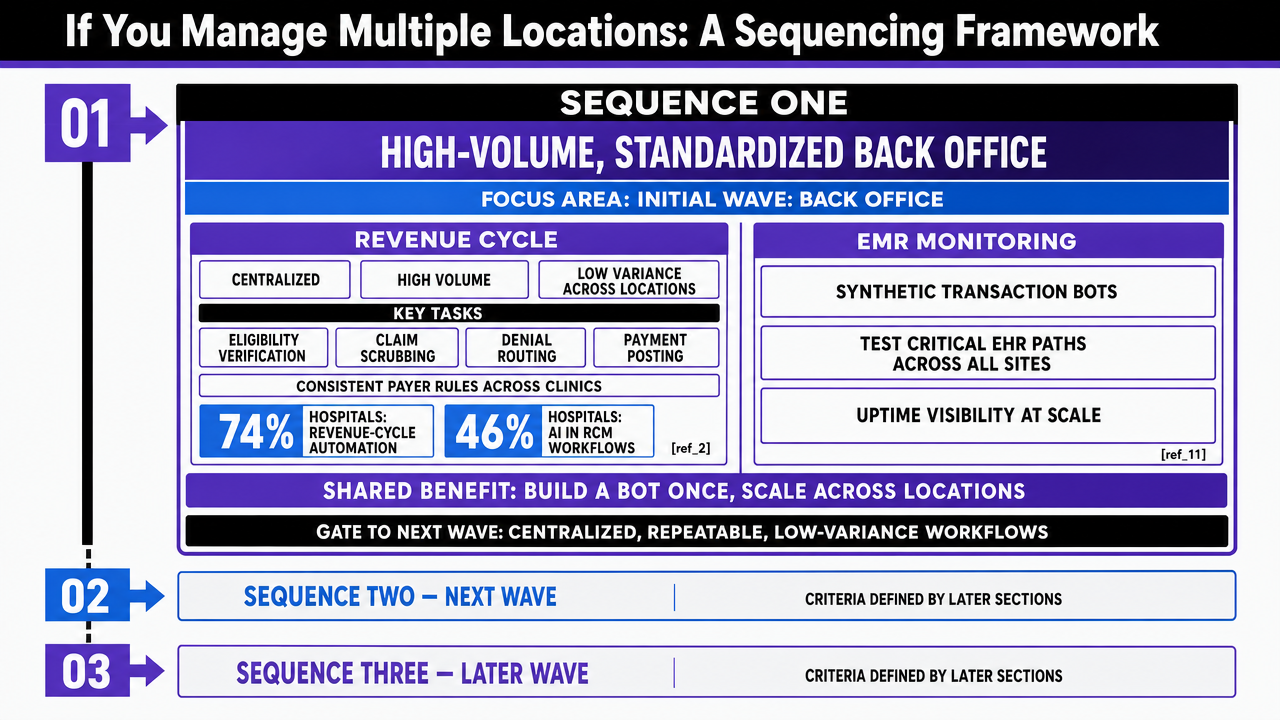
If You Manage Multiple Locations: A Sequencing Framework
Sequence One: High-Volume, Standardized Back Office
For operators managing multiple sites, the initial wave of automation should focus on the back office. Revenue cycle is an ideal starting point due to its centralized nature, high volume, and low process variance across locations. Tasks like eligibility verification, claim scrubbing, denial routing, and payment posting follow consistent payer rules regardless of the clinic. This explains why 74% of hospitals have deployed some form of revenue-cycle automation, and 46% specifically use AI in RCM workflows 2.
EMR monitoring should be included in this first wave alongside RCM. Synthetic transaction bots that test critical EHR paths across all sites provide uptime visibility that manual QA teams cannot match at scale 11. Both use cases share the benefit of building a bot library once and extending it to new locations at marginal cost. The ROI curve improves with footprint size, which is critical for multi-site operators.
Fund standardization work from the savings generated by this first wave before proceeding. RPA programs that skip this step often accumulate site-specific exceptions and fail to advance to subsequent sequences 10.
Sequence Two: Clinical-Adjacent AI Where Variance Is Bounded
The second sequence shifts to clinical-adjacent areas, but only where process variance is contained. Predictive scheduling is a prime candidate, with hospital adoption of AI-assisted scheduling rising from 51% to 67% in one year, and billing-adjacent automation from 36% to 61% 3. These use cases rely on data structures that are similar across sites, such as appointment slots, no-show histories, and payer mix. A model trained at one location can be adapted to another with retraining, not complete rebuilding.
Ambient documentation and ICU early-warning tools follow. Literature on ICU interventions shows these tools enable clinicians to safely manage larger patient loads without proportional staff growth 8. McKinsey's nursing workload analysis quantifies a potential 15-30% recovery of shift time when technology is combined with care-model redesign 15.
Each deployment in this sequence must be accompanied by a redesigned role specification. The conversational-assistant study explicitly states that automation can increase work density for humans in the loop rather than reducing overall workload 5. Measure workload distribution alongside cycle time to prevent capacity gains from dissipating.
Sequence Three: Capital-Bound Robotics Tied to Service-Line Strategy
Physical robotics is the final layer and should only be introduced based on a service-line strategy, never as a cost-saving measure. Each platform is a capital decision linked to a specific OR, surgeon pipeline, and procedure mix. Financial evidence consistently shows that robotic procedures typically incur higher direct hospital costs than laparoscopic alternatives, and reimbursement often does not provide a premium for the robotic technique 6, 12. While shorter lengths of stay and fewer complications are real benefits, they alone do not close the margin gap 12.
When evaluating additional units, operators should consider three factors:
- case-mix density at the candidate site,
- surgeon recruitment pressure in the relevant specialty, and
- competitive positioning in the local market.
If at least two of these factors justify the platform, the program can function as a strategic differentiator with disciplined utilization targets. If only one factor applies, defer the investment. Hospitals that underinvest in digital solutions relative to their challenges often do so by prioritizing capital robotics over compounding software layers 14.
 Visualize the three-sequence deployment framework described in the section, showing the order, focus, and gating criteria for each wave
Visualize the three-sequence deployment framework described in the section, showing the order, focus, and gating criteria for each wave
Governance, Change Management, and the Underinvestment Trap
Three critical execution risks can undermine even well-planned automation programs. The first is governance. Office of the National Coordinator data shows that hospital attention to performance monitoring, bias mitigation, and oversight frameworks increased with predictive AI adoption between 2023 and 2024 3. This correlation is crucial: models drift, payer rules change, and unmonitored bots can cause silent errors that surface as denial rates or patient safety issues months later. Multi-site operators require a unified oversight layer with versioning, performance thresholds, and clear ownership, rather than a fragmented, per-site approach.
The second risk is change management. The American Hospital Association emphasizes that workforce transformation requires deliberate engagement with staff to prevent resistance and align deployments with strategic goals 1. The conversational-assistant study further illustrates this point: automation implemented without role redesign often shifts work density onto the humans remaining in the loop, rather than reducing overall workload 5. Capacity gains projected at purchase can be lost during deployment if this step is overlooked.
The third risk is the underinvestment trap. McKinsey's survey of health system leaders indicates that many feel they are underinvesting in digital solutions relative to the challenges they face 14. This trap is selective: capital often flows readily to visible robotic platforms, while compounding software layers—RPA libraries, predictive models, and monitoring bots—remain underfunded. Operators who reverse this allocation and treat software as durable infrastructure can fully leverage the scaling benefits described in earlier sections.
Frequently Asked Questions
References
- 1.AI and the Health Care Workforce.
- 2.3 Ways AI Can Improve Revenue-Cycle Management.
- 3.Hospital Trends in the Use, Evaluation, and Governance of Predictive AI, 2023–2024.
- 4.The Role of AI in Hospitals and Clinics: Transforming Healthcare in the Digital Age.
- 5.Investigating the Impact of Automation on the Health Care Workforce: A Qualitative Study of a Clinical Conversational Assistant Implemented on Care Pathways.
- 6.The financial realities of robotic surgery programs: insights from recent research.
- 7.AI for Health: Opportunities to Improve Healthcare Delivery and Outcomes.
- 8.AI Interventions to Alleviate Healthcare Shortages and Enhance Working Conditions in Intensive Care Units.
- 9.Increasing Trends of Artificial Intelligence With Robotic Process Automation in Healthcare.
- 10.Utilization of Robotic Process Automation (RPA) and Artificial Intelligence (AI) in Healthcare Operational Processes.
- 11.Applying Robotic Process Automation to Monitor Business Processes in Electronic Medical Record Systems.
- 12.Robotic Surgery and Hospital Reimbursement.
- 13.The Global Health Workforce Stock and Distribution in 2020 and 2030.
- 14.Digital Transformation: Health Systems' Investment Priorities.
- 15.Reimagining the Nursing Workload: Finding Time to Close the Workforce Gap.
- 16.Heartbeat of Health: Reimagining the Healthcare Workforce of the Future.