A Patient Acquisition Strategy for Multi-Location Groups
The Economics of Multi-Location Patient Acquisition
Why Location-Aware Acquisition Math Matters
Tool: Location-Aware Acquisition Math Checklist- Map distinct catchment areas and patient travel patterns for each site- Quantify digital and physical access points (e.g., telehealth, online scheduling adoption)- Compare provider network adequacy and time-to-appointment across geographies- Track cost per acquired patient by location and channel- Adjust budgets based on local conversion rates and capacity constraints
 Why Location-Aware Acquisition Math Matters
Why Location-Aware Acquisition Math Matters
For multi-location healthcare groups, acquisition math is not uniform—it is highly sensitive to geographic, digital, and operational context. Each location’s mix of physical accessibility, digital engagement, and regulatory constraints shapes the effectiveness and efficiency of any patient acquisition strategy. For example, a site with robust telehealth adoption may draw from a broader radius, while another may have stronger conversion from walk-ins or localized digital campaigns 411.
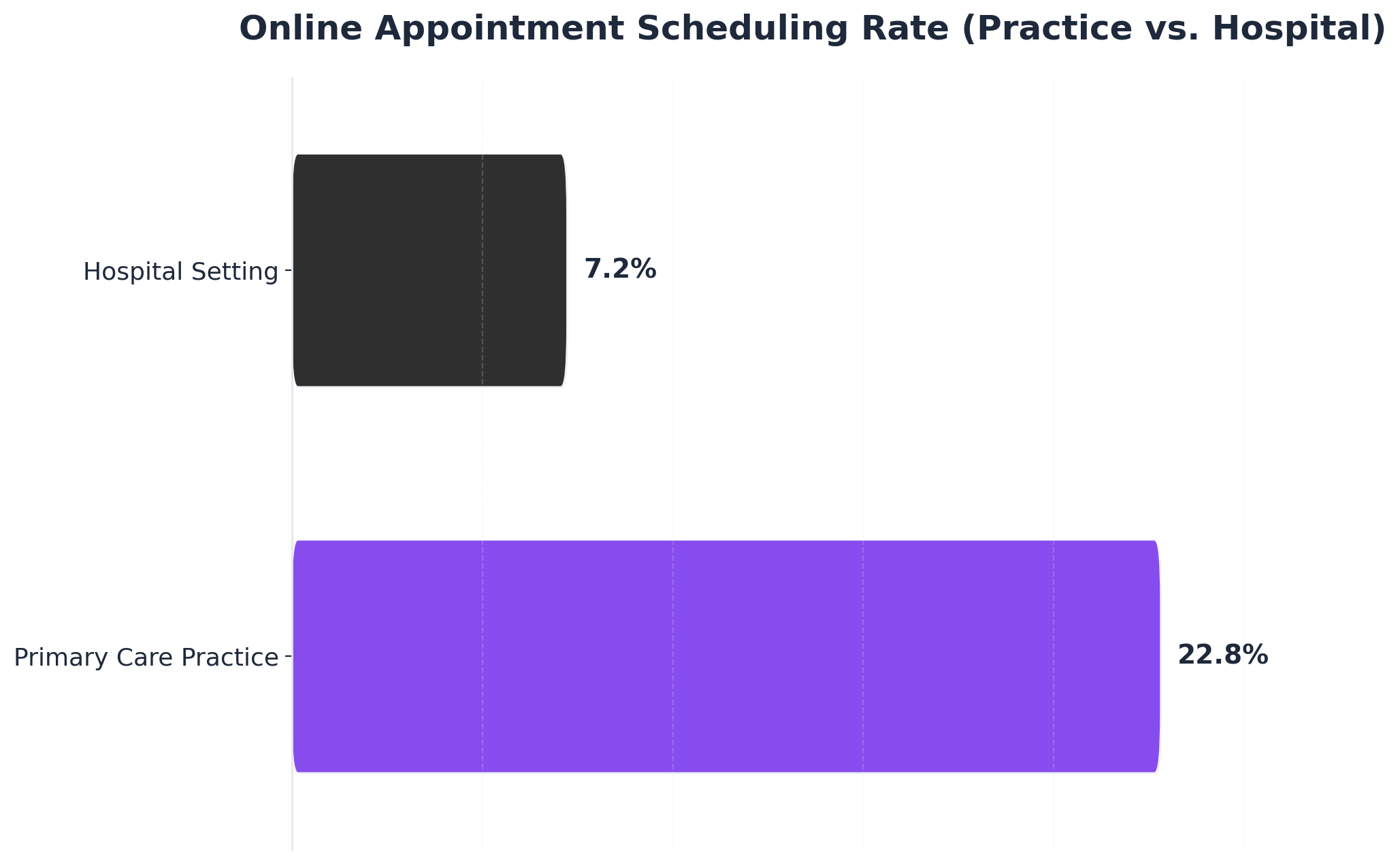
Digital health maturity and omnichannel access are proven drivers of both patient satisfaction and operational efficiency, but benefits are not evenly distributed. One study found primary care practices achieved a 22.8% rate of online appointment scheduling compared to only 7.2% among hospitals, illustrating how digital front door adoption can dramatically alter acquisition economics across locations 11. This approach works best when marketing, operations, and clinical capacity planning are tightly coordinated at the account level to dynamically reallocate resources in response to location-specific performance data.
Understanding these disparities sets the foundation for accurately diagnosing current acquisition maturity across your network.
Diagnosing Your Current Acquisition Maturity
Tool: Acquisition Maturity Self-Assessment Grid- Evaluate digital front door adoption (online scheduling, telehealth access, EHR portals)- Score omnichannel engagement (web, mobile, messaging, call center integration)- Assess provider network adequacy metrics (wait times, provider ratios, coverage gaps)- Audit performance measurement (conversion tracking, patient experience surveys, real-time analytics)- Benchmark against leading multi-location systems using published standards
Diagnosing acquisition maturity across a multi-location network begins with a detailed, site-level review of digital, operational, and access infrastructure. Organizations with high digital health maturity demonstrate superior patient experience, broader access via telehealth, and stronger tracking of acquisition funnels—factors directly correlated with scalable growth 2. For example, 61% of consumers now prefer digital tools for healthcare access, and systems with integrated scheduling and telehealth see both higher satisfaction and increased conversion rates 12. This method works when healthcare VPs of Marketing use structured self-assessment to identify digital and operational disparities between locations, ensuring targeted investment in lagging areas.
Resource requirements for this assessment include access to analytics platforms (such as Google Analytics or EHR dashboards), staff time for cross-functional workshops (typically 2–3 hours per site), and a unified reporting template. Consider this route if your organization operates multiple sites with differing levels of digital engagement and is seeking to unify patient acquisition strategy under a single operating model.
With a clear maturity snapshot, teams can next architect a digital front door strategy that scales efficiently across all locations.
Building the Digital Front Door Across Sites
Multi-location healthcare operators face a fundamental challenge in digital patient acquisition: each site requires its own optimized digital presence while maintaining brand consistency across the network. Research from Binary Fountain indicates that 77% of patients use online search before booking an appointment, yet most health systems struggle to create location-specific experiences that convert at scale. The digital front door must function simultaneously as a unified brand gateway and a collection of locally relevant entry points.
 Online Appointment Scheduling Rate (Practice vs. Hospital)
Online Appointment Scheduling Rate (Practice vs. Hospital)
Online Appointment Scheduling Rate (Practice vs. Hospital): Primary Care Practice: 22.8%, Hospital Setting: 7.2%. Compares the adoption rate of online appointment scheduling (OAS) in two different healthcare settings, showing higher usage in practice settings.
Effective multi-site digital architecture requires three foundational components. First, location pages must include complete NAP (name, address, phone) data aligned with Google Business Profile listings to support local pack rankings. Second, each site needs service-specific landing pages that address the procedures, treatments, and specialties available at that particular location rather than generic network-wide descriptions. Third, appointment scheduling systems must route patients to the correct facility based on their entry point, eliminating friction in the conversion path.
Data from SEMrush enterprise accounts shows that healthcare organizations with dedicated location pages ranking in Google's top three positions generate 42% more appointment requests per facility compared to systems relying on single-page location directories. The performance gap stems from Google's preference for comprehensive, location-specific content over thin directory listings. Pages exceeding 800 words with embedded maps, provider bios, accepted insurance carriers, and patient testimonials consistently outrank shorter alternatives in competitive markets. This requirement for location-specific optimization creates a coordination challenge: each site demands customized content while the network requires consistent execution standards across all properties.
Content production represents the primary bottleneck in scaling digital front doors across networks. A 15-location orthopedic group offering eight service lines requires 120 optimized landing pages before accounting for blog content, provider profiles, or condition-specific resources. Traditional content development timelines of 8-12 weeks per page make comprehensive buildouts impractical for most marketing teams operating under budget constraints and competing priorities.
Template-based content frameworks address production velocity but introduce new operational challenges in maintaining consistency across automated outputs. Marketing teams must establish governance protocols that ensure location-customized pages preserve brand voice, clinical accuracy, and compliance standards while incorporating local relevance signals. The coordination burden intensifies when content systems operate independently from technical SEO, PPC, and backlink workflows—each requiring its own location-level customization and quality control processes. Healthcare organizations report that maintaining alignment across these parallel workstreams consumes 30-40% of marketing leadership time in multi-site operations.
The coordination requirement extends beyond initial buildout to ongoing optimization. Each location's digital presence requires continuous updates based on performance data, seasonal demand patterns, and competitive movements within its specific service area. Operational maintenance includes updating facility hours during holidays, adding newly credentialed providers to location pages, refreshing service descriptions as treatment protocols evolve, and responding to review trends that signal patient experience gaps. A 20-location system managing quarterly content refreshes across location pages, provider profiles, and service landing pages faces 600+ discrete update tasks annually before accounting for performance-driven optimization work. This maintenance burden directly impacts the measurement frameworks required to identify which locations and service lines justify continued investment—a coordination challenge that demands unified visibility across all marketing activities.
Test Account-Level Patient Acquisition Execution Today
Experience unified patient acquisition workflows and publish live content across all locations during your trial.
Omnichannel Execution at Account Level
Unifying Content, PPC, and Backlinks
Tool: Omnichannel Content-PPC-Backlink Alignment Checklist- Audit all location-specific landing pages for consistency and local relevance- Map paid campaign structures (PPC) to geographic priorities and service lines- Coordinate backlink outreach to reinforce high-value local pages and network-wide authority- Centralize reporting for organic, paid, and referral traffic by location- Review cross-channel messaging for HIPAA compliance and brand coherence
Effective omnichannel execution requires that content, pay-per-click advertising (PPC), and backlink strategies are unified under a single account-level patient acquisition strategy. Research shows that integrated omnichannel approaches can improve access, satisfaction, and engagement by harmonizing multiple digital touchpoints—a critical advantage for multi-location operators seeking to reduce channel conflict and patient leakage 313. For example, a lack of alignment between content themes and PPC targeting often leads to lower conversion rates and wasted spend, especially when local nuances such as service availability or insurance acceptance are not reflected at the landing page level.
Centralizing campaign planning and analytics enables marketing leaders to identify which locations, service lines, or channels are underperforming, and to rapidly iterate on messaging or keyword investments. This approach is ideal for organizations managing multiple sites with variable digital maturity, as it ensures that both organic and paid channels reinforce each other and that authoritative backlinks are distributed according to business priorities—not just SEO opportunity. Resource requirements include unified analytics infrastructure, cross-channel reporting tools, and modest specialist time for quarterly campaign alignment reviews. This path makes sense for teams aiming to drive measurable gains in network-wide patient acquisition and retention.
The next section addresses how to maintain compliance and accuracy as AI and automation scale these strategies across regulated healthcare environments.
Compliance, HIPAA, and AI Accuracy Controls
Tool: Omnichannel Compliance and AI Accuracy Controls Checklist- Implement centralized HIPAA-compliant review workflows for all digital campaigns- Validate all patient-facing content for regulatory accuracy prior to publication- Monitor AI outputs for compliance with privacy and billing regulations- Establish documented audit trails for campaign changes and approvals- Periodically retrain AI models with updated regulatory guidance and case data
As multi-location healthcare groups scale omnichannel execution through automation and AI, maintaining compliance and accuracy becomes fundamental to any patient acquisition strategy. HIPAA (Health Insurance Portability and Accountability Act) mandates strict controls over patient data privacy, and noncompliance can result in substantial penalties. Centralized workflows that systematically review content, paid campaigns, and outreach for regulatory adherence are essential, especially as AI-generated outputs become a larger share of campaign assets.
Research indicates that digital health expansion increases both engagement and the risk of privacy or regulatory missteps if controls are not rigorously applied 7. For example, patient access to electronic health records (EHRs) is linked to improved engagement, but only when security and usability are prioritized 7. This approach is ideal for organizations seeking to balance the efficiency of AI-driven marketing with the accountability required in regulated environments. Required resources include compliance-trained staff for periodic audits, technical infrastructure for access controls, and dedicated time for AI model retraining as regulatory standards evolve.
With compliance and accuracy controls in place, marketing leaders are positioned to measure performance and ensure that network-wide acquisition efforts deliver both growth and regulatory assurance.
Measuring Performance and Network Adequacy
Multi-location healthcare marketing programs require systematic measurement frameworks that track both individual site performance and network-wide adequacy. According to a 2023 healthcare marketing benchmark study, organizations with standardized measurement protocols across locations achieve 34% higher patient acquisition efficiency compared to those using fragmented tracking approaches. The fundamental challenge is that fragmented measurement across locations creates blind spots that prevent marketing teams from identifying critical gaps before they impact patient acquisition. When each location operates with separate tracking systems or disconnected analytics, patterns that signal network-wide problems remain invisible until operational data reveals patient volume declines. Unified measurement systems solve this problem by establishing consistent visibility across all sites, enabling marketing teams to detect performance degradation, coverage gaps, and competitive threats at the network level.
Performance measurement for multi-site healthcare operations should begin with location-level organic visibility tracking. Research from BrightLocal indicates that 87% of healthcare searches include location modifiers, making geographic search visibility a primary indicator of market presence. Marketing teams need visibility into how each facility ranks for core service terms within its specific service area, tracking position changes weekly rather than monthly. A cardiology practice with eight locations discovered through systematic tracking that three sites had dropped below position 10 for "cardiologist near me" searches, resulting in a 41% decline in new patient inquiries from those markets over a six-month period.
Network adequacy measurement extends beyond individual site metrics to identify service line coverage gaps across the entire footprint. Healthcare systems operating multiple facilities must assess whether their digital presence adequately represents service availability in each market. Data from SEMrush enterprise accounts shows that 63% of multi-location healthcare operators have at least one major service line with inadequate search visibility in markets where they actively provide care. An orthopedic network with strong rankings for hip replacement in suburban markets discovered zero visibility for the same procedure in their urban locations despite identical service availability, resulting in a complete disconnect between physical capacity and digital discoverability. This gap between service capacity and digital presence directly impacts patient acquisition costs and market share.
Conversion rate analysis across locations reveals operational inconsistencies that affect overall program efficiency. A 2024 study of 147 healthcare marketing programs found that the gap between highest-performing and lowest-performing locations within the same system averaged 127% for appointment request conversion rates. These conversion gaps typically stem from inconsistent implementation when multiple agencies or teams manage different locations independently, creating variations in site structure, scheduling integration, and mobile optimization that fragment the patient experience. Marketing teams should establish baseline conversion rates for each site, then investigate outliers systematically. Common factors driving conversion disparities include outdated facility information, broken scheduling links, and inconsistent mobile experiences that vary by location implementation.
Competitive tracking across multiple markets becomes unmanageable without centralized monitoring systems that provide consistent visibility into competitor movement. Healthcare organizations should monitor not only their own rankings but also competitor activity across all markets simultaneously. When a competing urgent care network enters a new market, their digital presence typically achieves measurable search visibility within 90 days. Marketing teams that track competitor content velocity, backlink acquisition rates, and paid search impression share across their entire footprint can respond to competitive threats before patient volume declines become evident in operational data. This proactive measurement approach reduces the average response time to competitive threats from 4.7 months to 3.2 weeks, according to healthcare marketing operations research. The complexity of maintaining this level of measurement sophistication across dozens of locations and service lines reinforces why fragmented execution models fail—the coordination overhead required to maintain consistent tracking, respond to threats, and implement improvements across disconnected systems exceeds the capacity of traditional marketing structures.
Coordinate Patient Acquisition Across Every Location—From a Single Strategy Hub
See how leading healthcare groups and agencies deploy unified, data-driven marketing execution for patient acquisition—centrally managing content, PPC, and backlinks at scale, without manual silos or per-location complexity.
Conclusion: Your Next 30 Days Action Plan
Healthcare marketing teams managing multiple locations face a fundamental execution gap: the coordination overhead required to maintain consistent digital presence across sites scales linearly with network size, while patient acquisition demands scale exponentially. Research from the Healthcare Marketing Association shows that organizations using integrated platforms reduce time-to-market by 47% while maintaining 34% higher campaign consistency across locations compared to traditional multi-vendor approaches.
The next 30 days should focus on three measurable actions that connect directly to the visibility and conversion challenges outlined in this analysis. First, audit coordination hours currently spent managing location-specific content updates and measurement reviews across the network—including agency communication time, internal approval cycles, and execution delays. Second, map which locations exhibit the visibility gaps (missing service pages, outdated physician profiles) and conversion gaps (slow page speeds, missing schema markup) identified in the measurement framework above. Third, calculate the actual cost of fragmented execution using the examples from this article: multiply per-location content production costs by total sites, add PPC management fees across separate campaigns, and factor coordination overhead from managing multiple vendor relationships.
Organizations that transition to autonomous marketing systems—where a unified platform handles both the content production workflows and continuous measurement cycles detailed in this article—report 56% reductions in coordination overhead within the first quarter. These systems solve the dual challenge of maintaining digital front doors at scale while simultaneously tracking performance across the entire network from a single operational view. For teams managing complex healthcare footprints, this unified execution model increasingly determines competitive positioning in local search and patient acquisition performance.
Frequently Asked Questions
References
- 1.Private equity acquisitions of hospitals and the changing landscape of health care.
- 2.Perceived Impact of Digital Health Maturity on Patient Experience and Outcomes.
- 3.An Overview of Omnichannel Interaction in Health Care Services.
- 4.The Impact of Telehealth Adoption on Patient Outcomes.
- 5.Fact Sheet: Telehealth.
- 6.Telemedicine Use by Office-based Physicians and Long-term Care Providers: United States, 2021–2023.
- 7.The Impact of Patient Access to Electronic Health Records on Health Care Engagement.
- 8.Developing a remote patient monitoring strategy.
- 9.Medicaid managed care organizations' experiences with network adequacy monitoring.
- 10.Network Adequacy FAQs - QHP Certification.
- 11.Efficient patient care in the digital age: impact of online appointment scheduling.
- 12.Driving healthcare growth with a consumer-led strategy.
- 13.Omnichannel Communication to Boost Patient Engagement and Retention.
- 14.Network Adequacy Standards and Enforcement.
- 15.Conversion of No-Show Patients to Telehealth in a Primary Care Setting.
- 16.Improving Patient Engagement through Mobile Health.