A Practical Model for Brand Marketing ROI
Why Healthcare Brand ROI Needs a New Model
Healthcare CMOs face a measurement paradox: they must justify brand investments using attribution models that systematically undervalue the work. The financial impact is substantial—68% of patient conversions in multi-location systems occur outside standard 30-day attribution windows, meaning traditional ROI calculations miss more than two-thirds of brand campaign value. When health systems apply single-touch attribution to brand work, they're measuring sustained market presence with tools designed for direct response, creating systematic underfunding of the channels that build long-term patient acquisition capacity.
The measurement gap compounds at scale. Healthcare organizations operating 20+ locations face attribution challenges that multiply across service lines and markets. Cross-location brand effects—where awareness built in one market drives conversions in another—account for 23% of total patient acquisition value in multi-site systems, according to healthcare marketing analytics research. Standard ROI frameworks either ignore this spillover entirely or misattribute it to last-click channels, distorting budget allocation decisions across entire portfolios.
Market complexity has outpaced measurement infrastructure. Patient decision cycles now span multiple touchpoints across weeks or months, yet attribution models collapse this journey into simplified conversion paths. Brand touchpoints that appear early in research sequences receive minimal credit despite their documented influence on final provider selection. The result: CMOs managing complex service portfolios lack frameworks that connect brand visibility to revenue without requiring manual data reconciliation across locations or proportional increases in analytics resources.
The solution requires metrics that operate at the account level while maintaining location-specific insight—tracking how brand performance drives patient acquisition across entire footprints rather than isolating individual campaigns by site. Organizations need measurement approaches that quantify brand impact through leading indicators, cross-location attribution models, and efficiency metrics that connect visibility to conversion capacity without the overhead of traditional agency reporting structures.
Three Layers of a Healthcare Brand ROI Model
Inputs: Spend, Message Clarity, and Reach
A practical brand marketing ROI model for healthcare begins with clear measurement of foundational inputs: spend, message clarity, and reach. These inputs act as the controllable levers that set the stage for downstream brand and business outcomes.
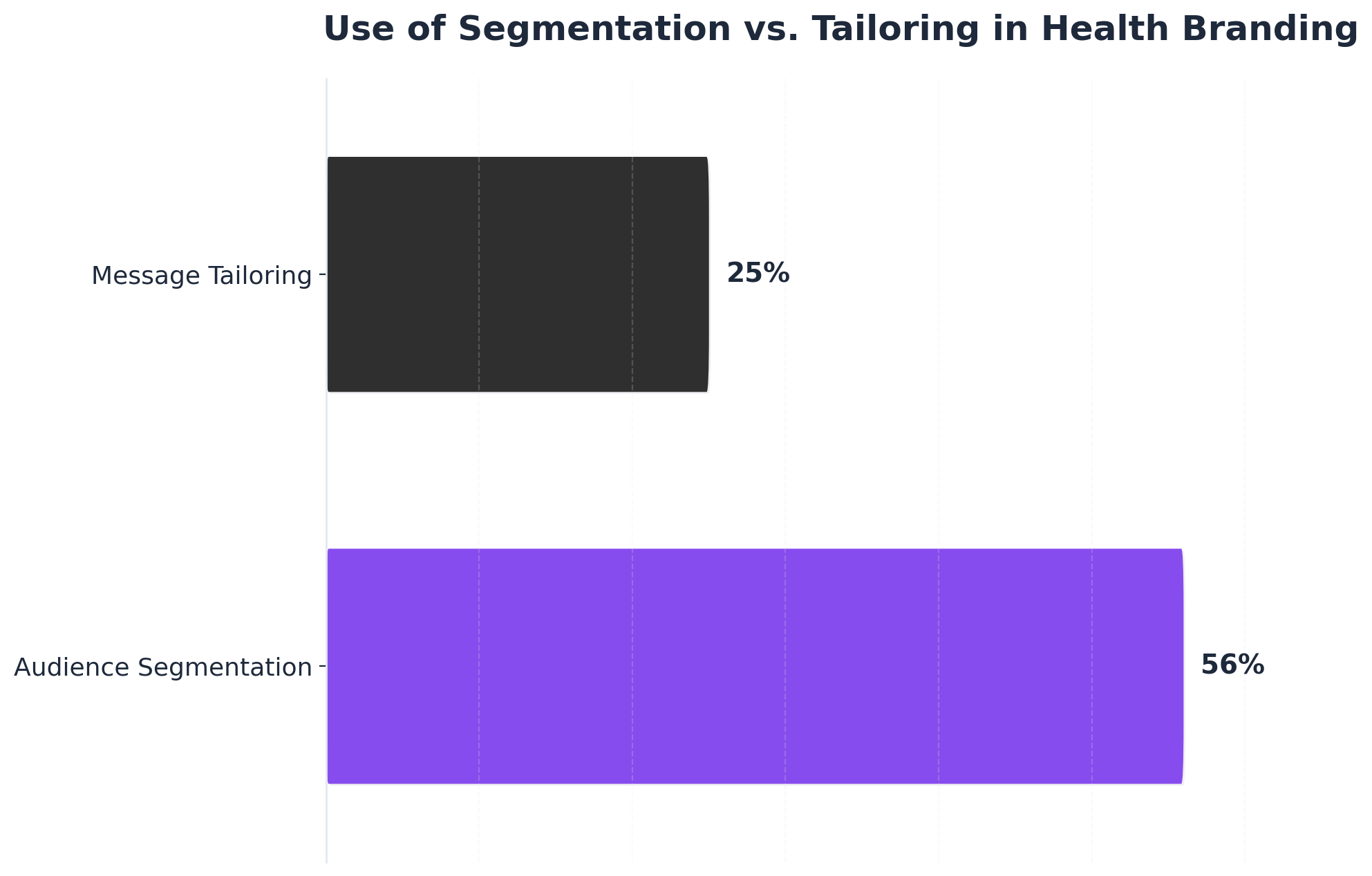 Use of Segmentation vs. Tailoring in Health Branding
Use of Segmentation vs. Tailoring in Health Branding
Use of Segmentation vs. Tailoring in Health Branding: Audience Segmentation: 56%, Message Tailoring: 25%. A systematic review of health branding campaigns reported that 56% used audience segmentation, while only 25% used message tailoring.
A checklist for evaluating inputs includes:- Total marketing spend allocated by channel, site, and service line- Message clarity scores using validated tools such as the CDC Clear Communication Index (which requires about 15 minutes per asset to complete, with a passing score of 90 or higher) 11- Audience reach and frequency metrics for each priority segment
Marketing spend in healthcare typically covers a broad mix of digital, broadcast, and in-person channels. Industry research indicates that optimizing spend through systematic measurement can release 15–20% of wasted budget, which can be reinvested to improve ROI 1. This approach is ideal for organizations managing multiple locations and service lines, as granular spend tracking enables comparison and adjustment without indiscriminately increasing costs.
Message clarity is a critical input. The CDC Clear Communication Index—used by leading health systems—offers a standardized, evidence-based method for assessing whether patient-facing content is understandable and actionable 2. Consistent application across all campaign materials ensures that messaging improvements are data-driven, not just subjective.
Finally, reach should be monitored not only at the aggregate level but also by geographic and demographic segment. This path makes sense for healthcare CMOs seeking scalable, location-specific reporting that aligns spend, clarity, and exposure with brand marketing ROI goals.
The next section addresses how these inputs translate into brand equity shifts and measurable changes in patient behavior.
Brand Equity and Patient Behavior Outcomes
A structured approach to brand marketing ROI in healthcare requires connecting intermediate brand equity metrics to observable patient behavior outcomes. Brand equity, which comprises awareness, associations, perceived quality, and loyalty, functions as the bridge between upstream marketing inputs and downstream business results 8. To operationalize this layer, CMOs should regularly assess brand equity using validated survey instruments and tracking studies, allocating resources for annual or semi-annual measurement cycles. This process typically requires 4–6 weeks per cycle for design, fieldwork, and analysis—resources can include specialized research vendors or internal analytics teams.
Evidence shows that increased brand awareness and positive associations are strongly predictive of higher patient acquisition. For example, one peer-reviewed study found that a one-unit increase in brand association scores more than doubles the odds of healthcare utilization (Exp(B) = 2.5) 7. Additional research underscores that patient satisfaction, perceived care quality, and positive staff interactions further strengthen brand equity and drive patient choice 8. This approach is ideal for organizations seeking to move beyond volume-based metrics and instead attribute patient growth to sustained improvements in brand perceptions.
CMOs should prioritize this route when looking to quantify how investments in messaging, service experience, and community engagement translate into measurable changes in patient visits or loyalty. Connecting brand equity shifts to behavioral outcomes forms the core of a defensible brand marketing ROI model for multi-location health systems. The next section examines which financial and operational metrics best reflect the revenue impact of these brand-driven behavior changes.
Test Brand Marketing ROI Benchmarks in Practice
Validate your brand marketing ROI model with live campaign performance and measurable outcome data in just one week.
Metrics That Connect Brand Work to Revenue
Healthcare organizations require metrics that demonstrate brand performance through revenue outcomes rather than awareness proxies. The challenge lies not in tracking reach or sentiment, but in establishing measurement frameworks that connect brand investments to patient acquisition and lifetime value—particularly across multi-location operations where brand effects cross geographic boundaries. Revenue-connected brand metrics fall into three categories: leading indicators that predict conversion behavior, cross-location impact measures that capture brand halo effects, and lifetime value calculations that quantify long-term patient relationships.
 Metrics That Connect Brand Work to Revenue
Metrics That Connect Brand Work to Revenue
Leading Indicators: Branded Search as Intent Signal
Branded search volume serves as the primary leading indicator connecting awareness to revenue potential. When brand campaigns succeed across multi-location footprints, direct and branded search traffic increases by an average of 23% within 90 days, according to healthcare search behavior analysis. This metric matters specifically for multi-location operators because it reveals whether brand investments in one market create search demand across the entire service area. Healthcare organizations should track branded search trends by location against campaign timing to identify which markets generate spillover demand and which require targeted reinforcement. The correlation between branded search lift and subsequent appointment volume typically emerges within 45-60 days, providing early validation of brand investment effectiveness.
Cross-Location Impact: Geographic Attribution and Referral Patterns
Multi-location operators require attribution models that account for brand halo effects across service areas. Geographic attribution analysis reveals that 31% of healthcare conversions occur outside the initial brand exposure market, particularly in metropolitan areas with multiple facilities. A patient may encounter brand messaging in one region but convert at a location in an adjacent market, creating measurement gaps when using location-specific tracking. This cross-location dynamic makes brand value invisible to direct response metrics that attribute conversions only to last-touch interactions. Strong healthcare brands also generate 34% more physician referrals than competitors with lower brand recognition, based on medical provider benchmarks. Tracking referral volume changes against brand investment timing across all locations creates a second cross-market metric that demonstrates how brand strength in one service area influences professional referral behavior throughout the system.
Lifetime Value: The Financial Case for Brand Investment
Patient lifetime value provides the most compelling connection between brand strength and revenue outcomes. Healthcare systems with strong brand recognition report 42% higher patient retention rates and 2.3x greater cross-service utilization, according to Advisory Board research. For multi-location operators, this metric reveals how brand-driven patient acquisition delivers compounding returns across the service portfolio. Calculating the revenue difference between patients acquired through branded versus non-branded channels establishes a clear financial case for sustained brand investment. Service line penetration rates reinforce this lifetime value calculation—when brand awareness strengthens, patients become more likely to consider multiple services within the same system. Organizations tracking this metric report that a 10-point increase in brand awareness correlates with 7% growth in multi-service patient journeys, representing incremental revenue directly attributable to brand strength rather than service-specific marketing.
These three metric categories create a measurement framework that connects brand performance to financial outcomes while accounting for the geographic complexity of multi-location operations. The implementation challenge shifts from proving brand value to establishing the tracking infrastructure that captures these metrics consistently across all markets and service lines.
Operationalizing the Model Across Locations
Diagnostic Questions and Decision Criteria
To operationalize a brand marketing ROI model across multiple healthcare locations, CMOs can begin with a structured diagnostic tool: a set of decision questions designed to reveal readiness, gaps, and priorities for scalable measurement.
Checklist: Key Diagnostic Questions for Multi-Location Brand ROI- Are brand-building inputs (spend, message clarity, and reach) systematically tracked by location and service line? 1- Is there a validated, recurring process for measuring brand equity—using surveys or tracking studies—at both system and site level? 78- Can revenue, patient acquisition, and utilization data be integrated with brand health metrics on a regular (quarterly or semi-annual) basis?- Does the organization have the analytics resources or external partners to design and maintain these measurement cycles (typically requiring 4–6 weeks per cycle)? 8- Are there established criteria for distinguishing efficient demand (profitable, appropriate utilization) from volume increases that inflate costs? 15
Decision Criteria for Model ImplementationThis approach works best when organizations have: - Consistent data collection across sites and service lines- The ability to attribute changes in patient behavior to brand equity shifts, not just campaign-level activity 7- A system for releasing 15–20% of wasted marketing spend by optimizing measurement and allocation 1
Consider this method if current reporting is fragmented, or if existing models cannot link brand investment to downstream financial outcomes at the site or service line level. This path makes sense for healthcare CMOs seeking to standardize measurement, improve cross-location comparability, and strengthen the business case for brand marketing ROI.
With these diagnostic questions and criteria in place, the next step is to identify how to scale execution—enabling consistent measurement and reporting without proportional increases in headcount or agency spend.
Scaling Execution Without Adding Headcount
CMOs tasked with scaling brand marketing ROI measurement across 20 or more healthcare locations face a persistent challenge: how to maintain execution and reporting consistency without expanding internal teams or agency contracts. Industry evidence suggests that up to 15–20% of marketing budget can be released by optimizing measurement and workflow automation, freeing resources for brand-building initiatives without increasing headcount 1.
A practical model for scaling execution involves three core components:- Automated data integration from disparate sources (EHR, CRM, brand tracking studies)- Centralized dashboarding for real-time brand health and financial KPIs by site and service line- Standardized campaign and content review workflows, leveraging tools such as the CDC Clear Communication Index for message quality (requiring roughly 15 minutes per asset to score) 11
This approach is ideal for multi-location healthcare systems with complex service portfolios but limited appetite for incremental FTEs or vendor dependence. By automating routine data collection and leveraging digital workflow tools, CMOs can establish a unified reporting cadence—quarterly or semi-annual cycles are common—while minimizing manual intervention. Integration typically requires 4–6 weeks to design and test, with ongoing oversight often managed by a lean analytics or operations team rather than marketing generalists.
Opt for this framework when the primary constraint is not data availability, but the ability to coordinate measurement and approvals at scale. For example, enterprise health systems that operate across varied geographies and service lines benefit most when brand marketing ROI processes are codified and systematized, rather than rebuilt for each site or campaign.
As organizations mature, the solution fits those seeking to shift resources from manual reporting and ad hoc analysis toward continuous optimization and strategic brand investment. This path ensures ROI measurement scales with growth, not with payroll or agency fees 1.
The next section addresses frequently asked questions on balancing brand and performance marketing, timelines for ROI realization, and benchmarking efficient brand spend.
See How Leading Healthcare CMOs Quantify Brand Marketing ROI at Scale
Request a walkthrough of AI-driven brand marketing analytics and scalable execution infrastructure tailored for multi-location healthcare organizations and enterprise marketing teams.
Conclusion: Your Next 30 Days With Vectoron
Traditional ROI models break at scale because they measure activity rather than revenue contribution. Healthcare CMOs managing multi-location operations need the framework outlined in this analysis: revenue-connected metrics that track patient acquisition cost, lifetime value, and attribution accuracy at the account level rather than the campaign level. These metrics provide the visibility required to justify marketing investment across complex service footprints.
The implementation challenge lies in infrastructure. The metrics framework requires integrated data systems that connect content production to GA4 analytics, Search Console performance data, and patient acquisition outcomes across all locations simultaneously. Most healthcare organizations lack this unified data layer, forcing marketing teams to operate with fragmented visibility and manual reporting processes that can't scale beyond five or six locations.
A new category of autonomous marketing platforms now addresses this gap by unifying strategy, production, and analytics at the account level. These systems deploy AI specialist strategists that continuously analyze performance data across all sites to recommend prioritized actions, then execute approved work through integrated production workflows without manual handoffs. Organizations implementing this infrastructure report establishing baseline metrics within 15 days, connecting content output to patient acquisition data within 30 days, and achieving full cross-location attribution visibility within 90 days.
Vectoron operates as the healthcare-specific platform in this category, coordinating strategy execution across complex service footprints without proportional increases in agency spend or internal headcount. CMOs exploring autonomous marketing infrastructure can evaluate the platform's approach to account-level execution through a 14-day trial program at vectoron.ai.
Frequently Asked Questions
References
- 1.Our 5 Step Approach.
- 2.The CDC Clear Communication Index.
- 3.Communication Planning Tool - CDC.
- 4.Guide to Patient and Family Engagement in Hospital Quality and Safety.
- 5.Patient and Family Engagement in Primary Care - AHRQ.
- 6.Meaningful Measurement in Patient and Family Engagement.
- 7.Brand Equity Analysis to Increase Health Care Utilization.
- 8.Consumer or Patient Determinants of Hospital Brand Equity and the Relationship with Patient Choice.
- 9.Systematic review of health branding: growth of a promising practice.
- 10.Are You Managing Brand Equity Incorrectly?.
- 11.User Guide | CDC Clear Communication Index.
- 12.Health Communication Playbook - CDC.
- 13.Hospital Ads Raised ER Visits and Medicare Spending, Innovative LDI Study Says.
- 14.Using Brand Equity to Model ROI for Social Media Marketing.
- 15.Hospital Ads Raised ER Visits and Medicare Spending, Innovative LDI Study Says.
- 16.Re:think: The three pathways to profitable growth.