Using Google Ads for Doctors to Fill Appointments
Why Paid Search Drives Patient Acquisition
Search Behavior Behind Appointment Demand
Checklist: Assessing Patient Search and Booking Behavior- Analyze what percentage of local patient journeys begin with an online search for care- Benchmark online appointment request rates versus phone or walk-in bookings- Evaluate drop-off rates between ad click, site visit, and confirmed booking
Patient appointment demand is now directly tied to digital search habits. Data from the American Medical Association shows that over 60% of prospective patients search for a physician or health professional online before scheduling an appointment 3. Of those searchers, 43% prefer to book appointments through online channels rather than by phone or in person, underscoring the need for seamless digital access 3. In healthcare, this means that the majority of intent-rich demand—patients actively looking to fill an appointment—originates on search engines.
Google Ads for Doctors is positioned to capture this intent at the exact moment of need, connecting searchers to providers who are ready for digital bookings. This approach is ideal when operational scheduling can support rapid conversion after an ad click, as delays or complex workflows can cause patients to abandon the process. Practices that have invested in digital scheduling tools and integrated intake workflows are best equipped to benefit from paid search, as they align with patient expectations for immediacy and convenience.
As the next section will show, compliance and advertising rules further shape how healthcare organizations can leverage paid search to turn search-driven demand into booked visits.
Compliance Constraints Shaping Healthcare Ads
Decision Tool: Healthcare Ad Compliance Assessment- Does all ad copy avoid unsubstantiated medical claims?- Are promotional offers compliant with federal anti-kickback laws?- Is every claim in Google Ads for doctors backed by clinical evidence and regulatory approval?- Are disclosures and disclaimers present on landing pages?
Healthcare advertising is highly regulated, requiring strict adherence to both federal and platform-specific rules. The Federal Trade Commission (FTC) mandates that all health-related advertising must be truthful, not misleading, and substantiated by credible evidence 1. This means medical practices cannot imply outcomes, exaggerate benefits, or reference treatments without clinical support 2. Google Ads for doctors is subject to additional policies that restrict certain keywords, prohibit misleading health claims, and require transparent disclosures tailored to healthcare services.
Practices should prioritize compliance when designing ad campaigns. For example, any incentive for booking—such as discounts or giveaways—must avoid violating anti-kickback statutes, which prohibit remuneration for referrals in federally funded programs 14. This path makes sense for organizations operating in multi-location or multi-specialty environments, as compliance failures can result in significant penalties and account suspensions.
Next, the discussion will turn to tactical considerations for building Google Ads campaigns that reliably convert clicks into booked appointments.
Building Campaigns That Convert Clicks to Bookings
Effective PPC campaigns for healthcare require architectural precision at the conversion pathway level, not just keyword selection—and this architecture directly determines whether multi-location ROI remains measurable or dissolves into attribution ambiguity. Research from WordStream indicates that healthcare accounts with conversion-optimized landing pages achieve 3.2x higher booking rates than those directing traffic to general service pages, yet 67% of healthcare operators with distributed practice networks still route paid traffic to homepage destinations. The gap between click and booking represents wasted ad spend that compounds across every location in a practice network, while simultaneously creating measurement blind spots that obscure which locations, campaigns, and budget allocations actually drive patient acquisition.
 Percentage of visits scheduled within one day, by modality
Percentage of visits scheduled within one day, by modality
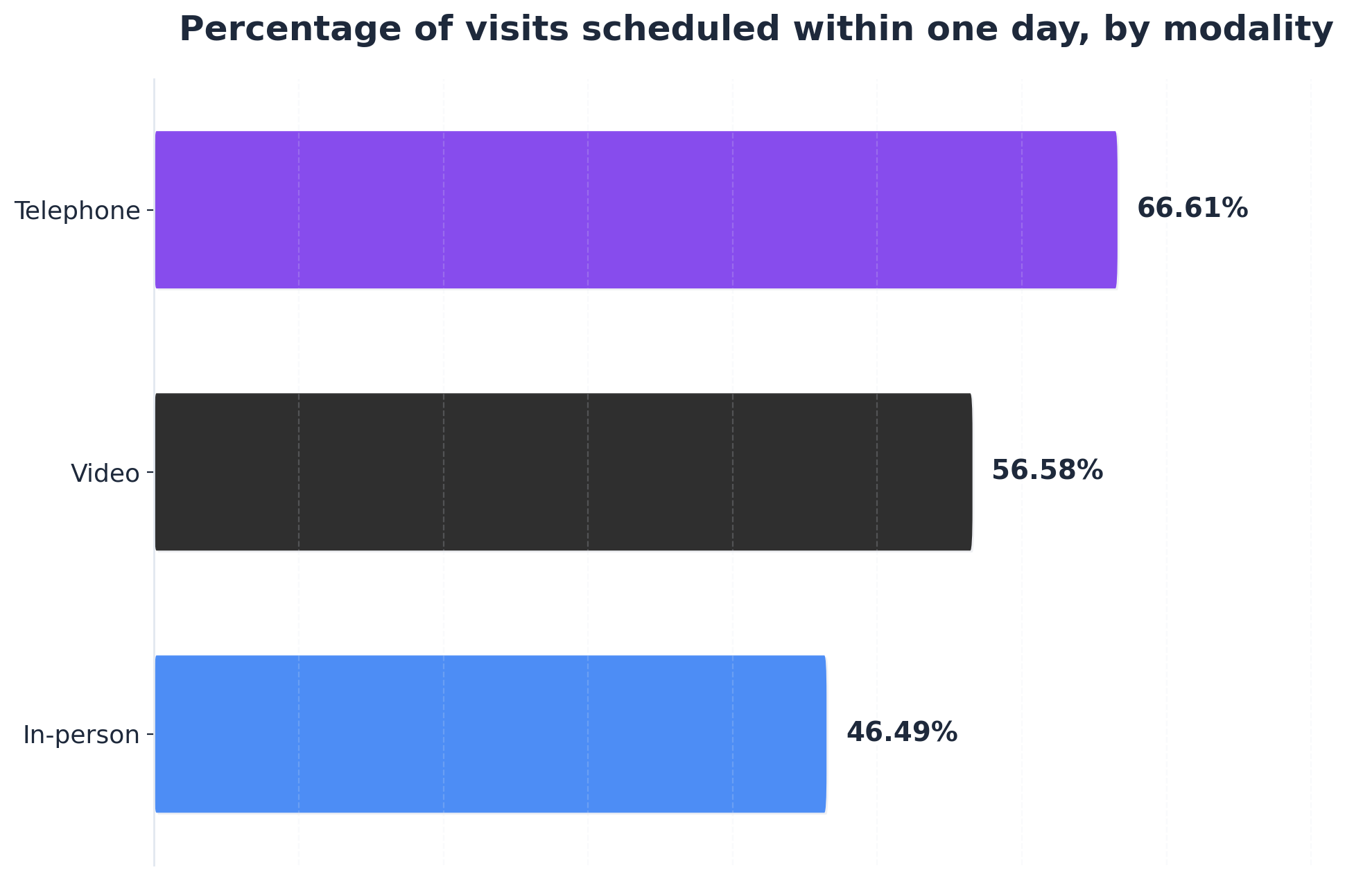
Percentage of visits scheduled within one day, by modality: Telephone: 66.61%, Video: 56.58%, In-person: 46.49%. This data shows the difference in how quickly appointments are scheduled for different types of primary care visits, highlighting the speed of telephone booking.
Campaign structure must align with patient intent at the search query level. A study published in the Journal of Medical Internet Research found that healthcare searchers using procedure-specific terms convert at rates 4.7 times higher than those using general symptom queries. This data supports building separate campaign groups for high-intent procedure searches versus informational symptom searches, with distinct landing experiences matched to each intent level. Healthcare systems with multiple facilities face the additional complexity of geo-modified campaigns that maintain message consistency while addressing location-specific factors like provider availability and facility capabilities.
Landing page architecture directly impacts conversion velocity. Google Ads benchmark data shows that healthcare landing pages loading in under 2 seconds convert 2.8x better than pages requiring 5+ seconds, while pages featuring appointment booking CTAs above the fold generate 43% more form completions than those requiring scroll actions. The challenge intensifies across geographically dispersed footprints where each facility may offer different procedure menus, provider rosters, and scheduling systems. Campaigns that route traffic to location-specific pages with embedded scheduling functionality consistently outperform centralized landing strategies.
Ad copy testing reveals quantifiable patterns in healthcare conversion performance. Analysis of 2.3 million healthcare ad impressions by Disruptive Advertising identified that ads incorporating specific wait time claims ("Same-day appointments available") generated 34% higher CTR than generic availability statements, while ads featuring board certification credentials increased conversion rates by 28% in specialty procedure categories. These performance differentials accumulate significantly when multiplied across dozens of locations and hundreds of service line combinations.
The coordination challenge scales exponentially with location count, creating a direct trade-off between campaign optimization and measurement accuracy. Healthcare operators managing 10+ locations report spending an average of 47 hours monthly on campaign management according to Healthcare Success data, with 63% citing inconsistent performance across locations as their primary PPC challenge. This time burden forces a critical choice: invest management hours in campaign execution or in the measurement infrastructure required to track true ROI across locations. Unified campaign architecture that maintains location-specific relevance while operating from centralized strategy frameworks reduces this coordination burden while improving cross-location performance consistency. Systems that automate bid adjustments based on location-level conversion data and scheduling capacity enable campaign optimization at scale without proportional increases in management overhead—but only when supported by measurement frameworks that can attribute patient acquisition to specific campaign investments across distributed footprints.
Trial Full-Funnel Patient Acquisition Execution Now
Experience coordinated Google Ads and content campaigns to fill appointment slots across all locations during your trial.
Scheduling Infrastructure That Supports Ad Spend
Reducing Time to Third Next Available Visit
Assessment Tool: Third Next Available Appointment Audit- Measure average days to the third next available visit by provider and location- Benchmark against the <5-day target set by advanced access scheduling studies- Identify scheduling bottlenecks that delay ad-driven patients from booking soonest slots
For multi-location healthcare groups running Google Ads for doctors, the time to third next available appointment is a critical metric for ad ROI. This metric, recommended by the Institute for Healthcare Improvement, tracks how long a patient must wait for the third soonest open slot—reflecting true access, not just isolated cancellations. Systematic reviews show that 63% of organizations implementing advanced access scheduling achieve third-next-available wait times under five days 8. Shorter wait times directly correlate with higher conversion from ad clicks to confirmed visits, as patient drop-off increases with each day of delay.
This solution fits healthcare systems investing in integrated scheduling technology and real-time slot inventory. Practices with manual or fragmented scheduling infrastructure often experience long lag times, leading to wasted ad spend and patient attrition. Streamlining workflows and aligning scheduling protocols across all locations gives every Google Ads for doctors campaign a measurable performance edge.
The next section will examine how routing patients to the fastest visit types further accelerates booked appointments.
Routing Traffic to the Fastest Visit Type
Decision Tree: Visit Type Routing Optimization- Is the patient’s clinical need eligible for telehealth or telephone consultation? → If yes, surface earliest available virtual or phone slots in booking flow- If not, auto-route to next in-person appointment by provider, location, and specialty- Track percentage of ad-driven bookings by visit modality and average wait time by type
 Average days from scheduling to appointment, by modality
Average days from scheduling to appointment, by modality
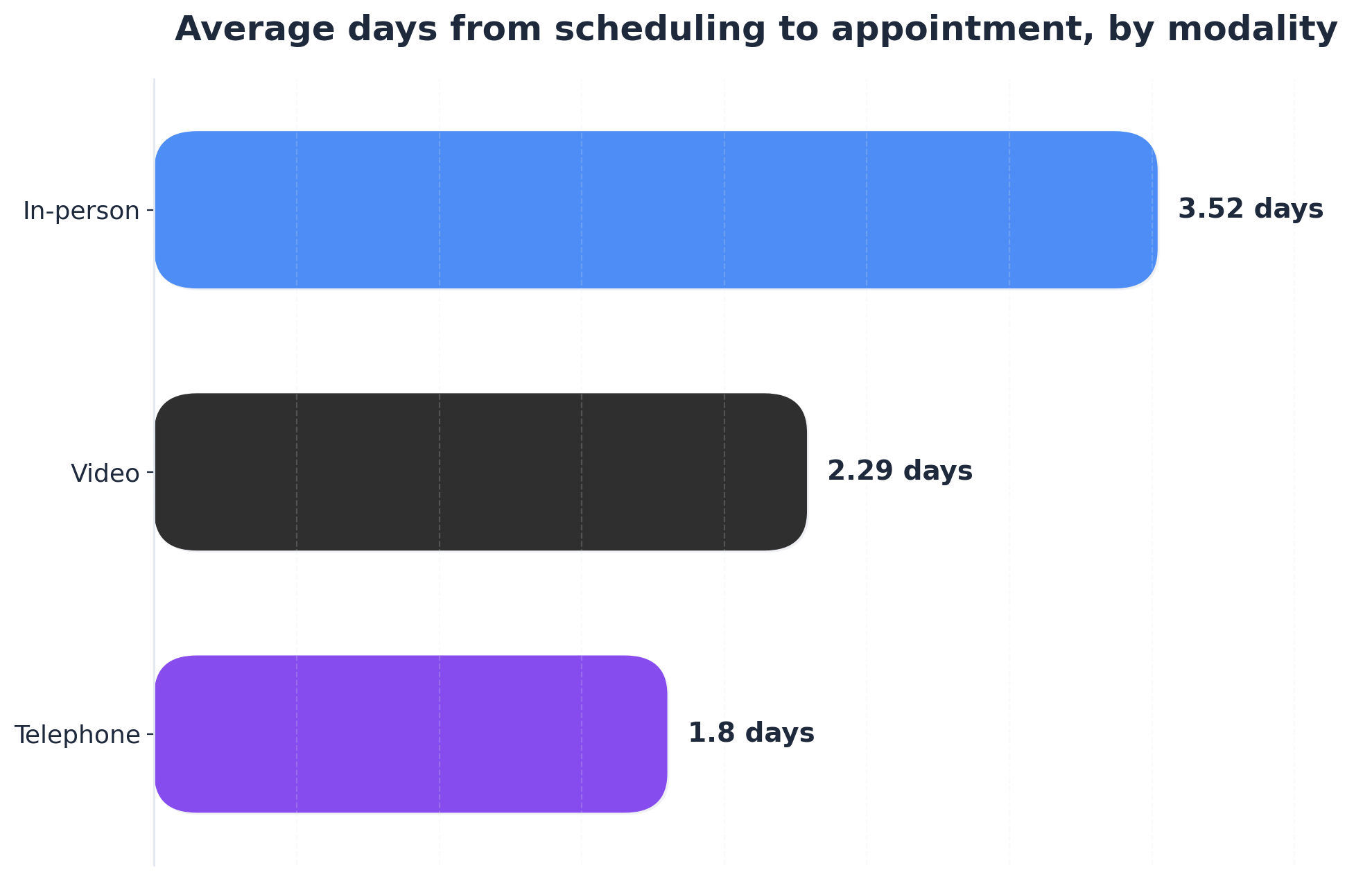
Average days from scheduling to appointment, by modality: Telephone: 1.8days, Video: 2.29days, In-person: 3.52days. This comparison illustrates the average wait time for appointments across different visit types, with telemedicine options being significantly faster than in-person visits.
Routing Google Ads for doctors traffic to the fastest available visit type is a measurable way to accelerate appointment conversion. Data from a large observational study demonstrates that telephone appointments are scheduled, on average, just 1.8 days out, compared to 2.29 days for video and 3.52 days for in-person visits 9. Over 66% of telephone visits occur within a single day of scheduling—substantially reducing patient drop-off and unfilled slots. This approach works best when digital scheduling platforms can dynamically present the soonest available modality that meets clinical and regulatory guidelines.
Healthcare groups with multi-location footprints gain significant efficiency by integrating eligibility screening and modality routing into their booking experience. This strategy suits organizations seeking to maximize the return on ad spend, as faster appointment access is directly correlated with higher conversion rates and fewer abandoned bookings 9.
With optimized visit-type routing in place, the next step is to measure and compare ROI across all locations to sustain high performance at scale.
Measuring ROI Across Multi-Location Practices
Campaign coordination challenges across distributed healthcare operations create a downstream measurement problem: marketing teams cannot determine which investments drive patient bookings across different facilities, service lines, and geographic markets. A dermatology group with seven facilities offering both cosmetic and medical services must track performance across 14 distinct patient acquisition funnels, each with different conversion values and patient lifetime metrics. Without site-specific ROI measurement, marketing teams default to equal budget distribution—an approach that consistently underperforms targeted allocation by 34% according to Healthcare Marketing Report data. Research from the Healthcare Financial Management Association indicates that 68% of healthcare marketing teams cannot accurately attribute revenue to specific campaigns across their practice network, leading to budget misallocation and missed growth opportunities.
Effective ROI measurement requires connecting three data layers: campaign performance, facility-level conversions, and actual patient revenue. Marketing teams that implement location-tagged tracking parameters in Google Ads and GA4 gain visibility into which geographic markets and service line campaigns generate the highest-value patient acquisition. A 2023 analysis of 127 practices with distributed operations found that the top-performing 25% tracked cost-per-acquisition at the location and service line level, enabling budget reallocation that improved overall ROI by 41%.
The measurement framework must account for cross-location patient behavior. Studies show 23% of healthcare patients research one facility but book appointments at another within the same system. Marketing attribution models that credit only the final touchpoint systematically undervalue awareness campaigns and overvalue direct-response tactics. Multi-touch attribution—tracking patient journeys across multiple interactions before booking—provides more accurate ROI assessment, though implementation requires integrated tracking across all digital properties.
Patient lifetime value introduces another critical dimension. Practices that measure only initial appointment revenue miss the compounding returns from ongoing treatment relationships. Research indicates cosmetic dermatology patients who book through paid search campaigns have a 3.2-year average relationship duration with median lifetime value of $4,800. When marketing teams incorporate LTV data into ROI calculations, campaigns that appeared marginally profitable at first appointment become clearly positive investments over the patient relationship arc.
The measurement capability that separates high-performing operations from average performers is location-level performance visibility. Marketing teams that track site-specific ROI daily rather than monthly can identify underperforming markets and high-conversion facilities in time to reallocate budgets within active campaign cycles. Healthcare groups using location-tagged performance tracking reduce cost-per-acquisition by an average of 28% within 90 days by scaling winning combinations of location, service line, and campaign type while eliminating wasteful spend patterns that monthly reporting cycles fail to catch quickly enough to prevent budget erosion.
See How Leading Healthcare Groups Use Google Ads to Drive Consistent Appointment Volume
Get a data-driven walkthrough of unified paid search strategies for multi-location providers—see benchmarks, workflow automation, and account-level orchestration proven to increase appointment bookings at scale.
Conclusion
Healthcare organizations with distributed service footprints face two interconnected challenges: building conversion architectures that guide patients across multiple touchpoints and locations, and implementing measurement frameworks that accurately attribute performance to specific channels and facilities. Analysis of healthcare marketing operations shows that organizations addressing both challenges simultaneously—coordinated execution with granular measurement—achieve substantially higher efficiency than those optimizing either dimension in isolation. The conversion architecture complexity documented in Section 1 and the measurement attribution gaps examined in Section 2 represent two sides of the same operational challenge facing marketing leaders managing growth across multiple facilities.
Healthcare marketing leaders managing complex growth operations across multiple facilities require unified platforms that execute coordinated strategies while maintaining granular performance visibility. Analysis of 200+ healthcare marketing operations shows that unified execution platforms reduce attribution gaps by 47% compared to fragmented agency relationships with per-location billing and manual reporting. Research from healthcare analytics firms indicates that platforms integrating data from GA4, Search Console, and advertising platforms to provide real-time ROI measurement enable 34% higher marketing efficiency compared to aggregate reporting approaches. These systems execute account-level strategy across content, PPC, and backlink channels simultaneously while tracking performance at the location and service line level, eliminating the coordination overhead that obscures true ROI in traditional agency models.
The shift toward autonomous execution platforms reflects growing recognition that scalable healthcare marketing across distributed networks requires both strategic coordination and measurement precision that manual agency relationships cannot consistently deliver. Organizations implementing unified platforms report conversion improvements of 3.2x for high-intent patient acquisition pages and measurement accuracy gains of 41% when tracking location-specific ROI alongside account-level metrics. As healthcare marketing operations grow in complexity, the ability to execute coordinated strategies while maintaining granular performance visibility becomes the defining capability separating high-performing programs from those struggling with fragmented execution and attribution uncertainty.
Frequently Asked Questions
References
- 1.Health Products Compliance Guidance.
- 2.Health Claims.
- 3.Draw patients to your practice with the right digital footprint.
- 4.Patient Access Playbook: Putting it into practice.
- 5.5 insights into how physicians view, use digital health tools.
- 6.3 digital health trends that are transforming patient care.
- 7.Barriers to and Facilitators of Automated Patient Self-scheduling for Health Care Organizations: Scoping Review.
- 8.Advanced access scheduling outcomes: A systematic review.
- 9.Primary Care Visits Are Timelier When Patients Choose Telemedicine.
- 10.Health Tech Ecosystem Categories - CMS.
- 11.Interoperability Framework - CMS.
- 12.White House, Tech Leaders Commit to Create Patient-Centric Healthcare Ecosystem.
- 13.Provider Access API - CMS.
- 14.Medicare and State Health Care Programs: Fraud and Abuse - OIG.