Key Takeaways
- Generic ROI math fails in multi-location healthcare because attribution tracking is restricted under HHS guidance 1, blended LTV hides service-line variance, and media spend understates the true cost of acquisition.
- Layer One draws a documented boundary between marketing pages where analytics can operate and pages where signals become regulated disclosures 2, with the privacy officer co-owning what finance sees.
- Layer Two rolls data up along two axes at once, location and service line, exposing loss-making service lines that a blended location-level return would otherwise greenlight for continued spend.
- Layer Three reports patient acquisition cost as a ratio against service-line contribution margin using fully loaded costs, shifting the conversation from spend justification to spend reallocation across service lines.
- Layer Four separates CLV from CLROI 10so finance can value the patient base while marketing directs the next dollar toward the acquisition pathway that returns more on it.
- Patient experience scores from HCAHPS 4and CAHPS 5belong inside the ROI model as quarterly leading indicators, flagging LTV drift by location and service line before revenue confirms it.
- Operators past twenty locations should replace per-location reporting with account-level rollups, because evaluating one program against one matrix surfaces the service-line concentration that twenty-two separate dashboards bury.
- Static average LTV gives way to predictive inputs service line by service line as cohort history accumulates 11, with the template flagging which figures are observations and which are estimates.
The CFO Conversation That Breaks Most Healthcare ROI Templates
A new CFO inherits a 22-location specialty group and asks the marketing leader to defend a $2.4M annual program. The marketing leader opens a familiar spreadsheet: blended cost per lead, channel-level spend, a return multiple calculated against attributed revenue. Within ten minutes the conversation is over, and not in marketing's favor. The numbers do not reconcile to the general ledger. The attribution model assumes tracking signals that the legal team has already restricted under federal guidance on online tracking technologies 1. The lifetime value figure is a single blended number that flattens orthopedics, cardiology, and primary care into one average that nobody in finance recognizes.
This is the conversation that breaks most healthcare marketing ROI templates. The template was built for a single-location consumer business and then extended, location by location, into a multi-site operator. It treats marketing as a channel problem rather than a service-line economics problem. It cites attributed conversions that a compliance officer cannot vouch for. And it answers a question the CFO did not ask.
The CFO is not asking whether marketing produced leads. The CFO is asking which service lines at which locations are funding the program, what each acquired patient is worth over time, and whether the cost to acquire and serve that patient leaves a return after contribution margin. A defensible template answers those three questions in language finance already uses inside a measurement infrastructure CMS has spent more than $1.3 billion building since 2008 8.
Why Generic ROI Math Fails in Multi-Location Healthcare
The standard ROI formula assumes three things that do not hold in a 22-location healthcare operator: that every conversion can be tracked back to a paid source, that revenue per acquired customer is roughly stable, and that the cost side of the equation ends at media spend. None of those assumptions survive contact with a multi-site service-line business.
Tracking breaks first. Federal guidance on online tracking technologies restricts how covered entities can connect third-party analytics signals to health-related activity on their sites and apps 1. That removes pixel-based conversion data from the back half of the patient journey for most service lines, so any ROI calculation built on a complete attribution chain is already overstating what the template can actually see.
Revenue per patient breaks next. A blended lifetime value figure averages a knee replacement against an annual physical and reports a number that matches neither. Service-line contribution margin varies by an order of magnitude across orthopedics, cardiology, dermatology, and primary care, and a single average hides which service lines are funding the program and which are draining it.
Cost breaks last. Media spend is one input. Patient acquisition cost in healthcare also absorbs intake staffing, scheduling capacity, and the operational cost to serve a patient long enough to realize the revenue the template is claiming.
The Four Layers of a Defensible Template
Layer One: Compliant Attribution Under HHS Tracking Guidance
The first layer of a defensible template is a clear statement of what the marketing team is allowed to see. Federal guidance from the HHS Office for Civil Rights specifies that tracking technologies used by covered entities and business associates fall under HIPAA when they collect or transmit information that ties an individual to health-related activity on a regulated entity's websites or mobile applications 1. The OCR bulletin behind that guidance frames the issue around disclosures: tracking signals routed to third parties can become reportable disclosures when they include identifiers connected to a user's interaction with regulated content 2. That language sets the boundary the template has to draw before any ROI math begins.
In practical terms, the boundary runs between two zones. On unauthenticated marketing pages that describe the organization, its locations, and general service categories, conventional analytics and conversion tracking can usually operate, provided identifiers are not joined to health-related activity. Once a user moves into pages that reveal a condition, treatment, or provider relationship, the same signals that powered the funnel on the marketing side become regulated disclosures on the clinical side. The template needs a documented map of which pages sit in which zone, signed off by the privacy officer, before any conversion event is wired into the ROI model.
That map then drives three template decisions. First, conversion definitions get rewritten around server-side events, call tracking with compliant routing, and form submissions that stop short of clinical detail. Second, attributed revenue is restricted to what the compliant signal set can actually observe, with the gap to total revenue reported as an explicit unattributed bucket rather than hidden inside a blended return number. Third, the template carries a footnote that the privacy officer co-owns, so the figures presented to finance are figures the compliance side already approved.
Layer Two: Location-Level Rollups Across Service Lines
The second layer addresses how data moves up. A single blended ROI figure for a 22-location operator is the executive equivalent of an unsorted spreadsheet: technically complete, operationally useless. CMS frames quality measures as instruments that quantify processes, outcomes, patient perceptions, and organizational structure across distinct dimensions rather than collapsing them into a single index 3. The same logic applies to marketing measurement. ROI has to be reported along two axes at once: location and service line.
The rollup structure is straightforward in concept. At the lowest grain, each acquired patient is tagged with a location and a service line. PAC, contribution margin, and downstream visit revenue are calculated at that grain. The template then rolls up two ways: by location across service lines, and by service line across locations. The first rollup tells the operator which locations are healthy. The second tells the operator which service lines are healthy. Neither view alone answers the CFO's question, because a location that looks profitable in aggregate can be carrying one service line on the back of another.
That hidden-variance problem is why blended numbers are dangerous. A location reporting a positive blended return can contain a Service Line A producing strong contribution margin, a Service Line B operating near break-even, and a Service Line C losing money on every acquired patient. The blended view greenlights continued spend on Service Line C. The disaggregated view exposes it.
The template artifact for finance is a matrix: locations down the left, service lines across the top, contribution after acquisition cost in each cell, and totals on both axes. That matrix is what gets presented. The blended number is what gets relegated to a footnote.
Layer Three: Patient Acquisition Cost Tied to Service-Line Contribution Margin
The third layer is where most templates lose finance. Patient acquisition cost reported as a single dollar figure invites a single dollar comparison, usually to a vague industry benchmark that nobody in the room can source. The defensible version reports PAC as a ratio against contribution margin at the service-line level, because contribution margin is the figure that funds the next marketing dollar.
The arithmetic uses three variables per service line s:
PAC_s : fully loaded acquisition cost
CM_s : contribution margin per acquired patient over a defined revenue window
PAC_s / CM_s : a ratio that finance reads as the share of margin consumed by acquisition
Fully loaded means media spend plus the operational cost of converting interest into a booked, completed visit: call center capacity, scheduling friction, no-show recovery, and the intake labor required before the first appointment is recognized as revenue. Templates that stop at media spend understate PAC by a margin large enough to flip the conclusion on lower-margin service lines.
Contribution margin is also a service-line variable, not a system constant. An orthopedic episode, a cardiology workup, and a primary care annual visit do not produce the same CM_s under the same payer mix, and they do not move the same way when volume changes. The template carries CM_s as an input owned by finance, refreshed quarterly, rather than as a marketing assumption.
The output is a ranked view:
- service lines where PAC_s / CM_s sits comfortably below one,
- service lines where it approaches one,
- and service lines where it crosses.
The last group is where the conversation shifts from spend justification to spend reallocation, and that is the conversation finance wants to be in.
Layer Four: Separating CLV from CLROI
The fourth layer is the one that survives the hardest CFO questions. A Harvard Business School faculty note draws an explicit line between customer lifetime value and customer lifetime return on investment, presenting them as two related but distinct measures of the financial value of a customer to the firm 10. CLV measures the value a customer generates. CLROI measures the return on the cost to acquire and serve that customer. Most healthcare marketing ROI templates report one number and call it the other, which is the moment finance stops trusting the model.
The distinction matters because two patient cohorts can carry identical CLV and produce materially different CLROI. Imagine Cohort 1 and Cohort 2, both acquired into the same service line, both producing the same downstream revenue over a five-year window. Cohort 1 arrives through a referral pathway with low PAC and a short scheduling cycle. Cohort 2 arrives through a paid funnel that required higher media spend, more intake labor to convert, and a longer time from first contact to first completed visit. CLV is identical. CLROI is not, because the denominator is not. The template that reports only CLV would treat both cohorts as equally valuable. The template that reports CLROI directs the next marketing dollar toward the acquisition pathway that returns more on it.
The template carries both. CLV per service line is the numerator finance uses to value the patient base. CLROI per service line by acquisition pathway is the operating metric marketing uses to decide where the next dollar goes. Presented together, they answer two different questions that finance and marketing have historically argued about by talking past each other. Presented as a single conflated figure, they invite the question that ends most marketing ROI conversations: what exactly is in that number, and why does it not match the general ledger.
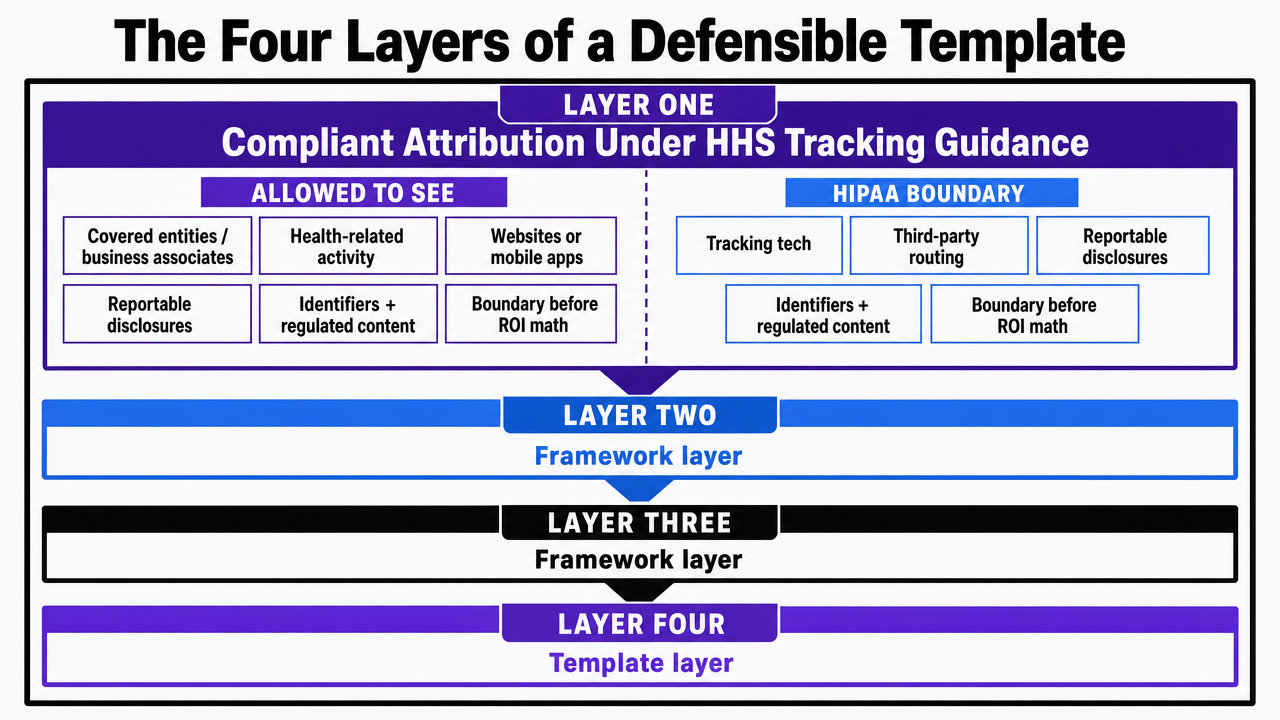 Visualize the four-layer operating framework that structures the entire article's central recommendation
Visualize the four-layer operating framework that structures the entire article's central recommendation
Test Real-Time ROI Reporting in Practice
Experience hands-on ROI calculations using your actual marketing data before making a commitment.
Patient Experience as a Leading Indicator of Retention Economics
Retention is where healthcare LTV is actually built, and patient experience is the earliest signal that retention will hold. AHRQ defines patient experience as the full range of interactions a patient has with the healthcare system, from access and scheduling to communication with clinicians and support staff 6. That definition matters for the ROI template because every one of those interactions sits downstream of the marketing promise and upstream of the second visit, the referral, and the renewed episode of care.
CMS administers HCAHPS as a standardized instrument designed to produce comparable data on patients' perspectives of care across hospitals 4, and AHRQ's CAHPS Database lets operators benchmark their own results against overall and regional averages to prioritize where improvement effort returns the most 5. Inside the template, scores from those instruments enter as leading indicators for the LTV inputs in Layer Four. A location with declining communication or access scores is a location whose CLV assumption is about to drift down, and the template should flag that drift before the revenue lag confirms it. AHRQ's own framing is direct on the link: good patient experiences track with better clinical outcomes 7, and those outcomes are what keep acquired patients inside the system long enough for marketing spend to earn out.
The operational consequence is that experience scores belong inside the ROI model as quarterly inputs by location and service line, not in a separate quality report that finance never sees alongside the spend justification.
If You Manage 20+ Locations: Reporting Model Choices That Shape the Budget Conversation
Per-Location Reporting vs Account-Level Rollup
The audience narrows here. A solo-site practice and a 22-location specialty group both produce marketing ROI reports, but the reporting model that defends spend at scale is structurally different from the one that defends it at a single site. Operators managing twenty or more locations face a choice that most agency relationships have already made for them by default: per-location reporting, where each site is treated as its own P&L with its own marketing line, or account-level rollup, where the program is measured as a single growth engine producing patients across the entire footprint.
Per-location reporting is the legacy of retainer-based agency billing. Each location pays a fee, gets a dashboard, and shows up to its own monthly call. The structure looks accountable. It also hides the two things finance most needs to see. Cross-location variance gets buried inside twenty-two separate reports that no one reads side by side, and service-line concentration across the network becomes invisible because each report blends its own service mix into a local blended return.
Account-level rollup inverts the unit of analysis. The program is one program. Spend, PAC, contribution, and patient counts are tracked at the account level and then disaggregated along the two axes that matter: location and service line. The CFO sees one budget producing one matrix, with the per-location and per-service-line cuts available underneath.
| Dimension | Per-Location Reporting | Account-Level Rollup |
|---|---|---|
| Spend unit | $X per location, N times | Single account budget across N locations and S service lines |
| PAC view | Local blended PAC per location | PAC_s by service line, with location as a secondary cut |
| Hidden variance | Service-line losses masked inside local averages | Loss-making service lines surface in the rollup matrix |
| Reallocation lever | Negotiate per-location retainer | Shift spend across service lines and locations from one plan |
The reporting choice is also a budget-conversation choice. Per-location reporting forces finance to evaluate spend twenty-two times. Account-level rollup asks finance to evaluate one program against one matrix, which is the conversation the template was built to win.
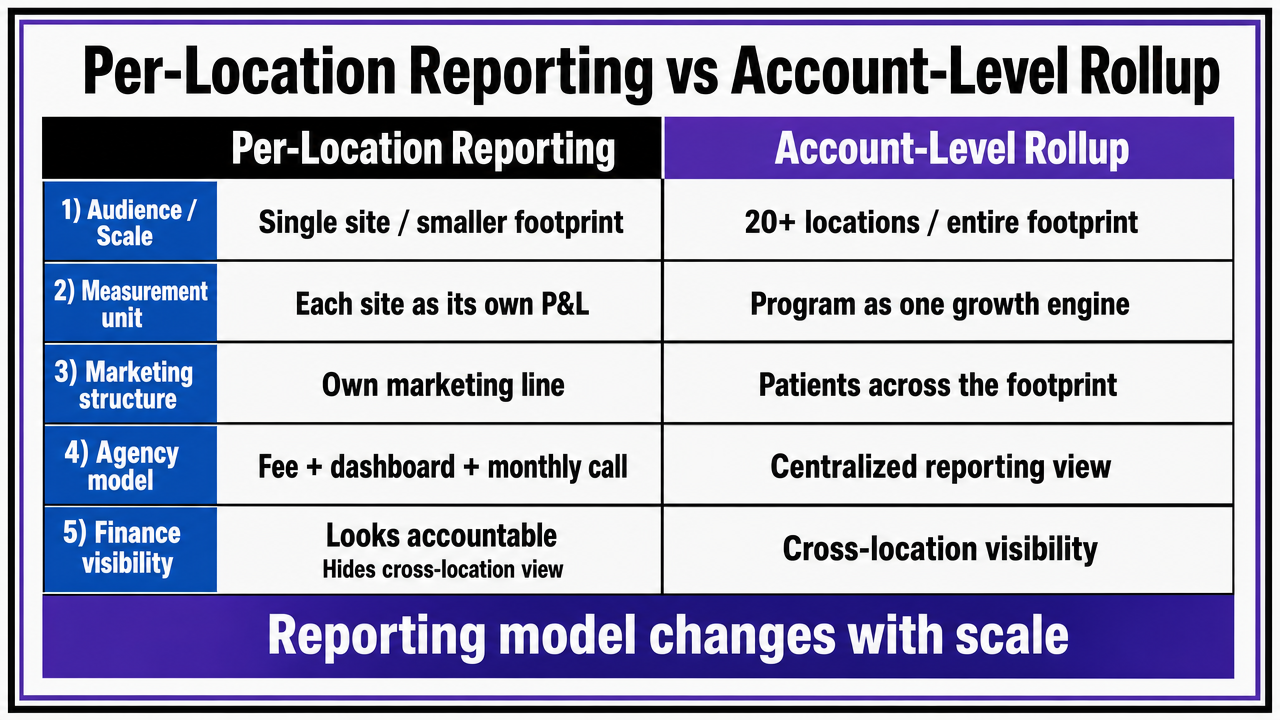 Visualize the side-by-side comparison table already present in the section, reinforcing the reporting-model decision
Visualize the side-by-side comparison table already present in the section, reinforcing the reporting-model decision
Moving from Static Averages to Predictive LTV Inputs
Once the rollup is in place, the LTV inputs feeding Layer Four come under pressure. A static average LTV per service line, refreshed annually, is acceptable for a five-location operator with thin historical data. It stops being acceptable at twenty-plus locations, where the volume of acquired patients across distinct service lines and payer mixes is large enough to support segmented models. Peer-reviewed work on customer value measurement points toward machine learning approaches that segment customers using lifecycle value theory rather than collapsing them into a single average 11.
The practical shift is incremental, not theoretical. The template starts with static CLV_s as a placeholder, then replaces each service-line input with a predicted CLV distribution as historical patient panels accumulate enough observations to support segmentation by acquisition pathway, payer, and visit cadence. Marketing does not own the model; finance and analytics do. Marketing owns the consumption of its outputs inside the ROI template.
The trigger for the move is data sufficiency. Service lines with several quarters of stable cohort behavior across multiple locations are ready. Service lines with sparse history stay on static inputs until they are not. The template carries a column noting which LTV input is static and which is predictive, so finance knows which figures are observations and which are estimates.
See How a Data-Driven ROI Template Can Clarify Marketing Impact Across Locations
Get a sample ROI template designed for multi-location healthcare and agency teams—built to quantify marketing impact, budget allocation, and scalability without guesswork. Ideal for CMOs managing complex service lines at enterprise scale.
A Worked Example: Variance Between a Strong and Lagging Location
Consider two locations inside the same 22-site specialty group, both running identical media plans at the same monthly spend per location ($X). Location A sits in a market with a mature referral network and stable intake staffing. Location L opened eighteen months ago, runs a thinner front desk, and serves a payer mix that skews lower on contribution margin for the same procedures.
Run the template against both. At Location A, PAC_s for the flagship service line lands at roughly 18% of CM_s, with completed-visit conversion holding above the network median. At Location L, PAC_s for the same service line lands closer to 47% of CM_s, driven less by media efficiency and more by intake friction: longer call-back windows, higher no-show rates, and a scheduling cycle that loses booked patients before the first visit is recognized as revenue. Media-level cost per lead looks similar at both sites. The fully loaded acquisition cost does not.
The blended account-level number averages these two locations and lands somewhere defensible. The matrix view does not let them average. Location A is funding the program. Location L is consuming it, and the consumption is operational, not creative. Reallocating media away from Location L would worsen the problem; the lever is intake capacity, not channel mix. That is the diagnosis the template is built to produce, and it is the conversation finance will fund against because the recommended action sits inside operations rather than inside a new agency scope of work.
Putting the Template in Front of the Board
The board meeting is not where a marketing ROI template gets debated. It is where the template either holds or it does not. The version that holds opens with the matrix from Layer Two, locations down the left and service lines across the top, and lets the disaggregated view do the talking before any narrative slide intervenes. Finance reads the matrix the way it reads any other operating report.
Three artifacts travel with the matrix:
- A one-page note from the privacy officer confirming the attribution scope, so no one in the room can dispute what the conversion data represents.
- A CLROI ranking by acquisition pathway and service line, presented alongside CLV rather than instead of it.
- And a column flagging which LTV inputs are observed versus predicted, so estimates are not mistaken for measurements.
The recommendation that follows the matrix is specific: which service lines at which locations receive additional spend, which trigger an operational fix before more spend, and which get cut. That is the format that turns a marketing review into a capital allocation conversation, and it is the conversation platforms like Vectoron are built to support across an entire footprint rather than one location at a time.
Frequently Asked Questions
References
- 1.Use of Online Tracking Technologies by HIPAA Covered Entities and Business Associates.
- 2.Use of Online Tracking Technologies.
- 3.Quality Measures.
- 4.HCAHPS: Patients' Perspectives of Care Survey.
- 5.Section 5: Determining Where To Focus Efforts To Improve Patient Experience.
- 6.What Is Patient Experience?.
- 7.CAHPS Surveys: Sorting Fact from Fiction.
- 8.Quality Measure Development and Associated Spending by the Centers for Medicare & Medicaid Services: 2008-2018.
- 9.Summary of the 2020 AHRQ research meeting on 'advancing patient experience measurement and patient-centered outcomes'.
- 10.Customer Lifetime Value (CLV) vs. Customer Lifetime Return on Investment (CLROI).
- 11.Research on customer lifetime value based on machine learning algorithms.