Key Takeaways
- Retention across multi-site networks is determined by structural design—panels, scheduling, records portability, and experience consistency—rather than by marketing campaigns or loyalty programs layered on top.
- Four compounding levers drive retention: relational continuity, information portability under the 2024 CMS rules, access friction from prior authorization, and experience consistency across sites 9, 5, 2.
- Operators must design for three coordination layers—within primary care, primary-to-specialist, and cross-sector—because referral patterns and structural choices, not promotions, determine where leakage occurs 6, 12.
- Above five locations, per-site vendor models fragment messaging and reporting; an account-level operating model that reduces cross-site variance is where multi-location leaders should focus next 11, 12.
Retention is a network design problem, not a campaign problem
Most articles on patient retention focus on marketing tactics like appointment reminders or loyalty programs. While these can be effective for single-site practices, retention in multi-site organizations (e.g., a 12-site primary care group or an 80-clinic dermatology platform) behaves differently. It shifts from being a campaign outcome to a property of the network itself.
Research supports this view: continuity of care is linked to reduced mortality, fewer hospital admissions and emergency department visits, lower total cost of care, better adherence, and stronger patient-clinician relationships 9. These outcomes stem from long-term relationships, stable organizational routines, and shared information systems across sites 1. A patient who consistently sees a familiar clinician, whose records are accessible across locations, and who can schedule appointments without repeatedly providing their history is more likely to be retained. Conversely, a patient who encounters friction in these areas is prone to leakage.
This perspective redefines operational priorities. The key levers are structural: how patient panels are built, how scheduling directs patients across sites, how records are managed under the 2024 CMS interoperability and prior authorization rules 5, and how consistent the access and communication experience is across all clinics 2. Network designers have historically modeled leakage based on network configuration, referral patterns, and provider incentives, rather than promotional efforts 12.
This article examines retention as a network design challenge, focusing on four compounding levers, three coordination layers, and a unit-economics model that becomes critical for networks exceeding five locations. Marketing campaigns are supplementary; they do not replace this foundational architecture.
The four compounding levers behind multi-site retention
Retention in a multi-site network is a complex interplay of four interconnected levers:
- relational continuity between patient and clinician,
- information portability across sites,
- access friction in scheduling and authorization, and
- consistent patient experience across all clinics.
These levers are interdependent; improving one in isolation yields limited gains, while neglecting one can undermine progress in others.
Each lever is critical. Continuity is strongly associated with improved patient outcomes 9. Patient experience, as defined by AHRQ, encompasses timely appointments, information access, and communication quality 2. Information portability is now mandated by federal regulations 5. Network design research consistently links leakage to structural choices, not just marketing 12. The following subsections detail each lever and its operational implications for executives.
Relational continuity as the dominant retention lever
Relational continuity has the strongest evidence base and largest impact on retention, yet it is often underestimated by operators who view it merely as a quality metric. A comprehensive review highlights that higher continuity correlates with reduced mortality, fewer hospital admissions and emergency department visits, lower total costs, improved preventive care, better adherence, enhanced quality of life, and stronger patient-clinician relationships 9. These are not minor benefits; they are the precise outcomes that determine whether a patient remains engaged with a provider or seeks care elsewhere.
The mechanism is clear: a patient who has seen the same clinician multiple times has already invested in building trust and explaining their health history. Switching to a new clinician necessitates restarting this process. In a single-site practice, this might happen infrequently. However, in a large multi-site network, this reset can occur every time a patient calls and is routed to the next available provider. Prioritizing "next-available" scheduling over clinician-matching is a structural decision that, in terms of continuity, leads to gradual patient leakage.
Achieving continuity also requires organizational support, including long-term, person-centered relationships, stable organizational structures, and shared responsibility for cohesive care 1. For multi-location operators, this means continuity is not solely dependent on individual clinicians but on the routines that support them: how panels are structured, how provider tenure is protected, how care teams are assigned, and how information is shared between visits. High clinician turnover, for example, can rapidly erode continuity, negating any patient communication efforts.
Consequently, continuity should be a key executive scorecard metric, not just a clinical quality addendum. Retained patients with continuous clinician relationships incur lower service costs, utilize fewer high-acuity services, and remain within the network 9. Those without such continuity are more likely to leave. The financial benefits of retention are directly tied to effective panel management.
Information portability under the 2024 CMS rules
What was once an aspiration is now policy. The Advancing Interoperability and Improving Prior Authorization Procedures final rule, effective in 2024, mandates expanded electronic health data exchange and streamlined prior authorization for various health plans 5. This, combined with the earlier Interoperability and Patient Access rule, requires standards-based patient-access APIs for key payers, enabling payer-to-payer data exchange upon patient request 3. Impacted payers must provide claims, encounters, and clinical data via FHIR-based APIs 4.
For multi-site operators, this significantly enhances operational capabilities. A patient transferring between clinics within the same network no longer needs a complete data restart. Their claims history, encounter data, and clinical information can follow them, provided the network's intake, scheduling, and clinical systems are integrated to receive this data. The federal standard for portability is established; realizing its retention benefits depends on internal system integration.
Operators should note two important caveats. First, payers are only required to share data they maintain, meaning data completeness will vary 4. Networks relying on fully complete records may encounter gaps. Second, while the policy strengthens access and portability, it does not automatically solve clinical workflow challenges or ensure adoption at the practice level 3. Standards-based APIs alone do not change daily front-desk procedures for transferring patients.
The link to retention is direct: information portability reduces the time from a patient's decision to seek care to receiving it, and it eliminates a common reason for patients to re-explain their history. A network that effectively operationalizes cross-site portability transforms what was a new-patient workflow into a continuing-patient workflow. The continuity benefits documented in clinical literature 9 are amplified when patient records seamlessly follow them.
Access friction and the prior-authorization tax on retention
Access friction is frequently misdiagnosed by operators. While missed appointments or unfilled slots are visible symptoms, the root cause often lies in a series of administrative hurdles: a referral requiring prior authorization, a week-long authorization process, a missed return call, or a competing provider offering an immediate appointment.
The 2024 rule directly addresses this by streamlining prior authorization through standardized electronic workflows 5. This aims to reduce administrative delays between a patient's decision to seek care and its receipt. The retention impact is quantifiable, even if not yet precisely measured: every day an authorization is delayed is an opportunity for a patient to be diverted to a competitor offering faster access, more responsive scheduling, or a timely marketing offer.
Continuity research reinforces this point: continuity is linked to fewer emergency department visits and hospitalizations because patients who can quickly reach their existing care team are less likely to escalate to higher-acuity services 10. When access friction impedes this, patients seek alternatives, either through an ED visit or a competitor, both resulting in leakage for the operator.
For multi-location executives, the operational decision is whether to treat prior authorization and referral processing as a back-office function or a retention function. A back-office approach prioritizes cost per authorization. A retention-focused approach prioritizes time-to-resolution and patient-visible status updates. The 2024 rule reduces the technical barriers to the latter 5. Networks that maintain a purely back-office perspective will continue to incur the costs of access friction.
Experience consistency across sites, not satisfaction theater
The fourth lever requires distinguishing between patient experience and patient satisfaction, a distinction AHRQ emphasizes but many retention programs overlook 2. Experience refers to objective occurrences: timely appointments, accessible information, and effective communication with clinicians and staff 2. Satisfaction is the patient's subjective rating of whether their expectations were met. While correlated, they are not interchangeable and respond to different interventions.
This distinction is crucial because most multi-location retention budgets are allocated to satisfaction metrics like post-visit surveys and NPS dashboards, which measure perception. True experience is shaped by underlying operational factors: phone answer times, whether after-visit summaries are received, or if appointment availability matches online promises. AHRQ considers experience improvement a core quality activity 8. For multi-site operators, it is also where retention is secured or lost between visits.
The retention payoff varies by setting. A study of primary care centers found a strong correlation between satisfaction and loyalty in private centers (r = 0.767) and a moderate correlation in public centers (r = 0.54) 11. This differential is significant for private and quasi-private multi-location operators (e.g., MSO-backed specialty platforms, DSO networks), where experience-driven loyalty has the strongest empirical impact.
Operationally, the goal is experience consistency across sites, not just high average satisfaction. A network with a 4.7 average rating that masks a 4.9 at flagship sites and a 4.1 at underperforming sites is leaking patients from the latter. Variance signals leakage. A retention program for a large multi-site operator should focus on reducing variance in metrics like phone answer times, appointment availability, communication completeness, and visit punctuality, measured uniformly across all sites and reported to a single executive.
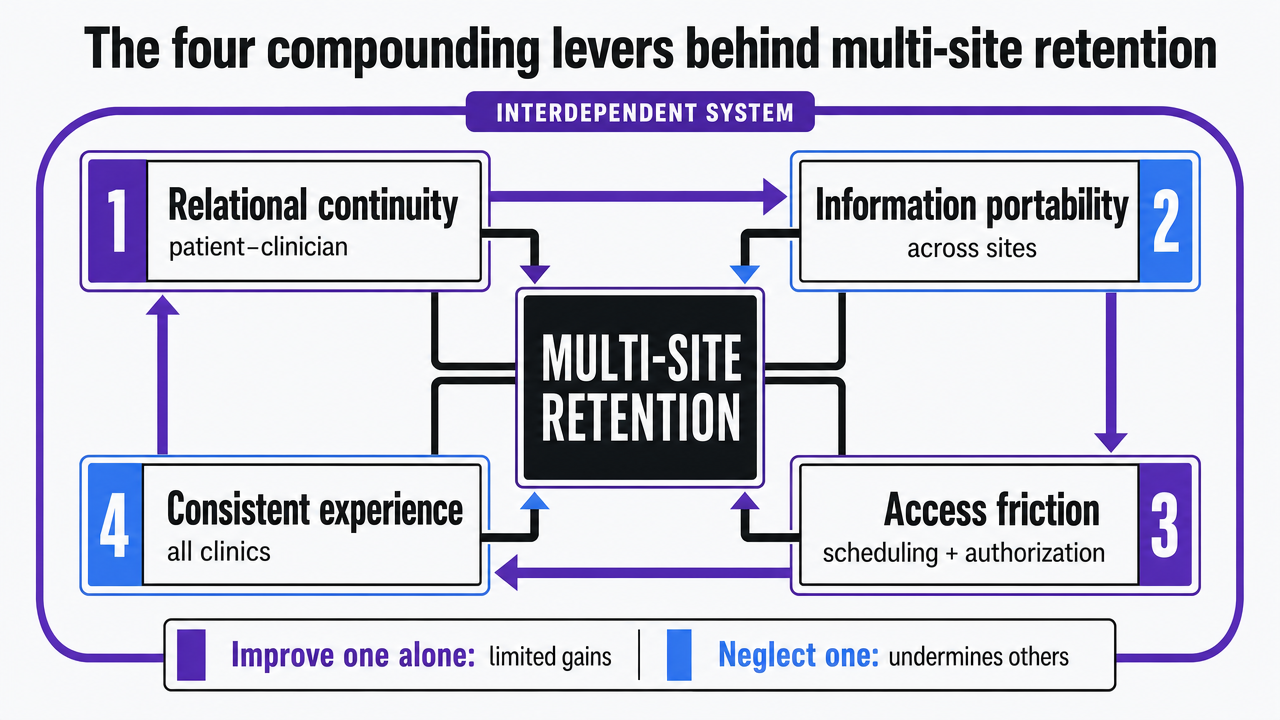 Visualize the four interdependent retention levers introduced in this section as a framework diagram, directly supporting the section's core construct
Visualize the four interdependent retention levers introduced in this section as a framework diagram, directly supporting the section's core construct
Test real patient retention strategies risk-free
Evaluate measurable retention improvements across locations with live content deployed during your trial period.
Three levels of coordination operators must design for
A 2023 review of continuity and care coordination in primary health care provides a structural framework for retention. It identifies three levels of coordination: within primary care, between primary care and specialists, and across sectors. Higher coordination at each level is associated with reduced fragmentation, better adherence, less duplication, and improved patient satisfaction 6. For multi-site operators, these levels directly correspond to common points of patient leakage.
Within-primary-care coordination is the first level, most directly controlled by operators. This involves how a patient's care transitions between different providers (e.g., family medicine, behavioral health, nurse care manager) and administrative staff within the same site or across sister sites in the network. For instance, if a patient is routed from one clinic to another for an earlier appointment, effective within-primary-care coordination ensures the receiving team has access to their active problem list, recent medication changes, and pending follow-ups. Weakness at this foundational layer propagates throughout the system 6.
Primary care to specialist coordination is where many multi-location networks experience significant, often unnoticed, leakage. A patient referred from an in-network primary care provider to an out-of-network specialist (e.g., dermatologist or orthopedic group) is unlikely to return to the original network for subsequent needs. Network leakage research explicitly models referral patterns and incentive design as primary determinants of whether a patient remains within the system 12. For specialty platforms, the operational question is whether referral workflows default to in-network specialists with confirmed availability or rely on individual clinician memory. This default setting is a critical retention factor.
Cross-sector coordination involves transitions between the ambulatory network and other settings, such as hospitals, post-acute care facilities, pharmacies, and social services. Operators often perceive this as outside their control, but it is not. The scoping review links coordination at this level to reduced fragmentation and improved outcomes 6. These improvements influence whether a patient returns to the ambulatory network after a hospitalization or opts for a competing system that managed the handoff more effectively. The 2024 federal rules on electronic data exchange and prior authorization reduce the technical barriers to achieving this level of coordination 5.
Operators should map their network's coordination performance against each of these three levels independently. A multi-site dental organization with strong internal coordination but poor primary-to-specialist referral capture faces a different leakage problem than a primary care group with strong referral capture but weak hospital-to-ambulatory handoffs. The necessary interventions are distinct. Treating coordination as a single metric on a dashboard can obscure the specific points where patients are leaving the network.
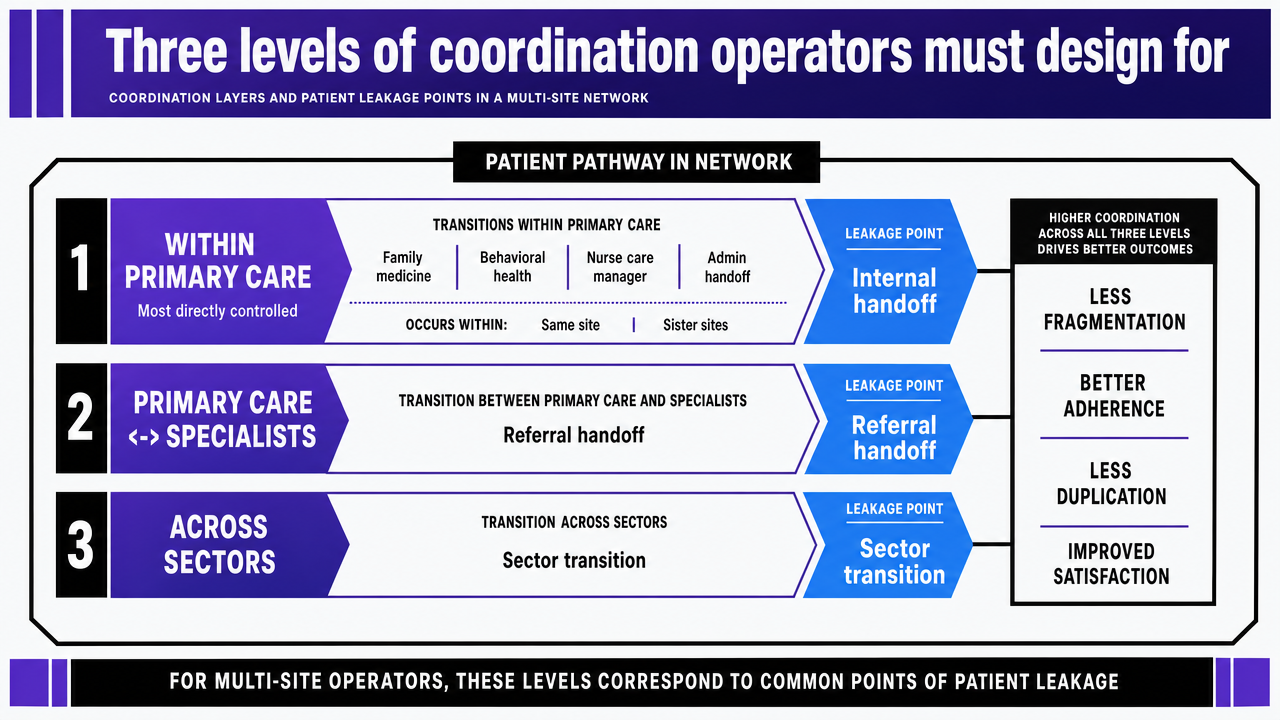 Visualize the three coordination layers cited from the 2023 scoping review, showing how each layer corresponds to different leakage points in a multi-site network
Visualize the three coordination layers cited from the 2023 scoping review, showing how each layer corresponds to different leakage points in a multi-site network
The unit economics of retained patients above five locations
The economics of patient retention differ significantly between a five-site network and a fifty-site network. For smaller networks, a marketing manager and a few vendors can manage retention through email campaigns and recall lists. However, beyond five to ten locations, the per-site coordination model typically breaks down. This leads to a proliferation of vendors, fragmented reporting, increased message inconsistency, and a rising marginal cost per retained patient, even as the network expands.
The underlying structural issue is that per-site vendor models bill against individual sites, not the patient's entire journey. A patient who begins care at one site, has a referral processed by another, and schedules a follow-up at a third interacts with multiple vendor surfaces that lack a unified plan, calendar, or measurement framework. Network leakage modeling identifies this fragmentation as a primary control variable: referral patterns and structural choices, rather than individual site promotions, determine patient retention 12. When coordination is managed site-by-site, it is inherently localized, lacking a cohesive network-level design.
The table below illustrates the contrast between per-site and account-level coordinated models, using variables rather than specific dollar figures, as industry benchmarks for customer acquisition cost (CAC) or retention lift are not provided in the cited research. The "Retention impact" column reflects findings from continuity and satisfaction-loyalty literature 9, 11.
| Cost driver | Per-site vendor model | Account-level coordinated model | Retention impact |
|---|---|---|---|
| Marketing and content | N locations × per-site retainer | Single account fee covering all sites | Consistent messaging reduces experience variance across sites 2 |
| Referral and authorization workflow | Site-level back office, site-level vendors | Network workflow standard across sites | Lower friction shortens time-to-care, reducing patient substitution to competitors 5 |
| Patient communication | Per-site tools, varied cadence | One cadence, one measurement frame | Reduced variance correlates with satisfaction-driven loyalty in private settings 11 |
| Reporting and attribution | N dashboards, manual rollup | Account-level view across sites | Leakage visible at the network layer, not buried in site reports 12 |
Two key findings underpin the benefits of an account-level approach. First, continuity is associated with fewer hospital admissions and emergency department visits, and lower total costs 9, meaning retained patients are less expensive to serve over time. Second, satisfaction and loyalty are strongly correlated in private primary care settings 11, indicating that consistent experience directly translates to higher retention rates in the types of multi-location networks most likely to exist. Per-site vendor models inherently work against these effects.
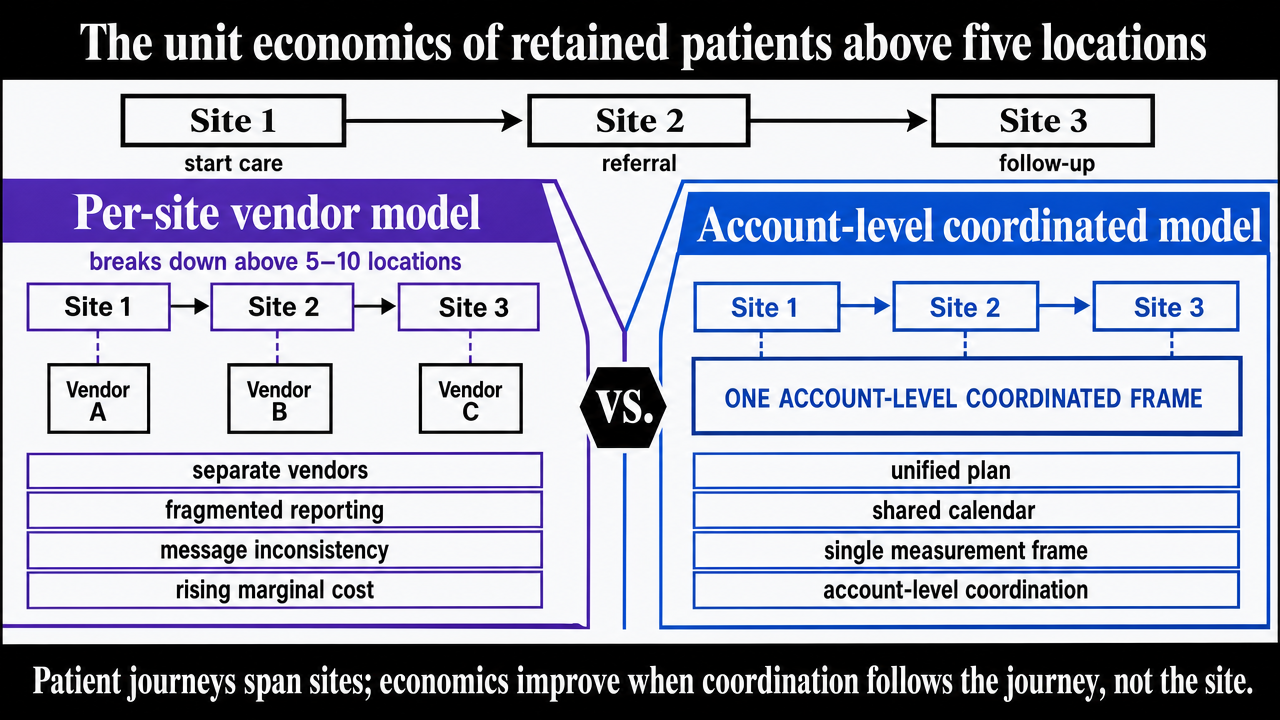 Visualize the comparison table contrasting per-site vendor model versus account-level coordinated model already present in the section's prose
Visualize the comparison table contrasting per-site vendor model versus account-level coordinated model already present in the section's prose
See How Leading Healthcare Operators Are Scaling Patient Retention Initiatives System-Wide
Request data-backed benchmarks and actionable frameworks for improving patient retention across multi-location networks—built for marketing leaders managing complex site portfolios.
An operating model that holds patients inside the network
Integrating the four retention levers and three coordination layers requires a comprehensive operating model, not just a series of projects. This model must simultaneously protect relational continuity to drive outcomes 9, standardize experience variables to foster loyalty in private multi-site settings 11, and leverage the federal portability standards now available across payers 5. These are ongoing operational principles, not one-time initiatives.
The operating model comprises four core components:
- A panel-and-scheduling architecture that prioritizes assigning patients to their established clinician, only routing to the next available provider when the patient explicitly prefers speed over continuity.
- An account-level workflow for referrals and prior authorizations, measured by time-to-resolution and in-network capture rates, rather than per-site authorization throughput 5, 12.
- An experience measurement framework that consistently tracks AHRQ-defined operational inputs—such as phone answer time, appointment availability, communication completeness, and visit punctuality—across all sites, with variance reported to a single executive 2.
- An information layer integrated with patient-access APIs, ensuring records, claims, and encounter data follow the patient across locations without manual re-entry at intake 3, 4.
When these components are integrated, accountability shifts. Site administrators no longer manage retention as a local marketing expense but as a continuity and coordination outcome measured at the network level. The marketing function evolves from site-specific recall campaigns to ensuring network-wide message consistency, which is crucial for satisfaction-driven loyalty in private primary care 11. Clinical operations become responsible for panel design and referral capture decisions, which network leakage literature identifies as primary drivers of patient retention 12.
This model also makes failure modes transparent:
- Leakage from primary-to-specialist referrals will manifest in low in-network capture rates, not just NPS scores.
- Inconsistent access will appear as cross-site variance in appointment availability, not merely average satisfaction.
- Broken continuity will be evident in low clinician-match rates across visits, rather than marketing attribution.
Each lever provides its own diagnostic, making these issues visible at the same strategic level as the P&L.
Provider panels, scheduling, and the continuity-access tradeoff
The balance between continuity and access is primarily determined by panel management and scheduling practices. A default that routes patients to the next available provider across sites maximizes short-term access but erodes relational continuity, which is linked to fewer ED visits and hospitalizations 10. Conversely, prioritizing a patient's established clinician protects continuity but may delay care. The optimal operational approach is to present this tradeoff as a patient-visible choice during booking, with continuity as the default, supported by stable panel assignments and provider tenure 1.
Where Vectoron fits and what to do next
The operating model described requires execution capacity that scales with the network, not just the number of sites. This points to a solution that provides a single, account-level program to manage message consistency, referral and access workflow standards, and cross-site experience measurement as a continuous operation, rather than fragmented vendor engagements 2, 12. Per-site retainers and localized agencies often work against the variance-reduction goal that drives satisfaction-loyalty in private multi-site settings 11.
Vectoron is designed for this account-level execution layer, specifically for multi-location healthcare operators. For organizations with more than five locations, a practical next step is to audit current retention spending against the four levers and three coordination layers discussed in this article. This audit can identify areas where per-site coordination creates unnecessary variance. Teams interested in evaluating this model can begin with a two-week trial at $599/month.
Frequently Asked Questions
References
- 1.What is needed for continuity of care and how can we achieve it?.
- 2.What Is Patient Experience? | Agency for Healthcare Research and Quality.
- 3.Interoperability and Patient Access Fact Sheet - CMS.
- 4.Patient Access API - CMS.
- 5.Advancing Interoperability and Improving Prior Authorization Procedures Rule.
- 6.Continuity and care coordination of primary health care: a scoping review.
- 7.Redefining Primary Care for the 21st Century.
- 8.Section 2: Why Improve Patient Experience? - AHRQ.
- 9.The Wall of Evidence for Continuity of Care: How Many More Bricks Do We Need?.
- 10.Continuity of Care and Other Determinants of Patient Satisfaction with Primary Care.
- 11.Understanding patient satisfaction and loyalty in public and private primary health care.
- 12.On designing of a low leakage patient-centric provider network.