Key Takeaways
- Patient acquisition and retention fail when funded and measured separately, because experience is the shared variable driving both repeat visits and the referrals that lower future acquisition costs 12.
- Value-based contracts reward continuity, experience, and longitudinal outcomes, so acquisition spend should be judged against retained-patient cohorts and quality bonuses rather than first-visit conversion alone 10.
- Continuity of care, access, communication, and digital tangibles are attributable marketing inputs that belong on the growth scorecard alongside CAC, with digital tools measured by segment rather than assumed universal 3, 7.
- Multi-location operators should consolidate fragmented per-location vendor stacks into one account-level plan, one scorecard, and one strategy owner authorized to route retention signals back into media planning.
Why Two Teams Keep Solving Half a Problem
Patient acquisition and retention fail as separate disciplines because they are funded, measured, and executed by different teams with different incentives. Marketing owns the funnel until the first appointment. Operations and clinical leadership inherit everything that happens after. The patient experiences one continuous relationship; the organization manages two disconnected ones.
The split shows up in the data. Acquisition gets measured in cost per lead, conversion rate, and channel attribution. Retention gets measured in recall compliance, no-show rates, and HCAHPS-style experience scores that rarely cross into a marketing dashboard. Two scorecards. Two budgets. Two sets of quarterly targets that compete for the same operational attention.
That competition is expensive. Research on patient experience consistently identifies it as the shared variable that drives both repeat visits and word-of-mouth referrals, meaning the levers retention teams pull are the same levers that lower future acquisition costs 12. When those levers sit outside marketing's authority, growth leaders end up paying to acquire patients the organization is structurally unprepared to keep.
The fragmentation gets worse at scale. A VP of Marketing overseeing 5 to 50 locations typically inherits a vendor stack assembled site by site: one agency for SEO, another for paid media, a third for content, plus regional operations teams running their own recall and reactivation programs. Each vendor optimizes its slice. No one owns the lifetime relationship.
This article argues for a different operating model. One in which continuity of care, experience metrics, and lifetime value are tracked as marketing KPIs, funded from a single account-level budget, and used to redirect acquisition spend toward the segments and service lines where loyalty compounds. The evidence base for that model is stronger than the org chart suggests.
The Business Case for Treating Acquisition and Retention as One System
The shared variable between acquisition cost and retention revenue is patient experience. A 2024 NIH review of the business case for patient experience found that patients with positive care experiences are more likely to return to the same hospital and ambulatory settings, retain their health plan, and voice fewer complaints, with the strongest evidence linking experience directly to retention and indirectly to acquisition through recommendations 12. One variable. Two revenue lines.
That finding reframes the org chart problem as a P&L problem. If experience drives both the patients who stay and the referrals that lower future acquisition costs, then funding experience improvements out of an operations budget while measuring acquisition out of a marketing budget produces a predictable distortion: marketing pays full freight for every new patient because the upstream lever that would reduce that cost sits in someone else's cost center.
The mechanism behind the number is well documented. Satisfaction drives loyalty both directly and indirectly through trust, meaning experience investments compound across the relationship rather than dissipating after a single visit 13. A patient who trusts the practice returns for the next procedure, accepts the referral to an in-network specialist, and recommends the brand to a coworker. None of that shows up in a channel attribution report. All of it shows up in lifetime value.
For healthcare marketing leaders, the operational consequence is direct. The metrics that predict whether an acquired patient becomes a profitable patient — experience scores, continuity rates, time-to-second-visit, referral velocity — belong inside the growth scorecard, not adjacent to it. When those signals route back into media planning, acquisition spend stops chasing volume and starts targeting the segments and service lines where loyalty already compounds.
The alternative is the current state: two teams, two budgets, and a patient relationship that nobody owns end-to-end.
Value-Based Care Made the Old Split Obsolete
Payer economics no longer reward the old division of labor. CMS defines value-based care as a model that ties payment to outcomes, equity, and cost rather than volume of services, with explicit goals around patient experience and longitudinal health management 10. Medicare's value-based programs reward providers based on quality of care delivered to populations, with measure sets that include patient experience, readmissions, and preventive service uptake 2. The same behaviors that drive retention — keeping patients engaged, following up on chronic conditions, closing care gaps — are the behaviors that increasingly determine reimbursement.
The American Medical Association frames the shift in similar terms: value-based arrangements manage a population rather than process transactions, and they require cohesive strategies for acquisition, engagement, and whole-person care 11. That language is worth borrowing. A growth program built around transactional acquisition — buy the click, fill the chair, hand the patient to operations — is structurally misaligned with a payment model that grades the organization on what happens across the next eighteen months of that patient's care.
Implementation honesty matters here. A 2025 scoping review of value-based healthcare found that while the conceptual model is strong, practical adoption varies widely, and patient engagement and data capabilities remain underdeveloped in many organizations 1. The gap is not strategic conviction. It is the absence of measurement infrastructure that connects clinical outcomes, experience scores, and longitudinal patient value into a single view a growth leader can act on.
That gap is the opening for marketing. Value-based contracts create a financial reason for the organization to care about continuity, recall compliance, and experience — the exact variables marketing has historically been told to stay out of. Healthcare marketing leaders who can instrument those variables, attribute them to acquisition channels and service lines, and feed the results back into spend decisions become the team that operationalizes value-based economics, not just the team that fills the funnel.
The implication for the operating model is direct. Acquisition spend should be evaluated against the contractual revenue and quality bonuses each patient cohort actually generates over time, not against first-visit conversion alone. That requires a measurement stack that spans the marketing funnel, the clinical record, and the payer contract — and a team structure authorized to read all three.
Continuity of Care as a Marketing KPI
Continuity of care sits in a strange place on the org chart. Clinical leadership treats it as a care-delivery variable. Operations treats it as a scheduling variable. Marketing rarely touches it at all, even though the evidence shows it is one of the strongest predictors of the outcomes marketing is now being asked to defend.
A foundational review of continuity of care found that higher continuity is associated with increased patient satisfaction, decreased hospitalizations and emergency department visits, and improved preventive service uptake, with no studies documenting negative effects from greater continuity 3. Four downstream variables. One upstream lever. The same review notes that continuity functions as both a clinical and experiential asset, meaning the patient who sees the same provider over time reports higher satisfaction and uses the system more efficiently 3.
A separate study on the determinants of patient satisfaction found that self-reported continuity of care is strongly associated with higher satisfaction, and the authors concluded that improving continuity may improve satisfaction directly 4. That matters for the growth scorecard because satisfaction is the upstream input to loyalty, referral velocity, and the likelihood-to-recommend numbers that quietly determine next quarter's acquisition cost.
The practical move for healthcare marketing leaders is to instrument continuity at the patient level and report it inside the growth dashboard rather than waiting for it to surface in a quarterly clinical quality review. Useful operational measures include:
- the percentage of patients seeing the same provider across visits within a defined service line,
- time-to-second-visit by acquisition channel,
- recall completion rates by location, and
- the proportion of returning patients whose appointments were scheduled before they left the previous visit.
Each of those numbers can be attributed back to an acquisition source. That attribution is the unlock. When marketing can see that paid search in one metro produces patients who complete a second visit within ninety days at a materially different rate than referrals from a community partner in another metro, channel mix decisions stop being about cost per lead and start being about cost per retained patient.
Continuity also creates a defensible reason to invest in the unglamorous parts of the funnel: provider-matching logic on intake forms, scheduling rules that prioritize same-provider booking, recall workflows that fire before the patient lapses, and post-visit messaging that names the specific provider seen. None of those are traditional marketing line items. All of them move the variables that determine whether an acquired patient becomes a retained one.
Treating continuity as a marketing KPI does not require taking it from clinical operations. It requires sharing the measurement. The team that buys the patient should be reading the same continuity report as the team that keeps the patient, because the cost of the next patient depends on what happened to the last one.
Test Unified Patient Growth Execution in Real Time
Experience streamlined patient acquisition and retention strategy across all locations using real content and live campaign data.
What Marketing Can Actually Influence in the Experience
Marketing teams rarely deliver the care. They do design most of the moments around it. A 2023 systematic review of patient satisfaction identified five dimensions that consistently determine how patients rate their experience: healthcare output, access, caring, communication, and tangibles 5. Three of those five sit inside marketing's working scope on any given week.
Access is the most direct. Online scheduling friction, intake forms that demand information the practice already has, call-center hold times, and provider directories that surface the wrong location are all measurable, fixable, and owned by the same team that buys the click. Communication is the next layer. Pre-visit instructions, appointment confirmations, post-visit summaries, and the tone of recall messages shape whether patients feel known by the practice or processed by it. Tangibles cover the digital equivalents of a clean waiting room: site speed, mobile experience, branded patient portals, and the visual coherence between a paid ad and the page it lands on.
Evidence from medical-aesthetic services, a setting where patients have unusually high choice and switching freedom, shows that patient experience significantly influences loyalty intentions, with satisfaction and trust acting as mediators 6. The mechanism generalizes. The patient who finds it easy to book, easy to prepare, and easy to follow up forms the satisfaction-and-trust pattern that downstream loyalty depends on.
The operational takeaway for healthcare marketing leaders is to audit the experience layer using the five-dimension frame and to claim ownership of the digital surfaces inside it. Caring and clinical output remain with providers. Access, communication, and tangibles belong on the growth scorecard, with each one tied to a retention metric the same dashboard already reports.
Digital Engagement Without the Uniform-Win Fantasy
Patient portals, telehealth visits, and secure messaging are the easiest line items to defend on a retention slide. They are also the line items most likely to be overstated. A 2023 rapid review of patient perspectives on digital health tools found that empowerment, self-management, and personalization drive adoption, while digital literacy, health literacy, and privacy concerns operate as active barriers that can blunt the same tools in the populations that need them most 7. Digital engagement is not a uniform retention win. It is a segmented one.
The segmentation matters for spend allocation. A portal rollout that lifts re-engagement rates among commercially insured patients in a metro market may produce flat or negative effects in a rural service area where broadband, device access, and reading-level mismatches collide. The review explicitly flags the risk that poorly designed digital programs can widen disparities rather than close them, which has direct implications for organizations operating across mixed payer mixes and demographics 7.
Healthcare marketing leaders can treat digital tools as conditional retention infrastructure rather than universal engagement upgrades. The operational moves are concrete:
- measure portal activation and message-response rates by location, payer, age band, and language preference;
- pair digital recall with phone and mail fallbacks for segments where uptake is low; and
- audit the reading level and translation quality of automated communications before scaling them.
Adoption data should sit on the growth dashboard alongside CAC and continuity metrics, because a portal that no one opens is an acquisition cost the organization is paying twice.
Community and Population-Level Acquisition
Acquisition strategy stops being a media-buying exercise once the organization is accountable for the health of a defined geography. The American Hospital Association's framing of population health management makes the shift explicit: hospitals operating across communities must move beyond inpatient encounters and toward coordinated strategies that address the health of defined groups 16. For multi-location operators, that defined group is the actual service-area population each site is competing to serve, retain, and report on.
Community engagement is the acquisition channel that compounds. A 2025 CDC model for community-engaged prevention emphasizes integrated efforts across education, clinical care, and service, with partnerships across social services, business, and faith organizations that address the root causes of inequities driving chronic disease burden 8. Those partnerships produce something paid search cannot: a steady inflow of patients arriving with context, trust, and a relationship to the institution before the first appointment. The National Academy of Medicine perspective on hospital and public health collaboration treats community health needs assessments not as compliance paperwork but as a planning instrument that aligns local needs with service-line strategy 9.
The operational consequence for healthcare marketing leaders is that community partnerships, screening events, and population-level outreach belong inside the growth program, not in a separate community-benefits silo where their acquisition value goes uncounted. Tracked correctly — by referral source, service line, and downstream retention rate — these channels often outperform paid acquisition in cost per retained patient, particularly in service areas where commercial paid media saturation has already pushed CAC past the point where first-visit revenue justifies it.
Align Patient Acquisition and Retention Across Every Location—From a Single Platform
See how centralized, AI-powered campaign execution enables multi-site teams to unify content, PPC, and SEO for measurable patient growth—without adding headcount or duplicating work across locations.
Chronic Disease Programs as One Motion, Not Two
Chronic disease management is the clearest case where acquisition and retention collapse into a single workflow. A systematic review of disease management programs found that these interventions can improve both effectiveness and efficiency of care for chronic conditions, though the magnitude varies by program design 14. The patients who benefit most are the ones already in the system but at risk of falling out of it, and the patients who should enter the program are often already attached to the practice in some other line of care.
That overlap rewrites the funnel. Enrolling an eligible diabetes or cardiovascular patient into a structured program is an acquisition event for that service line and a retention event for the broader relationship. The same outreach motion — risk stratification on the existing panel, targeted messaging by condition, scheduling that anticipates the next touchpoint — produces both numbers. Splitting it across a marketing campaign and an operations recall workflow duplicates effort and obscures attribution.
Integrated care models reinforce the point. Combining care integration with a population health approach depends on cohesive strategies that span prevention, coordination, and longitudinal engagement 15. Healthcare marketing leaders running chronic disease growth should report enrollment, program completion, and twelve-month retention on one scorecard, funded from one budget.
Account-Level Economics for Multi-Location Operators
The arguments so far apply to any healthcare organization trying to fund acquisition and retention from one strategy. The economics get sharper, and the case for consolidation gets harder to ignore, for growth leaders running 5 to 50 sites under one P&L.
Multi-location operators inherit a vendor stack that was assembled site by site. One agency runs SEO for the flagship location, another handles paid media for the suburban cluster, a content shop produces blog posts for the service-line launch, and a backlink vendor was brought in last year for a single market. Each contract was rational in isolation. Together they produce a tax on coordination that scales with every new location opened or acquired.
The tax shows up in three places:
- Vendor count multiplies the number of strategy conversations required to move a single decision.
- Per-location billing turns every new site into a fixed cost increase rather than a marginal one.
- The reporting roll-up that should tell a VP of Marketing which markets are producing retained patients arrives as a stack of separate dashboards that no one has reconciled.
The literature on integrated care and population health makes a parallel point about clinical operations: combining integration of care with a population health approach depends on cohesive strategies that span prevention, coordination, and longitudinal engagement across defined populations, and those strategies fail when governance, financing, and data systems are not aligned across the organizations delivering them 15. The same logic applies to the growth program. Fragmented vendors cannot feed retention signals back into acquisition spend if no one owns the consolidated view.
The comparison below isolates the cost drivers that move when an operator shifts from a fragmented per-location stack to a unified account-level model. Directional language is used on the fragmented side because the dollar figures vary too widely across markets and vendors to quote responsibly.
| Cost driver | Fragmented per-location model | Unified account-level model | Operational consequence |
|---|---|---|---|
| Vendor count | Scales with locations and channels | One account-level plan | Coordination overhead determines speed of strategy changes |
| Billing basis | Per site, per channel, often per deliverable | Account-level, fixed against the full footprint | New locations either inflate cost linearly or join at marginal cost |
| Strategy coordination | Distributed across vendor account managers | Single strategy owner across SEO, PPC, content, backlinks | Determines whether channel mix reflects retention data |
| Content production cycle time | Variable by vendor queue and approval chain | One production pipeline, one approval workflow | Cycle time governs service-line launch speed and recall content cadence |
| Reporting roll-up | Multiple dashboards, manual reconciliation | One account-level view across sites and channels | Determines whether LTV and continuity signals reach media planning |
| Retention-loop feedback to acquisition spend | Rare; clinical and experience data sit outside vendor scope | Built into the planning cadence | Decides whether spend chases volume or retained patient cohorts |
The last row is the one that justifies the model. A fragmented stack cannot route continuity rates, second-visit timing, and experience scores into next quarter's media plan because no vendor in the stack is paid to read those signals. A unified account-level plan can. That is the difference between an acquisition budget that funds growth and one that funds churn.
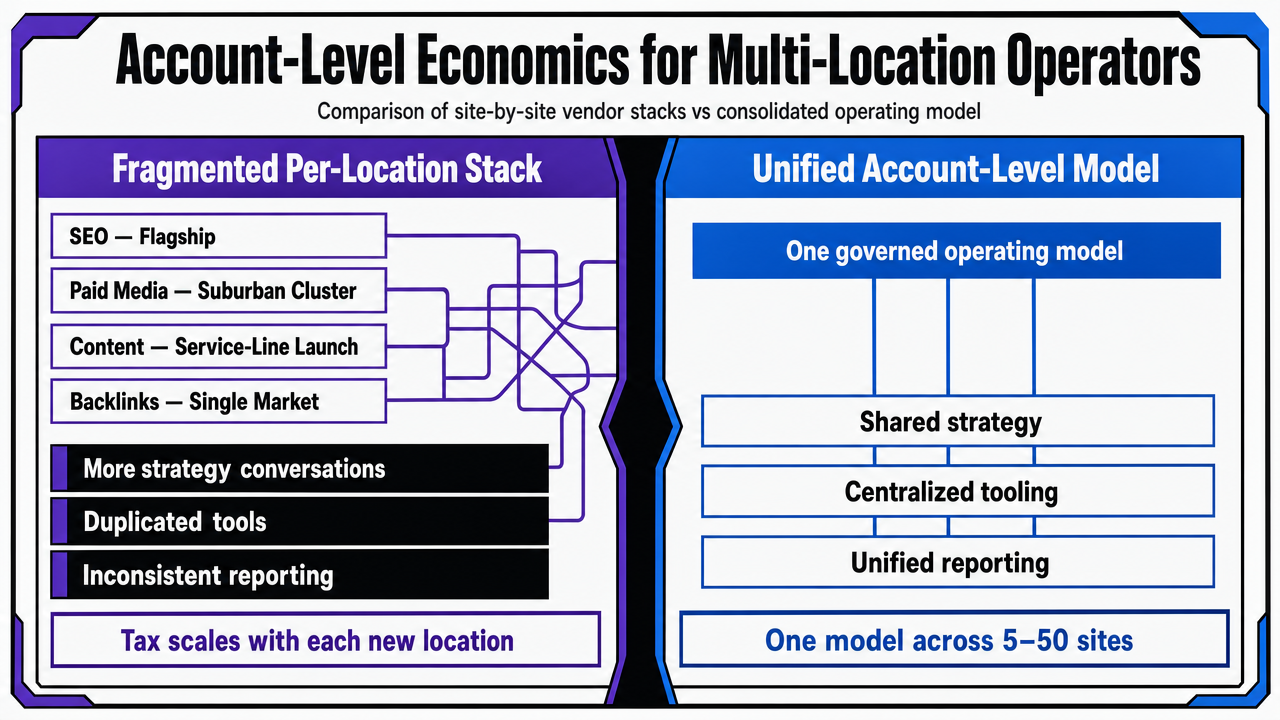 Visualize the section's comparison table contrasting fragmented per-location vendor stacks against a unified account-level operating model, mirroring the cost drivers explicitly discussed in the prose
Visualize the section's comparison table contrasting fragmented per-location vendor stacks against a unified account-level operating model, mirroring the cost drivers explicitly discussed in the prose
An Operating Model That Funds Loyalty and Growth From One Budget
The model that follows from the evidence has three properties. One budget covers acquisition and retention. One scorecard reports CAC, continuity, experience dimensions, and lifetime value side by side. One strategy owner sets channel mix against retained-patient cohorts rather than first-visit volume. Everything else is implementation.
The measurement stack is the first build. Acquisition data from GA4, Search Console, and ad platforms has to reconcile against second-visit timing, recall completion, and experience scores at the patient level. Without that join, the satisfaction-to-trust-to-loyalty chain documented in the research stays invisible to the team buying the patients 13. With it, media planning starts treating retention signals as inputs rather than afterthoughts.
The governance change is the harder build. A single strategy owner has to be authorized to read clinical experience data, set targets across service lines, and reallocate spend across markets without renegotiating six vendor contracts. That authority is what separates a growth program operating under value-based economics from one still optimizing for first-touch conversion.
For multi-location operators, the practical path is an account-level marketing operating system that runs content, SEO, paid media, and backlink work against one consolidated plan and one consolidated dashboard. Vectoron is built for that operating model. The acquisition budget and the retention scorecard finally fund the same patient relationship.
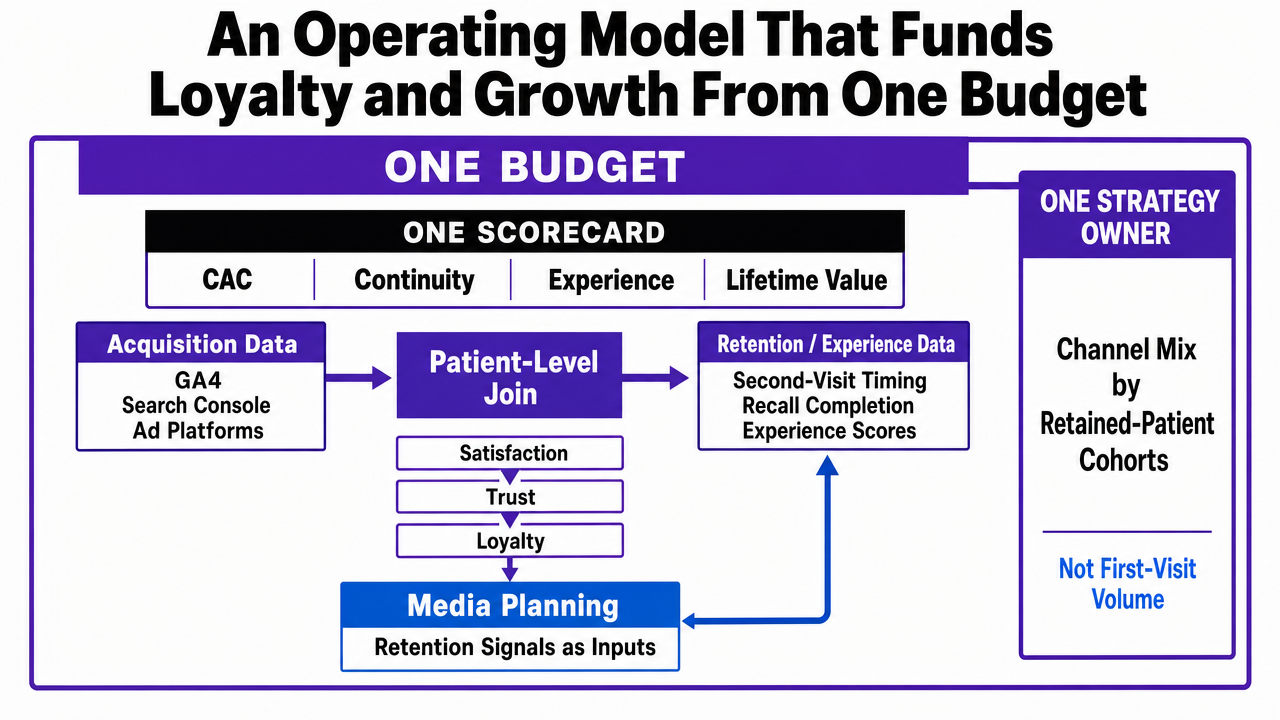 Process infographic visualizing the three-property unified operating model described in this section: one budget, one scorecard, one strategy owner, with the measurement stack feeding retention signals back into media planning
Process infographic visualizing the three-property unified operating model described in this section: one budget, one scorecard, one strategy owner, with the measurement stack feeding retention signals back into media planning
Frequently Asked Questions
References
- 1.Implementing value-based healthcare: a scoping review of key elements and support strategies.
- 2.CMS' Value-Based Programs.
- 3.Does continuity of care improve patient outcomes?.
- 4.Continuity of Care and Other Determinants of Patient Satisfaction.
- 5.Patient Satisfaction with Healthcare Services and the Techniques Used for its Assessment.
- 6.The Impact of Patient Experience on Loyalty in the Context of Medical-Aesthetic Health Services.
- 7.Patients' Perspectives on Digital Health Tools: A Rapid Review.
- 8.Harnessing the Power of Community Engagement for Population Health and Health Equity.
- 9.Improved Population Health Through More Dynamic Public Health and Health Care System Collaboration.
- 10.Value-Based Care.
- 11.What is value-based care?.
- 12.Examining the Business Case for Patient Experience.
- 13.The Impact of Patient Satisfaction on Patient Loyalty with the Mediating Role of Patient Trust.
- 14.The Effectiveness and Efficiency of Disease Management Programs for Patients With Chronic Diseases.
- 15.Combining Integration of Care and a Population Health Approach.
- 16.Managing Population Health: The Role of the Hospital.