Key Takeaways
- Acquisition at multi-site scale breaks at the coordination layer between vendors, not at the channel level, making the connective tissue across strategy, execution, and measurement the real bottleneck.
- A four-layer sequence compounds in order: foundation (findability and reputation), access (scheduling, telehealth, reminders), experience (coordinated touchpoints), and loyalty, with each layer requiring the prior one to function 1, 2, 15.
- HIPAA segmentation work should default to non-PHI signals like geography, consented intake data, and owned web behavior, reserving PHI-driven communication for the operations lane under 45 CFR 164.501 and 164.508(a)(3) 3.
- Growth teams running ten or more sites should evaluate where coordination hours, publishing cycle time, and fragmented attribution scale linearly with location count, since those variables — not media spend — quietly dominate operator economics.
Acquisition Has Become a Coordination Problem, Not a Channel Problem
Walk into the marketing operations meeting at a 40-site specialty group and the symptoms are remarkably consistent: three SEO vendors with overlapping scopes, a paid search agency that bills per location, a reputation tool that doesn't talk to the CRM, and a content calendar that quietly fragmented into 40 calendars somewhere around the second acquisition. The channels are not the problem. The channels are largely the same ones every operator uses. What breaks at scale is the connective tissue between strategy, execution, and measurement across sites.
That distinction matters because the evidence on which acquisition levers actually move volume is settled enough to plan against. Coordinated, multi-channel engagement supports stronger patient experience and loyalty when the channels are actually integrated rather than run in parallel 1. Telehealth expands access and produces high satisfaction when workflows are built around it 2. Consumer expectations for convenience, digital access, and price clarity now shape provider choice in ways health systems cannot opt out of 5. None of this is new to a healthcare marketing leader. What is new is the operating cost of running each of those levers as a separate vendor relationship, with its own retainer, reporting cadence, and approval queue, multiplied by every clinic on the map.
The rest of this analysis treats acquisition as an operating-system question and works backward from there.
The Four-Layer Model: Foundation, Access, Experience, Compounding
A useful way to organize acquisition decisions for a multi-location operator is to stack them in the order they actually compound:
- Foundation comes first: search visibility, accurate location data, and reputation signals that determine whether a clinic appears at all when a prospective patient looks. Many medical practice websites still lack core SEO features that affect discoverability 17, which makes this layer a prerequisite rather than an optimization.
- Access sits on top of foundation. Self-scheduling, telehealth, and reminder systems convert demand the foundation layer surfaces, with telehealth associated with improved access and high satisfaction when integrated into workflow 2.
- Experience is the third layer — coordinated touchpoints across portals, messaging, and clinic visits that consumer expectations now treat as table stakes 5.
- Compounding is the fourth: loyalty and referral economics that lower long-run acquisition cost as the first three layers mature 15.
The sequence matters because investing in experience or compounding before foundation and access work simply amplifies friction. The sections that follow take each layer in order and identify where execution breaks at scale.
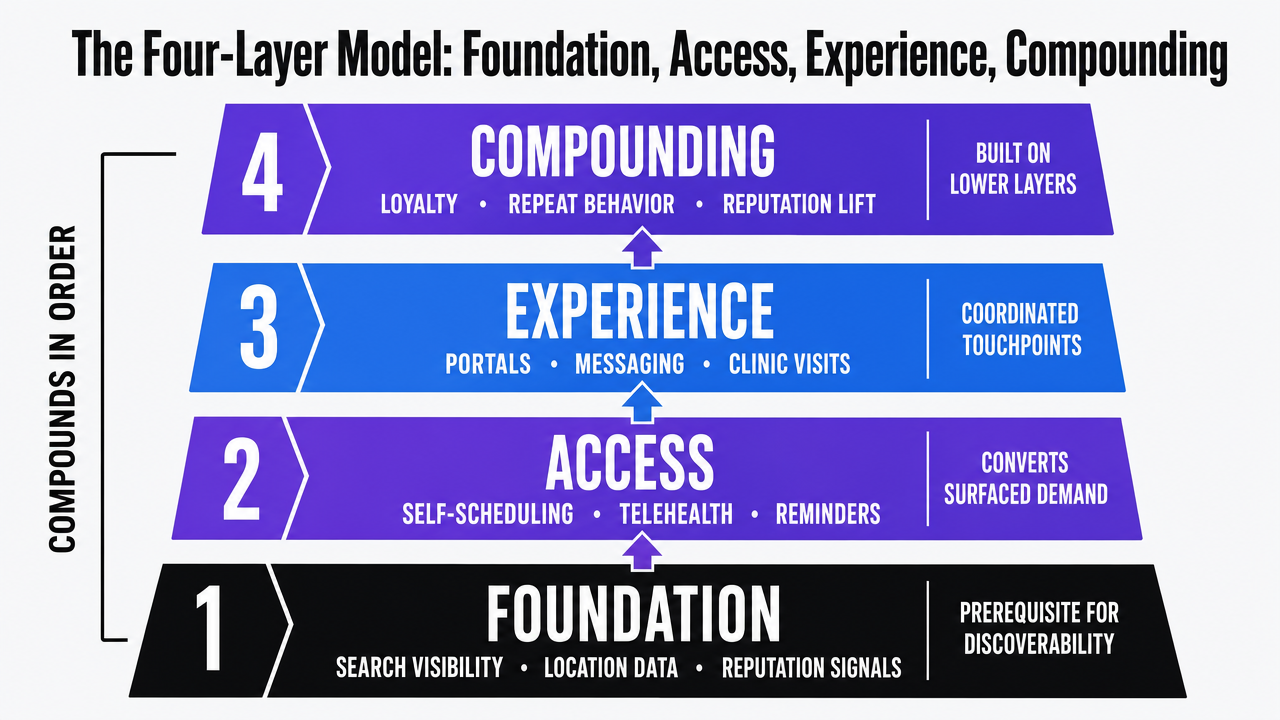 Visualize the four-layer compounding model that organizes the entire article's framework, showing the sequential dependency of foundation, access, experience, and loyalty layers
Visualize the four-layer compounding model that organizes the entire article's framework, showing the sequential dependency of foundation, access, experience, and loyalty layers
Layer One — Foundation: Findability and Reputation Across Every Site
Findability: Where Search Visibility and Location Data Break Down
Foundation work fails quietly. A clinic ranks fifth instead of first for its highest-intent local query, and nobody on the marketing team notices because the report still shows traffic — just less of it than the site two miles away. A cross-sectional study of medical practice websites found that a substantial proportion lacked core SEO features that influence discoverability, including basic technical and content elements associated with higher search rankings 17. The study examined practice websites directly rather than health system portals, so the gap is most acute at the location level — exactly where multi-site operators do their growth work.
That gap interacts with reputation in a specific way. A systematic review of online patient reviews concluded that reviews play a meaningful role in how individuals choose providers, shaping perceptions of quality and trust during the consideration window 9. The review synthesized studies across geographies and specialties, so the takeaway is directional rather than a precise lift figure: when a prospective patient lands on a search result, the rating, volume, and recency of reviews influence whether they click and whether they convert.
For a 40-site group, the operational problem is that findability requires location-level work — schema, NAP consistency, service-page depth, review velocity — that does not survive being handed to one agency per market. Each vendor optimizes its own scoreboard. Account-level coordination is what keeps the foundation from cracking along the seams between sites.
Reputation as a Foundation Asset, Not a Marketing Campaign
Treating reviews as a quarterly campaign is the most common reason reputation programs underperform at scale. The systematic review on online reviews framed them as an ongoing input into provider choice rather than a periodic asset class 9, which means the operational unit of work is the post-visit review request at every location, every day — not a once-a-quarter push.
The mechanism connecting reputation to acquisition runs through experience. Patient experience has been described in the marketing literature as a strategic asset that drives word-of-mouth, loyalty, and organizational reputation, with experience strategy and clinic operations functioning together rather than as separate workstreams 8. When a clinic delivers a clean visit and the operator captures that moment with a structured review request, the foundation layer compounds. When the request never goes out, paid acquisition has to carry weight that organic signals should have absorbed.
The takeaway for multi-location operators is that reputation work belongs in the same operating cadence as scheduling and clinical follow-up, not in a separate marketing campaign queue. Centralizing the workflow — request templates, response standards, escalation paths — while letting each site execute against it is the structural fix.
Test unified patient acquisition strategies at scale
Experience account-level execution of multi-location patient marketing campaigns before making a commitment.
Layer Two — Access: Converting Demand Without Adding Headcount
Self-Scheduling, Telehealth, and the Digital Front Door
Foundation work surfaces demand. The access layer decides whether that demand becomes a booked visit or a dropped session. For multi-location operators, the binding constraint is rarely awareness — it is the gap between the moment a prospective patient is ready to act and the moment a clinic is ready to receive them.
Telehealth changes the geometry of that gap. A systematic review of telehealth adoption found that virtual care was associated with improved access and generally high patient satisfaction when technology and clinical workflows were properly integrated, with clinical outcomes often non-inferior to in-person care across the contexts studied 2. The review covered varied specialties and settings, so the takeaway is directional: telehealth functions as an access expansion mechanism, not a replacement for physical capacity. For a network with uneven provider availability across markets, virtual visits absorb demand that geography or scheduling lag would otherwise lose.
Self-scheduling sits next to telehealth in the same access stack. When a prospective patient lands on a location page from search or a review profile, the conversion path either runs through a real-time booking widget or it routes to a call center with hold times that compete with three other clinics on the same results page. The operational question is whether scheduling, virtual care intake, and intake forms share patient identity across sites or fragment it. Consumer expectations for digital access and convenience have moved from preference to baseline across healthcare 5, which means an access layer that asks the same patient to re-enter information at every touchpoint is leaking demand the foundation layer paid to generate.
Reminders and Conversion: The Lowest-Cost Lever in the Stack
Reminder systems are the most underrated line item in a healthcare growth budget. A systematic review and meta-analysis of reminder interventions across SMS, phone, and email modalities concluded that reminders were associated with a significant improvement in appointment adherence compared with no reminder, with heterogeneity across modality and frequency 10. The analysis pooled studies across settings rather than isolating new-patient cohorts, so the cleanest read is that reminders reduce attrition between scheduling and visit — which is exactly where new patient volume hemorrhages.
The math at scale is unforgiving. A 40-site group running paid search to fill new-patient slots is paying twice when a reminder workflow fails: once for the click, once for the empty room. Reminder cadence, channel, and content belong in the same operating layer as scheduling and telehealth, not in a separate engagement tool with its own login and reporting view.
The operational fix is to treat the booked-to-seen conversion rate as a top-line acquisition metric at every site, not a clinic operations footnote. When that metric moves into the marketing dashboard alongside cost per booked visit, the value of reminder infrastructure stops being theoretical.
Layer Three — Experience: Coordinating Touchpoints Across Sites
Omnichannel Coordination as a Growth Driver
The experience layer is where most multi-location operators discover that their stack is not actually one stack. A prospective patient may search on a phone, click a paid ad, read three reviews, switch to a desktop to compare two clinics, request a callback through a contact form, receive an SMS confirmation from a different system, and arrive at intake to fill out the same demographic fields they already submitted online. Each handoff is a tracked event in a separate tool. None of them know each other.
That fragmentation has a measurable cost. The omnichannel review of health care services concluded that coordinated, integrated channels support stronger patient engagement and loyalty, while poorly orchestrated channels produce the opposite — friction that erodes the experience gains each individual channel was supposed to deliver 1. The review framed omnichannel as an operating design question rather than a technology purchase, which is the right framing for a VP managing dozens of sites with overlapping vendor contracts.
Consumer-led growth analysis reinforces the point: organizations competing on convenience, digital access, and price clarity have to design experiences around the patient rather than around internal departmental boundaries 5. For a multi-location operator, that means the unit of coordination is the patient journey across sites, not the channel performance at any single site.
Patient Portals, mHealth, and the Equity Caveat
Patient portals sit at the center of the digital front door. The state-of-the-science review on portals found that they can improve engagement and satisfaction when interfaces are usable and features like secure messaging and test-result access are integrated into the care workflow, but adoption and active use remain uneven across populations 14. The same review flagged disparities in portal use by age, income, and digital literacy, which carries direct implications for acquisition: portal-gated experiences will systematically underserve segments of the addressable market unless alternative paths exist.
Mobile health interventions extend the surface area beyond the clinic. Evidence on mHealth apps and texting programs shows promise for engagement and adherence across clinical contexts, though results are heterogeneous and sustained use is a recurring challenge 16. For growth teams, the operational implication is to treat portals and mHealth as part of the experience layer's load-bearing infrastructure — not as standalone product launches — and to maintain non-digital fallbacks so the access layer does not narrow the patient base the foundation layer worked to attract.
Layer Four — Compounding: Loyalty, Referrals, and Long-Run CAC
The first three layers buy a patient. The fourth decides whether that patient buys back, sends a neighbor, or churns to the urgent care on the next exit. A conceptual and empirical review of patient loyalty concluded that loyalty drives repeat utilization and word-of-mouth referrals, making it a strategic outcome that compounds acquisition spend rather than a soft retention metric 15. The same review flagged that loyalty is multifaceted — insurance networks, geography, and switching costs all interact with satisfaction and perceived quality, which means loyalty programs cannot be reverse-engineered from any single touchpoint.
The acquisition implication is direct. Patient experience functions as a strategic marketing asset because positive experiences generate the referrals and repeat visits that lower the marginal cost of the next patient 8. A network that closes the experience loop — clean visit, structured follow-up, easy rebooking — converts paid acquisition into organic acquisition over time. A network that does not closes the loop with paid spend forever.
For multi-location operators, the compounding layer is where centralized strategy earns its keep. Loyalty signals — repeat visit rate, referral source, review velocity — need to roll up across sites to identify which clinics generate compounding patient bases and which run on paid drip alone.
Centralize Medical Patient Acquisition Across All Locations—See the Data-Driven Approach
Explore how unified, AI-powered execution enables healthcare organizations and agencies to run coordinated, measurable patient acquisition strategies for every site, all from one account.
HIPAA Marketing Boundaries: What Segmentation and Outreach Can Actually Use
Compliance gets hand-waved in most acquisition playbooks, which is how growth teams end up with campaigns that legal kills the week before launch. The HIPAA Privacy Rule defines marketing narrowly enough that the distinction matters in everyday execution: with limited exceptions, written patient authorization is required before protected health information is used or disclosed for marketing purposes, under 45 CFR 164.501 and 164.508(a)(3) 3. The boundary that trips operators is the line between marketing and health care operations — appointment reminders, treatment alternatives, and care coordination messages generally sit on the operations side, while communications that promote a third party's product or service for which the provider receives remuneration fall squarely into marketing and require authorization 3.
For segmentation work, that distinction shapes what is actually usable. Outreach driven by diagnosis codes, medication lists, or visit history to promote services beyond the patient's existing treatment relationship needs authorization or a different design. Outreach that uses non-PHI signals — geography, service-line interest captured at intake with proper consent, web behavior on the operator's own properties — does not carry the same constraint. The operational fix is to build acquisition workflows that default to non-PHI sources for prospect targeting and reserve PHI-driven communication for the operations lane, with authorization captured deliberately when a campaign genuinely needs it.
Operator Economics for Multi-Location Healthcare
If a Team Manages Multiple Locations: Fragmented vs. Consolidated Execution
For growth teams running ten sites or more, the cost structure of acquisition deserves its own analysis. The traditional model assigns vendors per market: a local SEO shop in one metro, a paid search pod for the southeast region, a reputation tool the central team bought, and a content agency on retainer for the flagship locations. Each contract has its own scope, reporting cadence, and approval queue. The line items look manageable on a per-site basis. The aggregate is where the model breaks.
The comparison below frames the operator economics using variables rather than invented dollars, because the actual numbers depend on market mix, service line, and existing vendor contracts. What matters is how each driver scales.
| Cost or Capability Driver | Fragmented Per-Location Model | Consolidated Account-Level Model |
|---|---|---|
| Monthly retainer exposure | N locations × R retainer (linear scaling) | Single account-level fee (sub-linear) |
| Coordination overhead | H hours per location per month across vendor calls, briefs, and QA | Centralized strategy with localized publishing variants |
| Publishing cycle time | Per-vendor SLAs; multi-week handoffs for content and PPC changes | Single production workflow; same cycle across all sites |
| Attribution coverage | Partial; data fragmented across vendor dashboards | Unified account-level reporting across channels and sites |
| Compliance review | Repeated per vendor, with inconsistent interpretation | One standard applied to all outbound work |
| Loyalty and referral compounding | Hard to attribute; experience signals scattered | Centralized roll-up of repeat visits and referral sources, where loyalty drives repeat utilization and word-of-mouth that lowers long-run acquisition cost 15 |
The variable that quietly dominates the model is H — the coordination hours per location per month. In a 40-site group, even two hours per location across briefs, approvals, and reporting reconciliation reaches 80 hours monthly before any actual creative or technical work happens. That figure scales linearly with N under the fragmented model and approaches a fixed cost under consolidation. The same dynamic applies to publishing cycle time: a content update that takes three weeks to roll out across 40 sites in a vendor-per-market model can move in a single production cycle when strategy and execution share an operating layer.
Service-Line Campaigns: Where Digital Outreach Has Measurable Lift
Not every service line responds to digital outreach the same way, and the evidence is uneven enough that budget allocation should follow it. A meta-analysis of digital interventions for cancer screening — reminders, portal prompts, and educational tools — found that digital approaches were associated with increased participation in screening programs compared with usual care, with variability across populations and intervention designs 11. For an operator running a screening service line, that result reframes digital outreach as a clinical participation lever, not a generic awareness play.
The pattern repeats in primary care. A systematic review and meta-analysis of web-based weight management interventions delivered in primary care reported modest but statistically significant weight loss outcomes compared with usual care, with limitations around follow-up duration and intervention heterogeneity 12. The relevant takeaway for growth leaders is that a digitally supported program can function as a service-line offering that differentiates a network in the market — which directly affects acquisition for that line.
The operational implication is to map digital outreach budgets to service lines where evidence supports lift, rather than spreading the same campaign template across every line on the schedule.
From Retainer-and-Handoff to Account-Level Execution
The four-layer model only compounds when execution runs on a single operating layer. Foundation, access, experience, and loyalty work all touch the same patient — but in the traditional model, they touch that patient through different vendor contracts with different approval queues and different reporting views. The handoff is where the strategy leaks.
Marketing has been described in the healthcare literature as a strategic function rather than a promotional one, requiring sustained investigation of patient needs and tailored service design rather than campaign-by-campaign tactics 6. That framing is incompatible with a retainer-and-handoff structure where each vendor optimizes its own scoreboard on its own cadence. Consolidation activity across hospitals and systems has already reshaped competitive dynamics in many markets 7, which means the operators absorbing new sites cannot afford to inherit and maintain parallel vendor stacks at every acquired location.
Account-level execution treats strategy, content production, technical SEO, paid search, and reputation work as one continuous workflow across every site. The structural unlock is removing the coordination tax that scales linearly with location count. For growth teams under pressure to expand patient volume faster than headcount, that is where Vectoron fits — as the operating layer that runs the four-layer model across the full footprint without the per-location vendor sprawl.
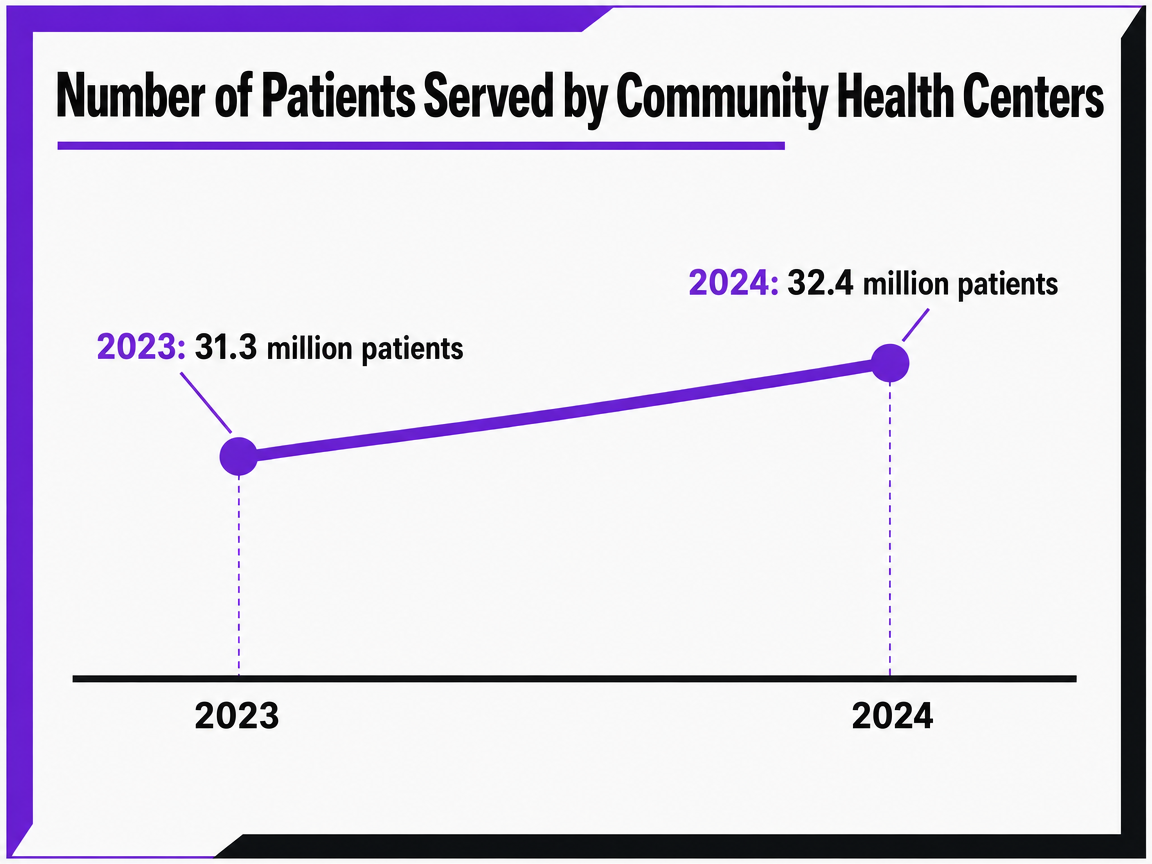 Number of Patients Served by Community Health Centers
Number of Patients Served by Community Health Centers
A time series chart showing the growth in patient volume at US community health centers from 2023 to 2024.
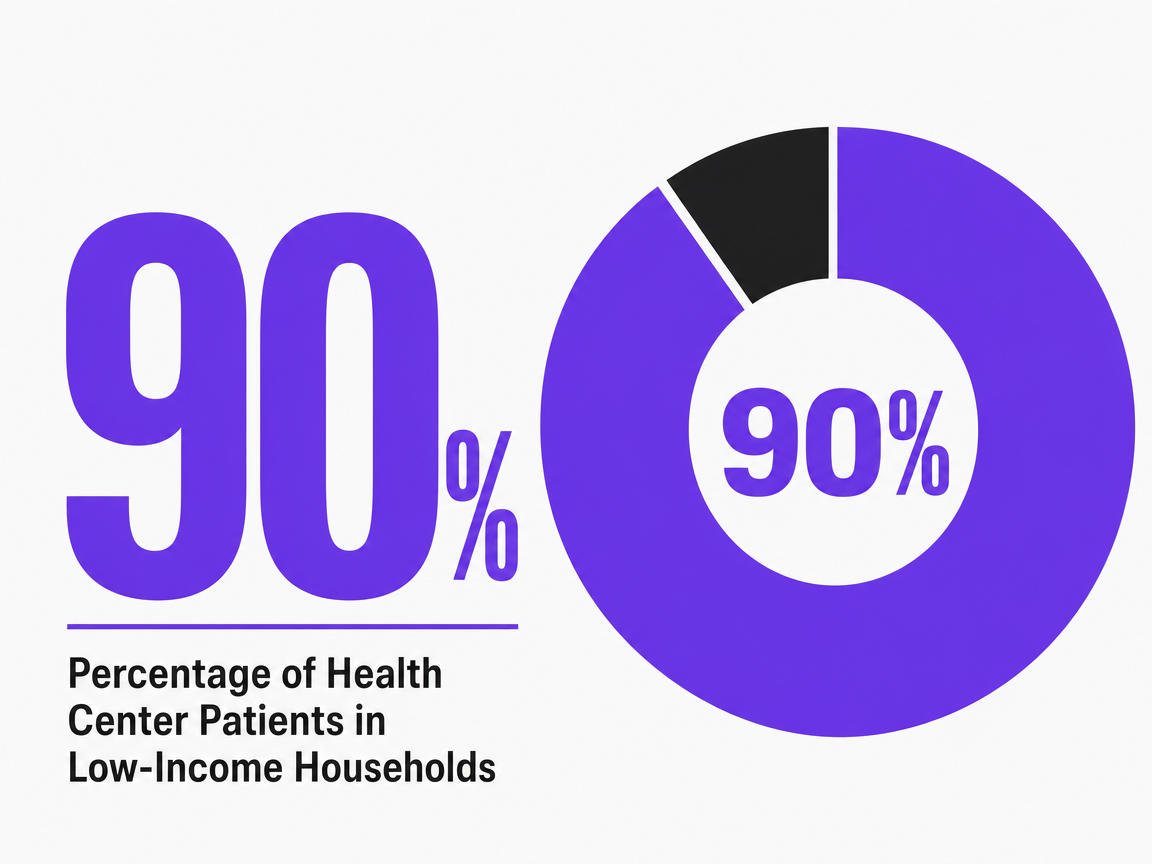 Percentage of Health Center Patients in Low-Income Households
Percentage of Health Center Patients in Low-Income Households
Percentage of Health Center Patients in Low-Income Households
Frequently Asked Questions
References
- 1.An Overview of Omnichannel Interaction in Health Care Services.
- 2.The Impact of Telehealth Adoption on Patient Outcomes.
- 3.Marketing.
- 4.Person and Family Engagement.
- 5.Consumers rule: Driving healthcare growth with a consumer-led strategy.
- 6.The impact of marketing strategies in healthcare systems.
- 7.New Report: Partnerships, Mergers and Acquisitions can Help Hospitals and Health Systems Better Serve their Patients and Communities.
- 8.The role of patient experience in marketing health care services.
- 9.The importance of online patient reviews in decision making: a systematic review.
- 10.Impact of reminder systems on appointment adherence in healthcare: a systematic review and meta-analysis.
- 11.Digital interventions to increase cancer screening: a systematic review and meta-analysis.
- 12.Effectiveness of web-based interventions for weight management in primary care: systematic review and meta-analysis.
- 13.The influence of social media on patient health information-seeking behavior in healthcare.
- 14.Patient portals and patient engagement: a state of the science review.
- 15.Patient loyalty in healthcare: a conceptual and empirical review.
- 16.Mobile health (mHealth) interventions in healthcare: evidence and opportunities.
- 17.Search engine optimization and online visibility of medical practices: a cross-sectional study.