
Key Takeaways
- Patient acquisition now compounds across four forces—consumerism, public quality data, brand equity, and competitive market structure—each moving quarterly and each reinforced or surrendered by marketing decisions.
- Of the 21 documented factors shaping patient choice, marketing directly owns promotion and co-owns the presentation of services and price; facilities, physicians, and location are inherited operational outputs 4.
- Experience reliably drives retention through satisfaction, trust, and loyalty, but no empirical study has established a direct causal link between patient experience and new patient acquisition 10, 16.
- Per-location retainers scale linearly and fragment system narratives, while account-level execution templates strategy once and localizes across sites, shifting cost from location count to actual content units produced.
Patient Choice Now Behaves Like Consumer Choice
The patient who once selected a hospital based on a physician referral and a 10-minute drive now opens three browser tabs, scrolls Google reviews, checks insurance coverage, and compares wait times before placing a call. Patient-centered care and healthcare consumerism have become the two dominant frameworks shaping how Americans engage with providers, with online channels acting as the primary arena where those expectations get expressed 2. Decision authority has shifted toward the individual, supported by digital tools, accessible health data, and a growing tolerance for switching 8.
This change has operational consequences for any CMO who owns acquisition KPIs. Patients carry consumer reflexes into a context that healthcare systems historically organized around clinical workflows and referral networks. They expect search results that answer specific questions, transparent service information, and digital touchpoints that work on a phone at 9 p.m. When those signals are missing or inconsistent across locations, prospective patients route around the system entirely.
The argument that follows is not that hospitals should market more. It is that the acquisition function now sits on top of four compounding forces—consumerism, public quality data, brand equity, and competitive market structure—each of which moves quarterly and each of which marketing either reinforces or surrenders. Treating marketing as a campaign-by-campaign discretionary spend misreads the underlying behavior. Effective hospital marketing begins with a structured understanding of patient needs and expectations, not an ad calendar 9. The sections that follow examine each force, map which acquisition levers marketing actually controls, and address the harder question of how to run that system across many locations without doubling the budget every time a site is added.
The Four Forces Reshaping Hospital Acquisition
Consumerism: Patients Research, Compare, and Switch
Healthcare consumerism is no longer a future-state slide in a board deck. Decision authority has moved toward the individual patient, supported by digital tools, accessible health data, and generative AI interfaces that summarize provider reputations in seconds 8. Patients now expect personalization, transparency, and frictionless access—the same standards they apply to retail and banking—and they carry those expectations into every search query, intake form, and post-visit review 2.
The behavioral consequence is switching. A 2023 McKinsey analysis of more than 3,000 U.S. healthcare consumers found that satisfied consumers are 28 percent less likely to switch providers, a finding drawn from self-reported survey data about intent and recent provider changes rather than longitudinal claims records 17. The inverse carries the operational weight for CMOs: dissatisfied patients, or patients who never developed a relationship strong enough to feel satisfied, leave at materially higher rates. Every leakage event is also an acquisition event for a competitor in the same market.
Switching does not happen in a clinical vacuum. It happens after a patient compares two urgent care sites on Google Maps, reads three reviews of an orthopedic group, and notices that one health system's website answers her question about same-day MRI availability while the other does not. The consumer roles patients adopt online—information seeker, comparison shopper, reviewer—directly shape the funnel CMOs are responsible for filling 2. Treating that funnel as a brand-awareness budget understates what consumerism has already done to the underlying demand pattern. Acquisition now depends on whether the system shows up, with the right answer, at each of those comparison moments—across every location a patient might consider.
Public Quality Data as a Marketing Surface
HCAHPS changed what a hospital's reputation is made of. As the first national, standardized, publicly reported survey of patients' perspectives on hospital care, HCAHPS makes experience data visible to any consumer, payer, or referring physician with a browser 5. CMS continues to refine the survey's role in value-based purchasing, which means scores carry both reputational and financial weight at the same time 5. For a CMO, that publication cadence creates a permanent marketing surface the team did not choose to compete on but cannot ignore.
The competitive implications are not abstract. Research examining U.S. hospitals found that systems achieving higher HCAHPS scores than their local competitors are associated with greater market share, with the relationship strong enough to position experience as a documented differentiator rather than a soft attribute 6. The study uses observational data, so causality between any single score movement and share gain is not isolated 6. The directional signal still matters: relative experience scores correlate with relative share in the same geography.
The marketing function does not produce HCAHPS scores. Clinical operations, nursing leadership, environmental services, and discharge processes do. What marketing controls is how those scores get framed in service-line pages, physician profiles, location landing experiences, and patient-facing reputation channels. Public experience data either reinforces a system's narrative or contradicts it. When the gap between what the marketing site claims and what the publicly reported scores show is large, consumer trust erodes—particularly among the comparison-shopping behaviors documented in consumerism research 2. The acquisition implication is direct: experience data is now part of the funnel whether the system integrates it or not.
Brand Equity as a Measurable Strategic Asset
Brand equity in healthcare is often dismissed by CFOs as a line item that cannot be defended in a budget review. The literature suggests otherwise. A systematic review of consumer and patient determinants of hospital brand equity concluded that perceived service quality, hospital reputation, and patient experience function as the central drivers of brand equity, and that brand equity in turn shapes patient choice, loyalty, and price tolerance 3. The asset is not the logo. The asset is the accumulated set of perceptions that determines whether a prospective patient considers the system at all.
A complementary analysis of hospital branding describes it as a strategic imperative rather than a discretionary investment, linking favorable brand image to measurable outcomes including customer satisfaction, service quality perceptions, loyalty, and repurchasing intention 12. In competitive markets, a strong brand helps patients differentiate between providers who otherwise present similar clinical credentials, insurance acceptance, and geographic reach 12. That differentiation work happens before any single ad is served; it determines which systems make a patient's shortlist when a need emerges.
Two caveats matter for CMOs defending this spend. The brand equity literature notes inconsistent conceptualizations and measures across studies, which complicates direct ROI benchmarking against a single index 3. And branding investments must align with operational delivery—poorly aligned branding creates expectation gaps when operations cannot deliver on the promise 12. Neither caveat dissolves the asset argument. They sharpen it. Brand equity is measurable when paired with consistent satisfaction and reputation instruments, and it is defensible as a strategic asset because it materially affects which patients enter the funnel in the first place.
Competitive Market Structure and the Cost of Silence
Competition in healthcare markets is not just a policy concept. CMS frames it directly: in competitive markets, providers are more likely to offer a wider range of services at more affordable prices to attract patients, and competition supports value-based, patient-centered care models 7. The corollary is operational. When competitors expand service variety, refine pricing transparency, and invest in patient-centered design, a hospital that stays silent on those same dimensions surrenders consideration by default 14.
The cost of silence is not a missed campaign. It is a structural reduction in how often a system appears in the consideration set of patients who are actively comparing options. Patients exercising choice based on preferences, budget, and experience need information to make those comparisons 14. If a system does not produce that information at the service-line level, across every location, competitors fill the gap with their own narratives.
Competition-driven marketing carries a genuine tension that CMOs should not paper over. Research on hospital competition and strategic mission found that costs tend to increase in markets where hospitals compete heavily on quality and amenities, raising legitimate questions about system-wide efficiency 13. The finding does not argue against marketing. It argues against marketing disconnected from operational substance—promotion that drives demand for services the system cannot deliver consistently. The four forces compound here: consumerism creates the demand for comparison, public quality data supplies the evidence, brand equity determines which systems make the shortlist, and competitive market structure punishes the systems that opt out of the conversation.
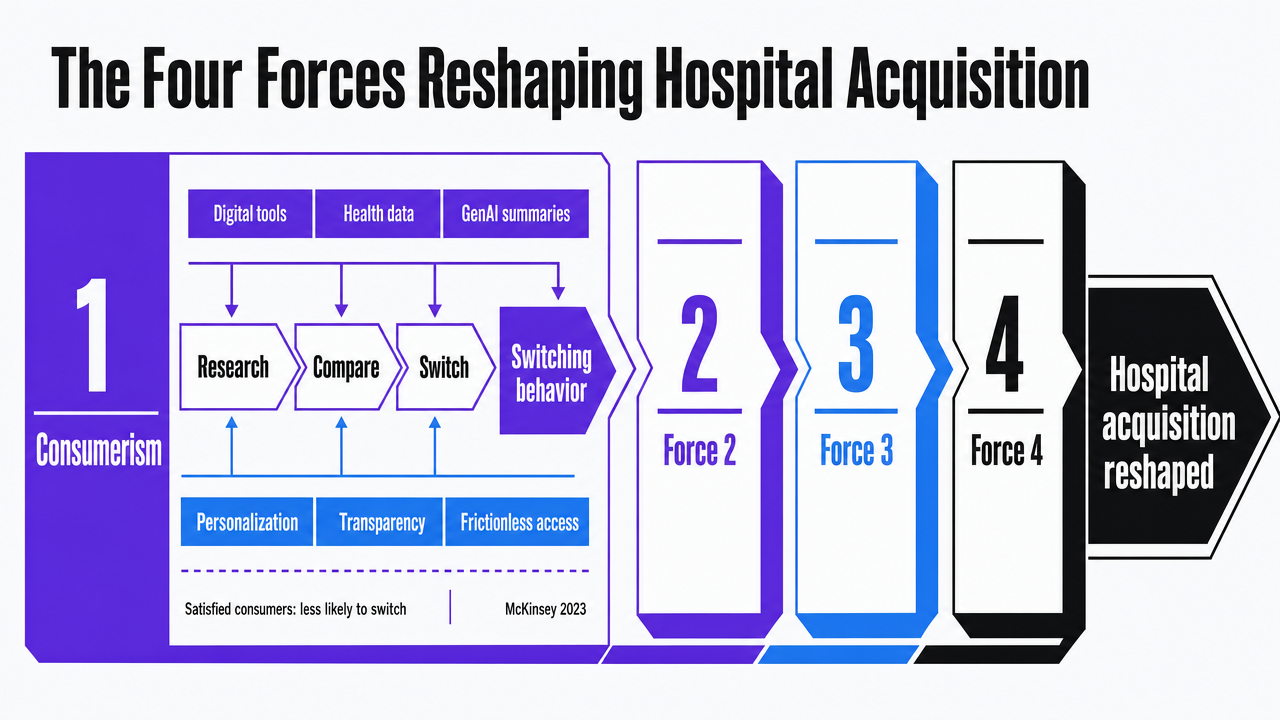 Visualize the four compounding forces framework that structures the entire section, giving readers a memorable mental model before diving into each force
Visualize the four compounding forces framework that structures the entire section, giving readers a memorable mental model before diving into each force
Mapping Acquisition Levers to What Marketing Actually Controls
An empirical study of patient choice identified 21 distinct factors that shape which hospital or clinic a patient selects, grouped into six categories: facilities and physical assets, physicians and employees, location, services, price, and promotion 4. The categorization matters more than the count. It defines a defensible answer to the question every CFO eventually asks: which of these levers does marketing actually own?
Three categories sit largely outside the marketing function. Facilities and physical assets are capital decisions. Physicians and employees are recruiting, credentialing, and culture outputs. Location is real estate strategy set years before a campaign launches. Marketing can describe these attributes, but it does not produce them. Treating them as marketing deliverables creates the expectation gap that the branding literature warns against 12.
Three categories are either fully marketing-controllable or co-owned with operations. Promotion is the cleanest case: channel selection, messaging, search visibility, reputation management, and creative production are all direct marketing outputs. Services and price are co-owned. Marketing controls how service-line breadth, scheduling access, and price transparency get presented across digital touchpoints, while operations and finance set what is actually offered. The marketing function's job is to make the operationally true version of each category legible to a comparison-shopping consumer at the moment of decision 2.
This split has budget implications that hold up in a CFO review. Marketing investment in the promotion category produces direct, attributable outputs. Investment in the service and price categories produces presentation infrastructure—landing pages, location experiences, scheduling integrations—that converts inherited operational assets into visible acquisition levers. Investment that tries to compensate for weaknesses in facilities, staff, or location through louder promotion produces the cost-without-substance problem that competitive markets eventually expose 13. The framework gives CMOs a way to defend sustained spend on the categories marketing actually controls, while pushing back on requests to use marketing as a fix for operational deficits the function cannot solve 9.
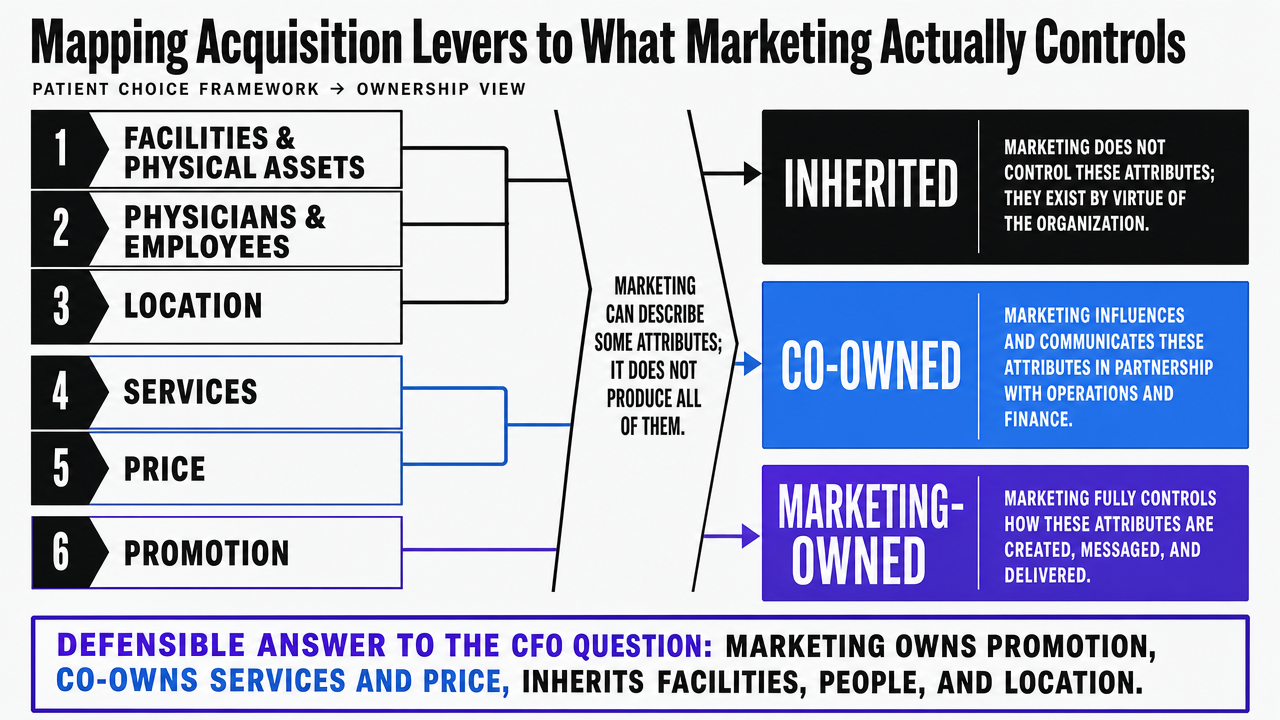 Translate the cited 21-factor, six-category patient choice framework into a defensible visual that shows which categories marketing owns, co-owns, or inherits — directly supporting the section's CFO-defense argument
Translate the cited 21-factor, six-category patient choice framework into a defensible visual that shows which categories marketing owns, co-owns, or inherits — directly supporting the section's CFO-defense argument
Test scalable patient acquisition workflows risk-free
Experience real-time, multi-location marketing execution and publish live campaigns during your free trial.
The Honest Gap: Experience Drives Loyalty, but Acquisition Measurement Lags
Patient experience research has a credibility problem that CMOs should name before a CFO does. A review of empirical studies on the business case for patient experience found no studies establishing a direct relationship between patient experience and the intermediate business outcome of new patient acquisition, despite a strong conceptual link to loyalty, market share, and malpractice risk 10. The evidence base supports experience as a retention and reputation lever. It does not yet prove experience causally produces new patients at a measurable rate.
That gap matters because the rest of the literature is consistent on what experience does drive. Patient satisfaction has a significant positive effect on patient trust and loyalty, with trust partially mediating the path from satisfaction to repeat behavior 16. Functional, emotional, and relational dimensions of experience independently raise intention to reuse services, with communication and empathy as particularly strong predictors of loyalty 11. The mechanism for keeping patients is documented. The mechanism for attracting strangers based on the experience of patients they have never met is inferred, not measured.
For CMOs, the honest framing is more defensible than the overreach. Marketing investment in experience-aligned narratives, reputation channels, and post-visit advocacy operates on two timelines: a measurable loyalty effect that protects existing patient revenue, and a directional reputation effect that likely supports acquisition through public scores 5and brand equity 3without a clean attribution path. Boards accept asymmetric evidence when it is presented as such. They reject it when marketing claims certainty the research does not support.
Digital Channels: Where Acquisition Compounds or Erodes
Digital marketing in hospital settings produces a documented set of acquisition benefits: attracting new patients, expanding business, increasing patient trust, strengthening loyalty, raising brand awareness, and prompting word-of-mouth referrals across patients' families and networks 15. The list reads like a CMO scorecard because that is functionally what it is. Each item corresponds to a measurable upstream signal—organic search traffic, branded query volume, review velocity, direct site visits—that converts into downstream appointment requests when the underlying infrastructure works.
The compounding mechanic is what makes digital different from a paid campaign cycle. Search visibility for a specific service line at a specific location accumulates over months and then produces traffic indefinitely. Reputation channels accrue review volume that influences every subsequent comparison shopper 2. Branded content earns repeat visits that lower the cost of every future acquisition in that geography. None of this works without consistent execution at the service-line and location level, which is where most hospital digital programs fracture.
The erosion side is equally specific. Digital channels also carry documented risks: misinformation in health content, privacy exposure in tracking implementations, and regulatory compliance failures in advertising claims 15. A single non-compliant landing page, a stale physician profile, or a service page that contradicts publicly reported quality scores does not just fail to acquire—it actively reduces trust among the consumers who found it. Digital acquisition compounds in both directions, and the systems that treat it as a quarterly campaign exercise rather than a continuous operation tend to discover the erosion side first.
See How Leading Hospitals Scale Patient Acquisition Without Agency Overhead
Get a personalized walkthrough of AI-driven marketing infrastructure proven to coordinate multi-site campaigns, streamline content operations, and deliver measurable patient growth—without adding internal headcount.
If You Manage Multiple Locations: Coordination Economics
Why Per-Location Retainers Scale Linearly
This section addresses CMOs running 10 or more sites. Single-facility leaders can skip ahead; the economics that follow only bind once a system carries enough locations for delivery overhead to dominate.
Traditional agency engagements price the work by site. A regional system with 20 ambulatory locations typically carries 20 retainers, each with its own account manager, intake call, monthly reporting deck, and creative review cycle. The unit cost looks reasonable in isolation. The aggregate cost scales linearly: every new urgent care, primary care expansion, or specialty acquisition adds another full retainer to the budget, plus the coordination tax of keeping that retainer aligned with the system's broader narrative.
The linearity problem is not just financial. Effective hospital marketing depends on a structured, system-wide understanding of patient needs and expectations, applied consistently across touchpoints 9. Per-location retainers fragment that understanding by design. Each agency team builds its own playbook for its assigned site, optimizes against site-level KPIs, and produces creative that drifts from sibling locations within two or three quarters. The CMO inherits a portfolio of microbrands instead of a coherent system.
The downstream cost shows up in three places. Service-line messaging contradicts itself across sites in the same metro. HCAHPS-aligned narratives get rebuilt 20 times instead of templated once. And every strategic pivot—a new service-line launch, a payer contract change, a competitor entry—requires 20 separate change orders before the system actually moves.
Account-Level Execution Across Sites and Service Lines
Account-level execution inverts the unit. Strategy, content production, SEO, and reputation work run against the system as a single account, with location-specific outputs generated from a shared operating plan rather than rebuilt from scratch at each site. The cost driver shifts from number of locations to number of distinct service lines and content units actually published, which scales sub-linearly as the system grows.
The model fits the underlying acquisition logic. Marketing's job is to make the operationally true version of each service legible to comparison-shopping consumers at the moment of decision, applied consistently across every site a patient might consider 9. That work is largely the same template applied 20 times with location-specific evidence, not 20 separate creative exercises.
The variables that drive cost in each model differ in kind, not just magnitude:
| Variable | Per-Location Retainer | Account-Level Execution |
|---|---|---|
| Locations (20) | 20 retainers | 1 account plan |
| Service lines (6) | Rebuilt per site | Templated once, localized |
| Content units per location/month | Linear with sites | Sub-linear; shared production |
| Strategy pivots | 20 change orders | 1 plan update |
| Cost scaling | Linear with locations | Sub-linear with locations |
The table is structural, not financial. Actual spend depends on service-line count, content velocity, and competitive intensity in each geography. The point is the slope: under retainer economics, adding the 21st location costs roughly the same as the 20th. Under account-level economics, the 21st location adds localization work against a plan that already exists, and the marginal cost falls.
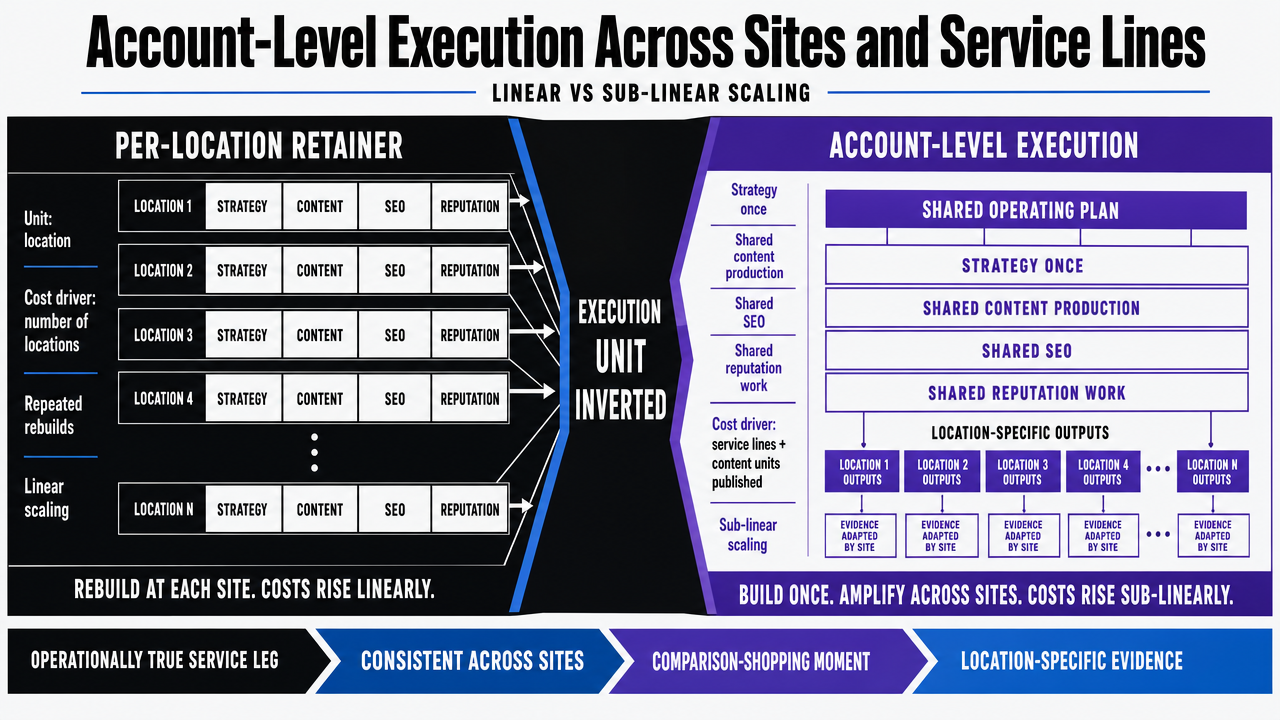 Convert the section's comparison table into a sharper visual contrast between per-location retainer economics and account-level execution, reinforcing the linear vs sub-linear scaling argument
Convert the section's comparison table into a sharper visual contrast between per-location retainer economics and account-level execution, reinforcing the linear vs sub-linear scaling argument
What a Continuous Acquisition System Requires
The four forces do not move on a campaign calendar. Consumerism reshapes search behavior week by week. HCAHPS scores publish on a fixed cadence and reset competitive narratives in every metro 5. Brand equity accumulates or erodes through reputation channels that never pause 3. Competitors launch service-line pages, refine pricing transparency, and capture comparison-shopping intent without warning 7. An acquisition function organized around quarterly creative sprints and annual planning cycles operates one timeline behind the market it serves.
A continuous system has three structural requirements. First, strategy that updates against live data—search visibility, branded query trends, review velocity, competitor service-line moves—rather than the planning artifact agreed to last fiscal year. Marketing built on a structured understanding of patient needs only stays accurate when that understanding gets refreshed against current behavior 9. Second, production capacity that can localize service-line content across every site without rebuilding the strategy each time. The framework of marketing-controllable levers—promotion, and the presentation layer for services and price—has to be executed at every location a comparison-shopper might reach 4. Third, governance that catches the erosion side of digital before it compounds: stale physician profiles, compliance drift, contradictions between site claims and public quality scores 15.
This is the cadence problem retainer models were not built for. The closing question is no longer whether hospitals need marketing. It is whether the delivery model behind that marketing can keep pace with patients who already have.
Frequently Asked Questions
References
- 1.Patient Satisfaction with Healthcare Services and the Techniques Used for Its Assessment: A Systematic Review.
- 2.Patient-Centered Care and Healthcare Consumerism in Online Patient–Provider Communication: A Systematic Review of Theoretical Perspectives.
- 3.Consumer or Patient Determinants of Hospital Brand Equity: A Systematic Literature Review.
- 4.Factors Contributing Towards Patient's Choice of a Hospital Clinic from the Patients' and Managers' Perspective.
- 5.HCAHPS: Patients' Perspectives of Care Survey.
- 6.The Relationships between Patient Satisfaction, Market Share, and Profitability: An Examination of U.S. Hospitals.
- 7.Competitive Health Care Markets.
- 8.Executive power shift: Embracing elevated consumerism in health care.
- 9.The impact of marketing strategies in healthcare systems.
- 10.Examining the Business Case for Patient Experience.
- 11.The Impact of Patient Experience on Loyalty in the Context of Medical-Aesthetic Health Services.
- 12.A Strategic Imperative for Promoting Hospital Branding.
- 13.Health Care Competition, Strategic Mission, and Patient Satisfaction.
- 14.Competitive Health Care Markets.
- 15.The impact and challenges of digital marketing in the health care industry.
- 16.The Impact of Patient Satisfaction on Patient Loyalty with the Mediation of Patient Trust.
- 17.Marketing in healthcare: Improving the consumer experience.