Key Takeaways
- Patient acquisition functions as an enterprise capability with three measurable components: service-line demand generation, digital access across sites, and conversion tied to booked, retained, value-aligned patients.
- Value-based contracts redefine an acquired patient by outcomes relative to cost, making payer alignment, service-line fit, and retention at twelve months core acquisition criteria 3.
- Multi-site operators carry a coordination tax from consolidation, where per-location agency retainers multiply integration debt across content, keywords, scheduling, and reporting 2.
- Marketing leaders should focus next on building an account-level operating model with a unified metric stack covering cost per acquired patient, cost per attributed life, retention, and outcome performance.
Why a Working Definition Beats a Dictionary Entry
Patient acquisition, defined narrowly, is the set of coordinated processes a health system uses to attract new patients and convert them into active users of its services 1. While technically correct, this definition falls short in the complex reality of a multi-site healthcare operator.
A dictionary entry treats acquisition as a marketing tactic. In contrast, a multi-site reality necessitates treating it as an enterprise function that coordinates demand generation, digital access, scheduling capacity, and care navigation under one account-level plan 4. This work spans service lines, sites, and channels simultaneously, which is why isolated location-level tactics often underperform consumer expectations for healthcare interactions 6.
Marketing leaders equipped with a robust working definition can justify demand budgets, access infrastructure, and conversion measurement systems in executive discussions. Without such a definition, they risk defending ad spend in isolation and losing arguments for necessary headcount and technology investments.
Effective healthcare marketing investigates patient needs and designs services, communication, and delivery models around those needs, rather than merely promoting existing inventory 1. Hospital marketing leaders are increasingly integrating digital strategy with patient care, moving beyond a purely promotional approach 9.
The following section outlines a three-component working definition that is defensible at the executive level and directly translates into measurable infrastructure.
The Three-Component Definition Marketing Leaders Can Defend
Demand Generation: Surfacing Intent at the Service-Line Level
Demand generation is the first measurable component of patient acquisition, focusing on surfacing intent for a specific service line within a particular catchment area, rather than general brand awareness across the entire system.
This distinction is crucial for budget allocation. A health system with 40 sites faces diverse demand challenges, segmented by service line, geography, and payer mix. For example, orthopedic joint replacement demand in a suburban area differs significantly from urgent care demand in a dense urban environment, and both vary from women's health demand driven by OB referrals. Treating these as a single funnel leads to averaged spending that can under-serve high-margin service lines and over-serve saturated ones.
Effective healthcare marketing strategy begins with a thorough investigation of patient needs, then designs services and communication based on these insights 1. For demand generation, this translates into service-line-specific keyword inventories, condition-level content libraries, and paid media segmented by procedure intent rather than facility name.
Hospital marketing leaders are increasingly integrating digital strategy with patient care navigation, moving away from simply pushing location-based ads 9. This shift means demand budgets are defended by service-line economics, not solely by impressions or click-through rates.
Digital Access: The Booking Surface Across Sites
Digital access is the second component, and it is a common point of revenue leakage in multi-site acquisition programs.
Access refers to the booking interface a patient encounters after their intent has been identified. This includes directory listings, provider profiles, online scheduling widgets, telehealth intake, call-center handoffs, and patient portal account creation. Demand without effective access results in wasted spending. For instance, a search ad leading to a location page without real-time scheduling, or a provider profile that doesn't show available appointments within a reasonable timeframe, breaks the acquisition chain before conversion can occur.
The Mayo Clinic Proceedings Digital Health review emphasizes that the ultimate goal of an omnichannel strategy in healthcare is to enhance patient engagement, improve access to care, and reduce costs while improving outcomes 4. This perspective places access on par with demand, recognizing it as an integral part of the acquisition definition, not merely a downstream operational issue.
Telehealth has significantly expanded the access landscape for multi-site operators. Telemedicine platforms can centralize patient records and connect clinicians across various sites, effectively extending the catchment area of each facility and introducing a new acquisition channel independent of physical proximity 7. For systems with uneven specialist coverage, a robust telehealth access layer can be critical for retaining referrals that might otherwise go to competitors.
Conversion to Booked, Retained, Value-Aligned Patients
Conversion is the third component, and it is frequently miscounted.
In patient acquisition, a true conversion is not just a form submission. It is a booked visit that the patient attends, is coded and billed, leads to a follow-up, and aligns with the system's value profile. Marketing dashboards that only track lead submissions measure an event with a weak correlation to revenue. Even dashboards that stop at booked appointments miss no-shows, cancellations, and one-time patients who do not return.
A systematic review of omnichannel communication in JMIR proposes a "digital twin" model that integrates various web-based and offline communication channels throughout the patient journey, linking marketing data with scheduling and care communication data 5. This integration is essential for end-to-end conversion measurement. Without it, marketing reports leads, operations reports visits, and finance reports collections, making it impossible to reconcile these metrics against the same patient cohort.
Multi-site operators face an additional measurement challenge. A patient acquired at an urgent care site who later books an orthopedic consult at a sister site should be counted as one acquired patient with two booking events. Counting this as two acquisitions inflates volume and distorts the cost-per-acquired-patient. A defensible acquisition count uses unique patient identifiers tied to the first encounter across the network, then tracks downstream utilization and retention against that initial event.
Evidence from connected health technology supports that integrated systems facilitate more reliable information flow than fragmented ones 8. This integration is a prerequisite for accurate conversion measurement. The three-component definition is only cohesive when the conversion layer is connected to the same data infrastructure as the demand and access layers.
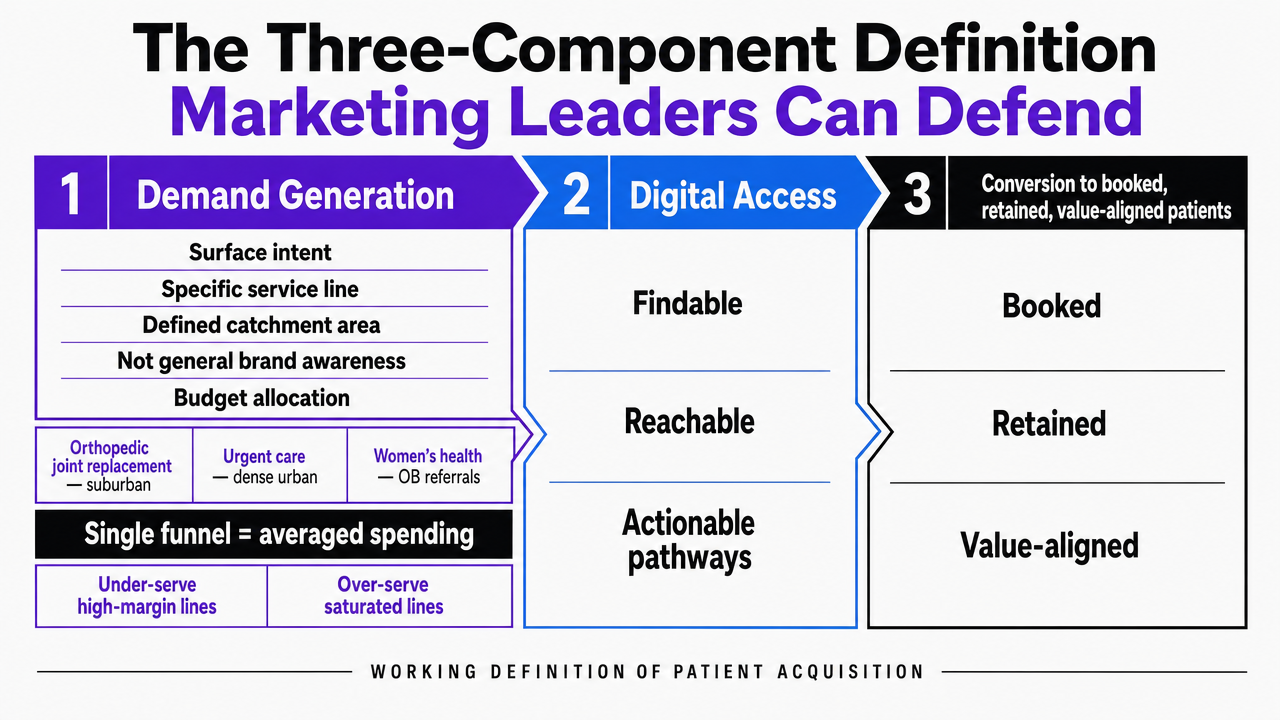 Visualize the three-component working definition of patient acquisition that the section explicitly structures: demand generation, digital access, and conversion to booked, retained, value-aligned patients
Visualize the three-component working definition of patient acquisition that the section explicitly structures: demand generation, digital access, and conversion to booked, retained, value-aligned patients
Value-Based Economics Reshape What Counts as an Acquired Patient
While volume-era acquisition treated every new patient chart as equivalent, value-based contracts introduce a different calculus.
Porter's framework defines value as the measured improvement in a person's health outcomes relative to the cost of achieving that improvement 3. In acquisition terms, a new patient's worth is determined by the outcomes the system can deliver per dollar across their episode or panel, not just the gross revenue from the first visit. An urgent care walk-in acquired via a paid search ad is not the same unit as a Medicare Advantage attributed life acquired through a primary care provider assignment, even if both appear as "one new patient" in a marketing dashboard.
This distinction impacts three operational choices. First, service-line targeting shifts towards conditions where the system demonstrates measurable outcome advantages, as acquiring patients into a losing service line under a capitated contract can destroy value. Second, payer mix becomes a critical acquisition input. Marketing leaders in risk-bearing systems segment paid media and content investments by payer alignment, recognizing that an acquired patient in a misaligned plan could generate a negative contribution margin over the contract year.
Third, retention is no longer a separate function. Under value-based contracts, an acquired patient who churns after four months costs more than they earned, making onboarding, care navigation, and adherence touchpoints integral to the acquisition definition, rather than post-acquisition operations 3.
Multi-site operators experience this most acutely. Consolidation expands the population eligible for value-based attribution, but integration challenges across acquired primary care practices and specialty groups can fragment the outcome measurement required by value-based contracts 2. A marketing leader defending an acquisition budget under risk contracts must demonstrate that spending channels patients into measured, coordinated care pathways, not merely into the next available appointment slot.
The practical metrics evolve accordingly. Cost per acquired patient remains useful, but it is now considered alongside cost per attributed life, retention at twelve months, and outcome performance within contracted conditions. A multi-site acquisition program unable to report on these four metrics collectively is operating on volume-era assumptions within a value-era framework.
Test unified patient acquisition strategy execution now
Experience coordinated, real-time patient acquisition campaigns across all locations with measurable results during your free trial.
The Coordination Tax That Single-Location Definitions Ignore
Consolidation Creates Predictable Integration Failures
Multi-site systems incur a coordination tax that single-location operators do not. This tax manifests as duplicated content, mismatched provider data across directories, conflicting paid media bids between sister sites, and reporting that cannot reconcile a patient across multiple facilities.
The Milbank Quarterly's analysis of community healthcare consolidation highlights that acquisitions of multispecialty and primary care practices by integrated delivery systems follow a common process with predictable integration and operational issues 2. These integration failures are not surprises but recurring patterns that impact acquisition strategy at scale.
For marketing leaders, this has concrete consequences. A system that has acquired twelve primary care practices over three years often operates with twelve different scheduling configurations, eight directory profiles, and four phone trees, each tied to a distinct legacy vendor. Demand generation routed into such an environment converts unevenly by site, not due to differing demand, but because of inconsistent access infrastructure.
Defining acquisition solely as a marketing tactic obscures this coordination tax. Defining it as an enterprise function makes this integration debt visible and assignable to a specific budget owner.
Omnichannel Breakdowns at the Site Boundary
The site boundary is a frequent point of failure for omnichannel strategies, with costs often invisible in standard marketing reports.
The JMIR systematic review on omnichannel communication describes the ideal patient care journey as one where multiple web-based and offline channels are integrated via a "digital twin" that connects all touchpoints 5. In a fragmented multi-site environment, this digital twin is often absent. The marketing channel might know a patient searched for a knee specialist, the scheduling channel at Site A knows the patient called, and the EHR at Site B knows the patient was internally referred for imaging. Yet, none of these systems share a unified record of the patient's journey.
Common breakdown points include:
- a paid search ad for an orthopedic consult leading to a location page without appointment availability;
- a patient calling a central number, being transferred between scheduling teams using different software, and abandoning the process;
- or a patient portal account created at Site A not authenticating at Site B, leading to duplicate accounts and fragmented data.
The Mayo Clinic Proceedings Digital Health review emphasizes improving engagement, increasing access, and reducing costs while improving outcomes 4. This goal is achievable only when handoffs between channels and sites are linked by a shared identifier and queue. Marketing leaders who view omnichannel as merely a campaign theme, rather than an integration specification, will inherit these systemic breakdowns.
Discharge, Referral, and Network Steering as Acquisition Touchpoints
Discharge is an acquisition event, though it rarely appears on marketing dashboards.
CMS discharge planning rules mandate hospitals support interoperability and patient preferences during transitions, with protocols designed to enhance engagement, choice, and continuity of care across settings 10. This regulatory framework highlights that the discharge moment is when a system either guides a patient into its own post-acute network or cedes the relationship to a competitor. Similarly, internal referrals—such as a primary care provider at Site A referring a patient to an orthopedist at Site B—represent an acquired-to-service-line event not generated by paid media.
Multi-site operators who exclude these touchpoints from their acquisition definition under-invest in the operational tools that facilitate effective steering: referral management software, post-discharge follow-up sequences, and provider-facing directories that display in-network specialists with real-time availability. Consequently, the marketing budget bears the full cost of new-patient volume that discharge and referral channels could have produced more cost-effectively.
Channel Reality: Where Human Beats Digital in Acquisition Math
Digital-first agency pitches often dismiss in-person and referral channels as outdated. However, evidence, particularly from recruitment, suggests otherwise.
A 2024 analysis of clinical trial recruitment found that in-person recruitment was the most efficient and cost-effective strategy in its context, with personal referrals being the next most productive channel 11. While this study focuses on research recruitment rather than routine care, the underlying mechanism is transferable: trust-laden, human-mediated interactions convert at higher rates than cold digital impressions when the decision carries significant clinical weight.
For multi-site operators, this points to three underfunded channels:
- provider-to-provider referral relationships between primary care and specialty sites;
- community health events tailored to specific service lines;
- and front-desk and call-center conversion training at the local level, where human interaction often finalizes bookings.
None of these typically appear on a paid media dashboard, yet all generate acquired patients at a lower marginal cost than incremental search spending.
This is not an anti-digital stance; digital channels are essential for surfacing demand at scale 9. Rather, it highlights that an acquisition definition solely focused on digital channels misvalues the human channels that consistently deliver high-intent volume.
Achieve Cohesive Patient Acquisition Across Every Healthcare Location
Connect with our specialists to see data-driven workflows for managing patient acquisition, content, and campaigns under a unified account—purpose-built for multi-site healthcare operators and agencies.
If You Manage Multiple Locations: The Per-Site Retainer Math
Why Per-Location Agency Billing Inflates Coordination Overhead
This section is relevant for operators managing ten or more sites under a shared brand or system. Single-location practices may skip ahead.
The per-location retainer model is structured around how agencies scale revenue, not how patient acquisition scales operationally. An agency billing $X per site per month for SEO, content, and paid media is incentivized to treat each location as a distinct account. This approach leads to multiple content calendars, overlapping keyword strategies for shared service lines, and separate reporting decks that are rarely consolidated into a system-wide view.
The Milbank Quarterly's research on community healthcare consolidation indicates that acquisitions of multispecialty and primary care practices involve predictable integration issues 2. Marketing operations directly inherit these challenges. A system that has continuously acquired new sites often maintains legacy agency relationships, duplicated vendor contracts, and fragmented reporting, all of which the per-location billing model perpetuates.
The coordination overhead is a significant hidden cost. Marketing leaders spend considerable time reconciling site-level reports, mediating between agencies competing for the same branded search terms, and explaining discrepancies in cost per acquired patient across the footprint. This time, though not on any invoice, represents a substantial expense generated by this model.
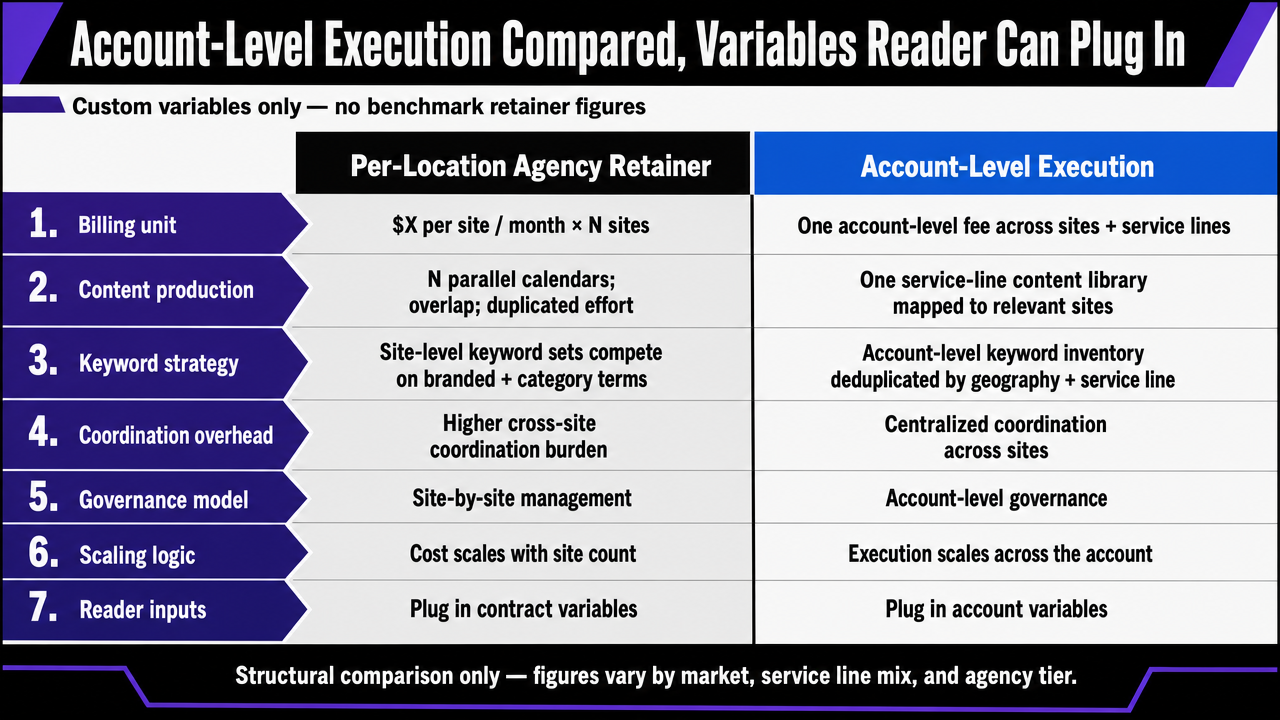
Account-Level Execution Compared, Variables Reader Can Plug In
The following comparison uses variables that operators can customize with their own contract figures. It does not provide benchmark retainer figures, as these vary by market, service line mix, and agency tier. The purpose is to highlight the structural differences, not to offer a fabricated dollar comparison.
| Dimension | Per-Location Agency Retainer | Account-Level Execution |
|---|---|---|
| Billing unit | $X per site per month, multiplied by N sites | One account-level fee covering all sites and service lines |
| Content production | N parallel calendars, overlapping topics, duplicated effort on shared service lines | One service-line content library mapped to all relevant sites |
| Keyword strategy | Site-level keyword sets that compete on branded and category terms | Account-level keyword inventory deduplicated by geography and service line |
| Coordination overhead (internal hours/week) | Scales linearly with N, often 1–3 hours per site for reporting and mediation | Roughly flat regardless of N once the account plan is in place |
| Time-to-publish | Gated by per-site approval loops and per-agency production queues | Single approval workflow and single production queue |
| Reporting | N dashboards, manual roll-up to system view | One unified dashboard at account, site, and service-line cuts |
| Integration with consolidation events | New site triggers new contract, new onboarding, new vendor | New site added to existing plan within the current cycle |
The pattern of consolidation is critical here. Integrated delivery systems acquiring primary care and specialty practices encounter predictable integration issues at every stage 2. A per-location agency model exacerbates these issues, as each acquisition adds another vendor relationship and reporting silo. An account-level model, conversely, integrates new sites into an existing operating plan, mirroring how the rest of the system handles integration.
Operators evaluating these models should calculate the total cost for their footprint: multiply N sites by the current per-site retainer, add internal coordination hours at a fully loaded rate, and compare this total against an account-level fee with a flat coordination cost. The structural advantage of the account-level model grows with the number of sites, making the per-location model particularly inefficient for operators who most need acquisition to function as a system-wide capability.
Platforms like Vectoron implement this account-level execution model for multi-site healthcare operators at a $599/month post-trial price, coordinating strategy, content, SEO, PPC, and backlink work under one plan rather than billing per site.
 Translate the article's comparison table between per-location agency retainers and account-level execution into a scannable side-by-side visual that mirrors the section's seven dimensions
Translate the article's comparison table between per-location agency retainers and account-level execution into a scannable side-by-side visual that mirrors the section's seven dimensions
What a Defensible Acquisition Plan Looks Like at the Executive Table
A defensible acquisition plan addresses three key questions before they are posed by the CFO: what is being acquired, how will it be measured, and where does the spending fit within the operating model.
First, it defines patient acquisition as an enterprise function with three measurable components, rather than a mere marketing line item. Demand generation surfaces service-line intent. Digital access converts that intent into a consistent booking surface across all sites. Conversion links booked, attended visits to unique patient identifiers, tracking retention and outcome performance. Each component has its own budget owner, technology stack, and reporting, making the plan defensible against the common objection that marketing spend cannot be tied to revenue.
Second, the plan presents a comprehensive metric stack, not just a single number. Cost per acquired patient is considered alongside cost per attributed life, retention at twelve months, and outcome performance within contracted conditions, reflecting that value-based contracts measure improvement in health outcomes relative to cost 3. A plan reporting only volume operates on outdated, volume-era assumptions.
Third, the plan addresses the operating model. Per-location vendor relationships perpetuate the integration debt inherent in consolidation 2. An account-level execution model integrates new sites into a single plan, content library, keyword inventory, and reporting interface. Marketing leaders presenting this structure can justify headcount and technology investments by demonstrating a more efficient alternative to compounding agency retainers across an expanding footprint.
Platforms like Vectoron offer this account-level model for multi-site healthcare operators, coordinating strategy, content, SEO, PPC, and backlink execution under one plan at a $599/month post-trial price.
Frequently Asked Questions
References
- 1.The impact of marketing strategies in healthcare systems.
- 2.The Dynamics of Community Health Care Consolidation: Acquisition of Primary Care Practices in the Midwestern United States.
- 3.Defining and Implementing Value-Based Health Care.
- 4.An Overview of Omnichannel Interaction in Health Care Services.
- 5.Omnichannel Communication to Boost Patient Engagement and Retention: A Systematic Review.
- 6.Driving growth through consumer centricity in healthcare.
- 7.Telemedicine for healthcare: Capabilities, features, barriers, and applications.
- 8.Connected Healthcare System Technology Interventions to Improve the Quality of Healthcare: A Literature Review.
- 9.SHSMD23 Puts Digital Marketing Strategy and Its Role in Patient Care in the Spotlight.
- 10.CMS’ Discharge Planning Rule Supports Interoperability and Patient Preferences.
- 11.Successes and Challenges in Clinical Trial Recruitment.