Key Takeaways
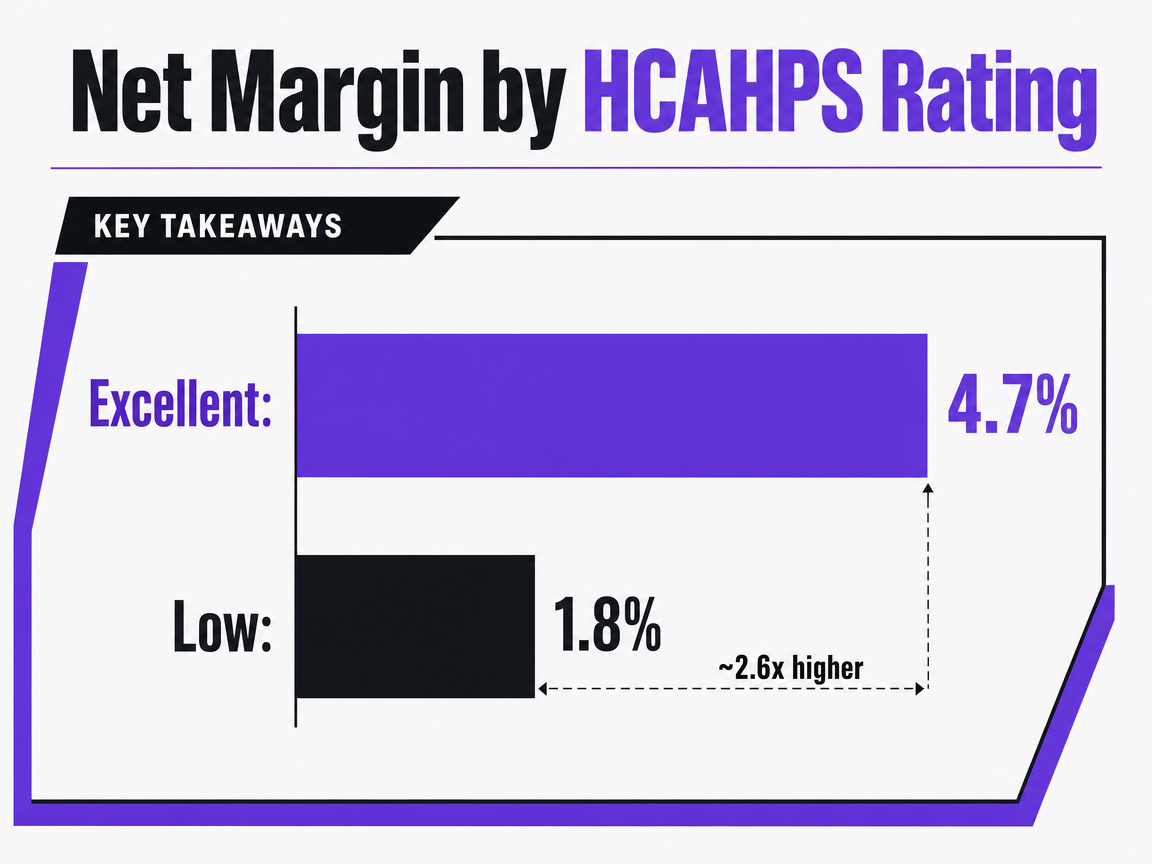
Compares the average net margin of hospitals with 'excellent' HCAHPS ratings versus those with 'low' ratings.
- A three-layer ROI model—acquisition economics, satisfaction and trust as leading indicators, and financial linkage to net margin—translates marketing activity into the language finance uses for budget decisions.
- Hospitals with excellent HCAHPS ratings averaged 4.7% net margin versus 1.8% for low-rated peers, and a 10-point top-box gain tracked with a 1.4-point margin lift 1.
- Payer mix dictates the formula: fee-for-service lines argue volume times margin per case, while value-based lines must include HCAHPS-linked reimbursement as a contracted revenue variable 6.
- Across 20+ locations, standardize CAC, LTV, retention, and experience definitions at the account level before rollup, and align satisfaction data to marketing cohorts rather than leaving it siloed in operations.
Why channel dashboards collapse under CFO questioning
Most healthcare marketing reviews encounter a common challenge. While CMOs present channel-level metrics like cost per lead, paid search efficiency, and click-through rates, CFOs often ask about the impact on net margin and specific service lines. Traditional dashboards frequently lack these answers because they are not designed to connect marketing activities to financial outcomes.
This is the "linkage problem." Channel metrics describe marketing efforts, but they don't speak the language of finance, which focuses on metrics such as net patient revenue per adjusted discharge, operating margin, and value-based purchasing exposure. Until acquisition and retention metrics are translated into this financial vocabulary, marketing can appear as a mere expense.
Evidence suggests this translation is possible. Hospital-level analyses link patient-reported experience to increased future revenue, reduced costs, and a higher share of elective patients, even after accounting for other factors 10. Multivariate studies on quality ratings and profitability also show a measurable revenue increase tied to HCAHPS improvements 2. The financial impact exists; the challenge lies in the measurement architecture used to track it.
This article outlines a three-layer model—acquisition economics, loyalty drivers, and downstream financial impact—designed to connect marketing's influence to finance's reports. Each layer is validated by its ability to demonstrate a direct impact on the income statement.
The three-layer ROI architecture that survives finance review
Layer one: acquisition economics CFOs already accept
The first layer focuses on metrics commonly reported by marketing teams and generally accepted by finance, provided the calculations are precise. These include patient acquisition cost (total marketing investment divided by new patients acquired), patient lifetime value (average visit revenue × visit frequency × retention years × gross margin), and payback period (months until cumulative gross profit from a new patient cohort exceeds acquisition spend).
While these concepts are not controversial, issues arise from imprecise inputs. Marketing spend that excludes agency fees, attribution windows that miscount repeat visits as new acquisitions, or LTV models using list price instead of contribution margin can undermine the ROI case. Ensuring accurate inputs is crucial before presenting outputs.
To make layer-one numbers defensible, three disciplines are essential:
- Define new-patient cohorts by service line, as acquisition costs vary significantly (e.g., primary care versus orthopedic surgery).
- Base LTV on gross margin per encounter, not gross revenue, as finance prioritizes margin.
- Report payback in months to align with the receivables cycles finance already monitors.
Layer one helps secure a meeting but doesn't guarantee budget approval. Acquisition economics accurately describe costs but don't explain whether acquired patients remain loyal, refer others, or transition to higher-margin services. This is where layer two becomes critical, addressing areas often overlooked by standard marketing dashboards.
Layer two: satisfaction, trust, and NPS as leading indicators of retention revenue
Retention rate is a lagging indicator; by the time it declines, revenue is already lost. Metrics that predict retention earlier, such as patient satisfaction, perceived trust, Net Promoter Score (NPS), and HCAHPS dimensions, are vital for marketing KPIs. They signal potential issues before financial damage appears in quarterly reports.
Structural evidence supports this. A peer-reviewed model of healthcare patients found that satisfaction positively influences trust, and both significantly predict loyalty, with strong statistical correlations 7. This causal chain demonstrates to finance that survey-measured satisfaction is not merely a "feel-good" metric but a key variable determining patient return rates and referrals.
The financial benefits of this chain have been quantified. A 2023 analysis in the European Journal of Health Economics, using hospital-level data, showed that improved patient-reported experience predicts higher future revenue, lower future costs, and an increased share of elective patients 10. The "elective share" is particularly important for CFOs, as it represents the high-margin case mix that grows with stronger retention and reputation.
These metrics are actionable for marketing because the drivers of satisfaction—communication quality, access, and waiting time 4—are areas marketing influences through intake design, appointment scheduling content, pre-visit communication, and post-visit follow-up. While clinical encounters are operational, marketing shapes the overall patient experience.
Practically, marketing should track three survey-derived KPIs alongside layer-one funnel metrics:
- A satisfaction score segmented by service line and location
- A trust or willingness-to-recommend item (NPS-aligned)
- A 12-month retention rate segmented by acquisition channel
Reporting these together shifts the narrative from "we generated leads" to "we generated patients who stayed, referred others, and increased elective volume." This narrative sets the stage for layer three, which translates these insights into financial terms.
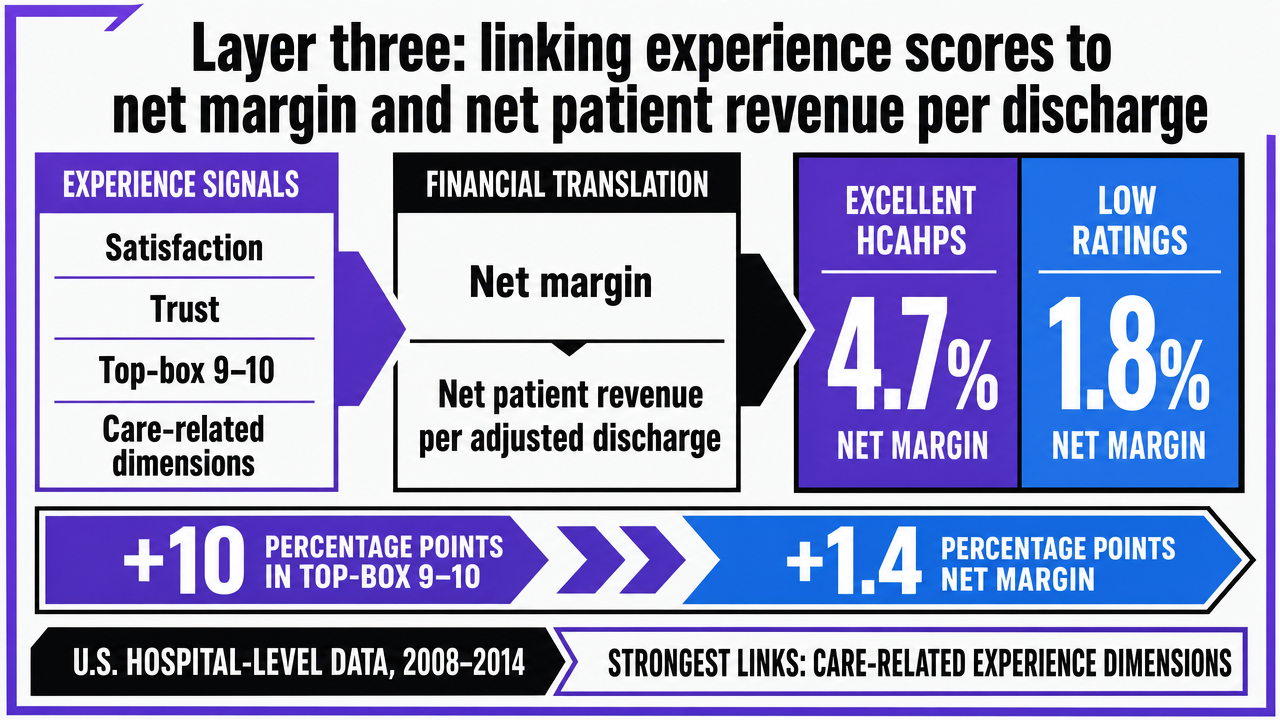
Layer three: linking experience scores to net margin and net patient revenue per discharge
Layer three transforms marketing's case into a financial argument. The goal is to translate satisfaction, trust, and experience signals from layer two into metrics CFOs use, such as net margin and net patient revenue per adjusted discharge.
Deloitte's analysis of national HCAHPS data (2008–2014) provides a financial anchor. Hospitals with "excellent" HCAHPS ratings had an average net margin of 4.7%, compared to 1.8% for those with low ratings 1. The study also found that a 10-percentage-point increase in top-box (9–10) ratings correlated with a 1.4-percentage-point increase in net margin 1. When presenting these figures, it's important to note that the data is hospital-level and U.S.-national, and the strongest associations were with care-related experience dimensions (e.g., nurse communication), not amenities.
This distinction is crucial for budget allocation. Evidence suggests that marketing programs investing in pre-visit communication, post-discharge follow-up, and patient-facing care narratives correlate with margin movement, unlike investments in lobby redesign or signage.
Layer three also considers reimbursement mechanics. HCAHPS scores, administered by CMS, directly influence value-based purchasing, linking experience scores to Medicare payments 6. For systems with significant Medicare exposure, improving patient experience is not just about retention; it's a reimbursement factor that finance already models, often without marketing's direct involvement.
For reporting, layer three requires a quarterly view showing satisfaction and NPS movement from layer two alongside corresponding net margin and net patient revenue per discharge by service line. When these metrics align over time, the ROI argument becomes clear. Divergences prompt diagnostic questions about specific experience dimensions or patient journey gaps, leading to informed budget decisions and integrating marketing into financial reviews.
 Visualize the Deloitte finding that hospitals with excellent HCAHPS ratings averaged 4.7% net margin versus 1.8% for low-rated peers, which is the central financial anchor of this section
Visualize the Deloitte finding that hospitals with excellent HCAHPS ratings averaged 4.7% net margin versus 1.8% for low-rated peers, which is the central financial anchor of this section
Measure patient acquisition ROI with live data
Experience real-time patient acquisition and retention analytics on actual campaigns before you commit.
Service-line ROI: where marketing actually moves margin
System-wide ROI averages can obscure critical insights: which service lines effectively convert marketing investment into margin, and which do not. Blended figures, combining high-margin orthopedic lines with thin-margin urgent care, are easily seen through by finance. A service-line decomposition that links acquisition cost, retention rate, and experience scores to revenue per discharge within each line is essential.
Empirical evidence supports separating experience from broader quality metrics at the service-line level. Multivariate analysis shows that a one-point increase in a hospital's HCAHPS Summary Star Rating correlated with an 8.8% increase in net patient revenue per adjusted discharge, significantly higher than the 3.4% increase associated with a one-point rise in the broader Hospital Compare rating 2. While observational and hospital-level, this gap highlights that patient experience is a more impactful lever within the quality bundle, and one that marketing can directly influence.
This asymmetry reshapes service-line ROI reporting. For each line, three key columns should accompany revenue per discharge:
- A 12-month retention rate segmented by acquisition channel
- A service-line-specific HCAHPS or equivalent experience score
- The elective share of the case mix
Elective share monetizes loyalty; better experience predicts a higher proportion of elective patients, a high-margin segment finance already tracks 10. When marketing investments in pre-visit communication, scheduling content, and post-discharge follow-up improve experience scores in elective-heavy lines, the revenue lift becomes evident in the same financial columns used by finance.
The key reporting discipline for service-line ROI is segmentation at the input layer. Calculating acquisition cost across all new patients and then dividing by line afterward can obscure channel-level differences that explain varying retention curves. A more effective approach assigns marketing spend, channel mix, and experience measurement to each line from the outset. This ensures the rollup accurately reflects investment decisions. Service lines demonstrating a measurable lift in revenue per discharge receive more budget in the next cycle. Underperforming lines are diagnosed to identify specific experience dimensions or channels causing churn before further investment.
Fee-for-service math versus value-based math: which model your payer mix forces
The appropriate ROI formula is determined by the organization's payer mix. Marketing leaders must align their reporting model with the financial framework used by finance to maintain credibility. The distinction is clear: fee-for-service ROI emphasizes volume multiplied by margin per case, while value-based ROI focuses on outcomes per dollar spent, with experience-linked reimbursement as an added factor.
In a predominantly fee-for-service environment, the financial model rewards rapid patient acquisition within high-margin service lines. The marketing argument centers on case volume, payer mix within each line, and contribution margin per encounter. Retention is measured by repeat visits and referral volume. While experience metrics are still important, they function as predictors of return visits and word-of-mouth, not as direct reimbursement variables. The CFO conversation in this model revolves around cost per acquired case versus margin per case, with payback measured in months.
For value-based or mixed payer models, the financial calculus changes. Value is defined as health outcomes achieved per dollar spent. It's crucial not to conflate satisfaction with this definition, as doing so can misdirect spending 5. In this context, the marketing argument must include a reimbursement column: HCAHPS scores directly impact value-based purchasing, linking experience scores to Medicare payments in a way that doesn't exist in pure fee-for-service models 6. Here, an improvement in satisfaction is not just a retention strategy but a contracted revenue variable.
Consequently, the same acquisition and retention metrics are weighted differently based on payer mix. Two service lines with identical CAC and LTV can yield distinct ROI cases: one rewarded for volume, the other for outcomes per dollar against a benchmark. Reviews of value-based care implementation highlight that fee-for-service persistence within mixed systems can hinder accurate measurement, as incentive structures conflict and data infrastructure often fails to separate them cleanly 9.
The disciplined approach is to explicitly state the model before presenting numbers. Begin ROI presentations by outlining the payer mix for each service line, specifying which financial model applies, and reporting the corresponding metrics. Service lines exceeding a defined Medicare or value-based threshold should be evaluated using the outcomes-per-dollar framework with experience scores as a reimbursement variable. Lines below this threshold should use the volume-times-margin approach. Finance already understands and models these distinctions on the revenue side.
See How Leading Healthcare Operators Quantify Patient Acquisition ROI
Request a walkthrough of advanced patient acquisition and retention metric dashboards designed for multi-location healthcare brands. Learn how top teams benchmark, visualize, and optimize marketing ROI at scale.
If you manage 20+ locations: rolling acquisition and retention metrics up to an account view
Why per-site CAC and operations-owned experience data sink the ROI case
The scope of ROI analysis changes significantly for multi-location organizations. While single-site ROI logic holds up in a CFO review due to centralized inputs, a growth program spanning 20 or more sites and multiple service lines often produces fragmented metrics. Each metric might be calculated with slightly different rules, resulting in a rollup that finance cannot reconcile.
Per-site CAC is a primary point of failure. When acquisition cost is calculated individually for each location, shared channel spend (e.g., programmatic advertising, brand search, system-level content) is allocated using varying formulas across markets. This can lead to two sites with similar underlying performance reporting CAC figures that differ by 30% or more, depending on the allocation method chosen by local teams. Finance perceives this as inconsistent math rather than a coherent measurement story.
Operations-owned experience data presents another challenge. HCAHPS and similar surveys are typically managed by quality and operations teams, residing in clinical dashboards separate from marketing's CRM. This disconnect prevents marketing from linking satisfaction improvements at the service-line level back to the specific acquisition channels that generated those patient cohorts. Consequently, the crucial link between loyalty drivers and financial outcomes, supported by published evidence 7, 10, is severed. The metric exists, but the architecture to leverage it for ROI is absent.
The solution is structural: implement a single, account-level definition layer for CAC, LTV, retention rate, and experience scores. This standardized approach must be applied consistently across all locations and service lines before any data aggregation is attempted.
Measurement architecture comparison: per-location retainer model versus account-level operating model
The difference between operating models is fundamentally a measurement architecture question. Patient acquisition and retention metrics behave differently depending on whether they are calculated within fragmented per-location engagements or a unified account-level program. The table below uses formula variables and sourced benchmarks discussed in this article.
| Metric | Per-location retainer model | Account-level operating model |
|---|---|---|
| CAC definition | Marketing spend ÷ new patients, calculated separately per site with inconsistent allocation rules for shared channels | Single formula applied across all locations; shared-channel spend allocated by a documented rule before rollup |
| LTV definition | Average visit revenue × visit frequency × retention years × gross margin, often computed only where local data permits | Same formula, segmented by service line and rolled up at the account level so margin-rich lines are visible |
| Retention rate | Tracked unevenly; cohorting by acquisition channel rare | 12-month retention cohorted by channel and service line across the footprint |
| Experience metric ownership | HCAHPS and satisfaction data sit with operations; not linked to acquisition cohorts | Survey-based satisfaction, trust, and NPS items aligned to marketing cohorts and reported alongside CAC and LTV 7 |
| Financial linkage | Blended system averages obscure where experience movement produces margin lift | Net margin and net patient revenue per discharge reported by service line, with experience scores in adjacent columns 1, 2 |
| Reporting cadence | Quarterly site reports; coordination drag between local vendors delays rollup | Continuous account-level view; engagement runs across the care journey rather than as episodic campaigns 12 |
The operational implication is clear. In a retainer model, the CMO presents disparate reports that finance struggles to consolidate, and the link between experience improvements and revenue per discharge remains unclear. In an account-level model, metrics are calculated consistently, segmented uniformly, and presented in the financial language CFOs understand. Implementation reviews of value-based care emphasize that robust digital infrastructure and outcome measurement are prerequisites for demonstrating financial return, not afterthoughts 9. The architectural framework must precede the metric selection.
What an always-on engagement operating model changes
Episodic campaigns yield episodic data. A spring service-line push or a quarterly newsletter generates a CAC figure for its duration, then goes quiet, leaving critical experience metrics to be tracked on a different timeline. The American Hospital Association highlights that patient loyalty requires continuous engagement across the entire care journey, not isolated promotional efforts. The challenge in quantifying this often stems from disconnected data systems 12.
An always-on operating model transforms the ROI architecture in three ways:
- Satisfaction, trust, and NPS are continuously measured against marketing-generated cohorts, rather than through quarterly, operations-owned surveys 7.
- Content influencing communication quality, access perception, and pre-visit clarity—key satisfaction drivers 4—operates as a maintained system, not a one-off campaign.
- The financial linkage layer updates in sync with marketing inputs, making the lag between experience improvements and revenue responses a measurable interval, not an annual surprise.
Implementation reviews of value-based care identify digital infrastructure and continuous outcome measurement as crucial for systems that prove ROI versus those that merely claim it 9. For multi-location operators, building this infrastructure is paramount. A platform like Vectoron is designed to provide this account-level measurement and execution continuously across all sites and service lines, aligning with the evidence-based operating posture.
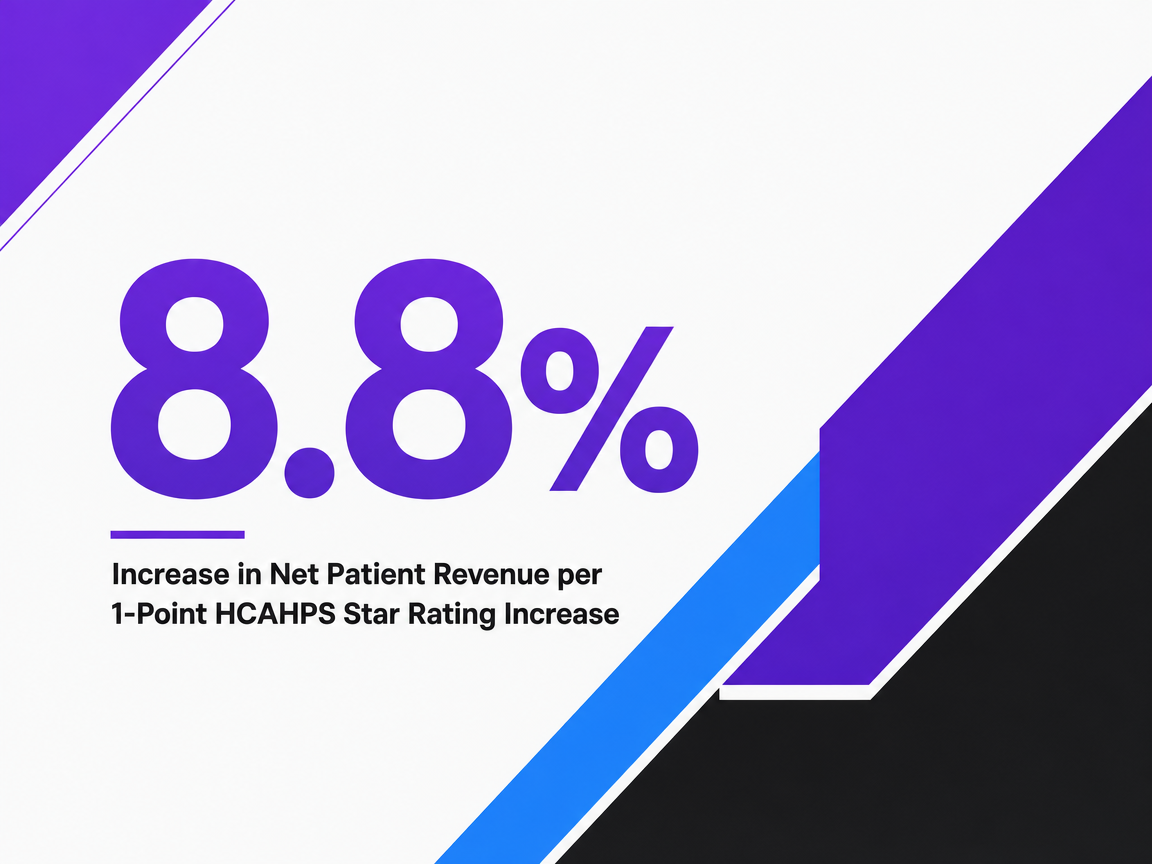 Increase in Net Patient Revenue per 1-Point HCAHPS Star Rating Increase
Increase in Net Patient Revenue per 1-Point HCAHPS Star Rating Increase
Increase in Net Patient Revenue per 1-Point HCAHPS Star Rating Increase
Frequently Asked Questions
References
- 1.Value of patient experience | Deloitte US.
- 2.An Exploratory Analysis of the Association between Hospital Quality Ratings and Hospital Profitability.
- 3.Relationship Between Patient Satisfaction and Hospital Financial Performance.
- 4.Patient Satisfaction with Healthcare Services and the Techniques Used for Its Assessment: A Systematic Review.
- 5.Defining and Implementing Value-Based Health Care.
- 6.HCAHPS: Patients' Perspectives of Care Survey.
- 7.The Impact of Patient Satisfaction on Patient Loyalty with the Mediating Role of Patient Trust.
- 8.Understanding patient satisfaction and loyalty in public and private primary health care.
- 9.Implementing value-based healthcare: a scoping review of key characteristics, challenges, and enablers.
- 10.Patient-reported experience is associated with higher future revenue and lower costs of hospitals.
- 11.Patient-reported experience is associated with higher future revenue and lower costs of hospitals.
- 12.Building Patient Loyalty with Effective Engagement.
- 13.The Impact of Patient Satisfaction on Patient Loyalty with the Mediating Role of Patient Trust (full text PDF).