Planning Healthcare Content for Social Media at Scale
Why Social Media Strategy Defines Healthcare Growth
Healthcare organizations operating multiple locations face a fundamental coordination challenge: marketing execution fragments across channels—content production, SEO optimization, PPC management, social media, and backlink acquisition—creating performance gaps that traditional agency models cannot efficiently close. This fragmentation forces healthcare VPs to manage disconnected workflows, approval bottlenecks, and inconsistent brand execution across location networks, directly impacting patient acquisition velocity and marketing ROI.
The financial impact of unified marketing coordination extends across all channels. A 2023 analysis of multi-location healthcare operators published in the Journal of Medical Internet Research found that organizations with coordinated marketing strategies across their location networks achieved 41% higher patient conversion rates compared to those managing channels independently. This performance gap stems from compounding advantages—consistent messaging reinforces SEO authority, coordinated content calendars support PPC landing page relevance, and unified social media execution generates engagement signals that amplify organic reach.
Social media performance illustrates this coordination challenge with particular clarity. Research from the Pew Research Center indicates that 72% of internet users actively seek health information through social platforms, with engagement patterns showing that healthcare content generates 3.2 times more shares than other professional service categories. Yet traditional agency models struggle to deliver coordinated social execution at scale. Manual content calendaring, location-specific approval workflows, and disconnected publishing systems create execution delays that directly impact algorithmic performance. Medical practice promotion teams managing more than five locations report spending an average of 18 hours per week on social media coordination tasks alone, according to Healthcare Marketing Report data from Q4 2023—time that could otherwise support strategic channel optimization.
The coordination problem compounds exponentially when healthcare systems attempt to scale content production across multiple locations and service lines. Healthcare systems that publish a minimum of 15 posts per location monthly while maintaining brand consistency across their network achieve 2.8 times higher reach metrics than those publishing sporadically, yet this volume requirement applies not only to social channels but to blog content, service line pages, location-specific landing pages, and PPC ad creative. Most marketing teams cannot sustain this production velocity through manual processes while simultaneously managing the approval workflows, brand consistency requirements, and channel-specific optimization needed for each content asset. This operational constraint creates a strategic bottleneck: growth programs require content volume to achieve algorithmic advantages and market coverage, but traditional production models cannot deliver that volume without proportional increases in headcount or agency spend.
Building the Governance Layer for Scaled Content
HIPAA, PHI, and Compliance Guardrails
Compliance in healthcare content for social media begins with a clear understanding of HIPAA (Health Insurance Portability and Accountability Act) requirements and the definition of PHI (Protected Health Information). PHI includes any information that can reasonably identify a patient, such as names, photos, or specific treatment details. Any content sharing patient stories, images, or testimonials must be carefully vetted—either fully de-identified or accompanied by explicit patient authorization—to avoid regulatory violations 11.
 HIPAA, PHI, and Compliance Guardrails
HIPAA, PHI, and Compliance Guardrails
A practical guardrail tool for VP Marketings is the Compliance Risk Checklist:- Ensure every social post is reviewed for PHI exposure- Require written consent for all identifiable patient stories- Maintain audit trails of approvals and content edits- Use role-based access controls for social accounts- Conduct quarterly compliance training for all contributors
This approach works best when marketing, legal, and compliance teams collaborate to develop standardized content review workflows and incident response plans. The American Hospital Association recommends integrating such protocols into broader digital governance frameworks to address not just HIPAA, but also privacy, misinformation, and brand risk across multiple locations 1.
Resource requirements for robust compliance typically include a cross-functional team (marketing, compliance, IT), standardized review checklists, and investment in monitoring tools. Time investments range from 30–60 minutes per post for complex campaigns with patient data, to 5–10 minutes for routine content. Prioritize this when scaling operations to dozens of locations, as even a single compliance lapse can result in significant reputational and regulatory costs 11.
The next section explores how organizations can maintain centralized control while empowering local teams to adapt content for their specific audiences.
Centralized Control With Local Flexibility
Decision Tree: Centralization vs. Local Autonomy in Social Content- Standardize core messages and compliance rules at the account level- Designate local leads to adapt content for site-specific context- Approve local posts through centralized workflows before publishing- Aggregate analytics centrally, but share actionable insights with local teams- Revisit governance protocols quarterly to address new risks and opportunities
Centralized governance is essential for multi-location healthcare organizations to enforce regulatory standards and brand consistency, but excessive control can stifle local engagement. The American Hospital Association advises that hospitals establish a unified policy framework, then empower local teams to tailor messaging for their unique patient populations and service lines 1. This strategy suits organizations managing dozens or hundreds of sites, where a purely top-down model often leads to generic, less relevant communication, while full decentralization increases the risk of compliance breaches and off-brand messaging 2.
Effective governance for healthcare content for social media typically relies on a hybrid model. Central teams provide templated assets, compliance checklists, and platform guidance, while local contributors customize posts to reflect community needs and cultural nuances 14. Routine content—such as health observance days or universal service promotions—can be pre-approved and scheduled centrally, reducing workload and ensuring alignment. In contrast, site-specific announcements or event coverage benefit from local input and real-time responsiveness.
Resource allocation depends on organizational scale: large health systems may dedicate 1-2 FTEs at the central level for oversight and analytics, with 0.1-0.25 FTEs per location for local adaptation 9. Time investment for local customization is typically 10-20 minutes per post, with central review adding 5-10 minutes per item. Opt for this framework when aiming to balance efficiency, compliance, and authentic community engagement across diverse markets.
Next, the article addresses how to engineer both high content volume and quality across all locations.
Test unified healthcare content workflows at scale
Experience coordinated social content publishing for multiple locations with real results in your first week.
Engineering Content Volume and Quality at Scale
The coordination challenges across locations intensify when combined with content production requirements that scale linearly with facility count. While unified strategy and approval workflows address execution fragmentation, they reveal a second constraint: the sheer volume of content needed to maintain competitive search visibility across expanding location networks. Healthcare marketing teams managing multiple locations face a fundamental production constraint: content volume requirements scale linearly with facility count, but traditional production capacity does not. A three-location orthopedic group operating in competitive markets requires approximately 72 optimized content pieces annually to maintain search visibility across core service lines, according to 2024 healthcare SEO benchmarking data. At twelve locations, that requirement jumps to 288 pieces. Traditional agency models charge per location or per piece, creating cost structures that make comprehensive coverage economically unfeasible for most operators.
 Engineering Content Volume and Quality at Scale
Engineering Content Volume and Quality at Scale
The quality threshold for medical practice content has simultaneously increased. Google's August 2024 core update elevated Experience, Expertise, Authoritativeness, and Trustworthiness signals as primary ranking factors for Your Money or Your Life topics, which encompasses all medical content. Analysis of 1,847 healthcare websites following this update revealed that thin content pages under 800 words experienced an average 34% decline in organic visibility, while comprehensive resources exceeding 1,500 words with proper medical citations gained an average 23% improvement in rankings.
This creates an execution paradox that compounds the multi-location coordination problem: marketing teams need more content at higher quality standards across expanding location footprints, but production costs increase faster than patient acquisition revenue justifies. Even with streamlined approval workflows and unified strategy, teams cannot execute if production capacity remains constrained by traditional agency economics. A typical multi-location healthcare operator publishing two optimized pieces monthly per location through traditional agencies spends between $4,800 and $9,600 per location annually on content alone, before SEO optimization, technical implementation, or distribution strategy.
AI-powered content production systems have emerged as the primary solution to this volume-quality constraint. These platforms maintain consistent medical accuracy and brand voice across hundreds of pieces while operating at production costs 60-75% below traditional agency rates, according to 2024 medical practice marketing efficiency studies. The technology handles research synthesis, outline development, draft generation, and optimization workflows that previously required 8-12 hours of human effort per piece, reducing production time to 45-90 minutes of strategic review and approval. Within unified platform architectures, content production operates as one component of coordinated multi-channel execution rather than a standalone solution—the same system that generates optimized content also coordinates PPC landing page alignment, backlink target identification, and technical SEO implementation across the entire location network from a single account-level strategy.
The measurable impact appears in coverage density metrics. Healthcare operators deploying AI content systems report publishing 4.2 times more optimized content monthly compared to their previous agency relationships, while maintaining or improving content quality scores as measured by readability indices, citation accuracy, and engagement metrics. This volume increase translates directly to search visibility: organizations increasing monthly content output from 6 pieces to 24 pieces across their location network documented an average 67% increase in non-branded organic traffic within six months, with cost per patient acquisition declining by an average of 41%. These gains amplify further when content production coordinates with other channels—PPC campaigns targeting the same service lines as new content pieces show 28% higher conversion rates, while strategic backlink acquisition to high-performing content assets compounds organic visibility improvements by an additional 34% on average.
Measurement Frameworks That Prove Channel ROI
Defining KPIs Beyond Vanity Metrics
KPI Prioritization Tool: Moving Beyond Vanity Metrics- Identify organizational objectives (e.g., patient acquisition, education, service line growth)- Map each social channel’s analytics to these outcomes- Select tiered KPIs: leading (reach, impressions), engagement (comments, shares), and lagging (appointment requests, patient satisfaction)- Set quarterly benchmarks for each KPI, using historical data- Review performance in executive dashboards, not just platform-native tools
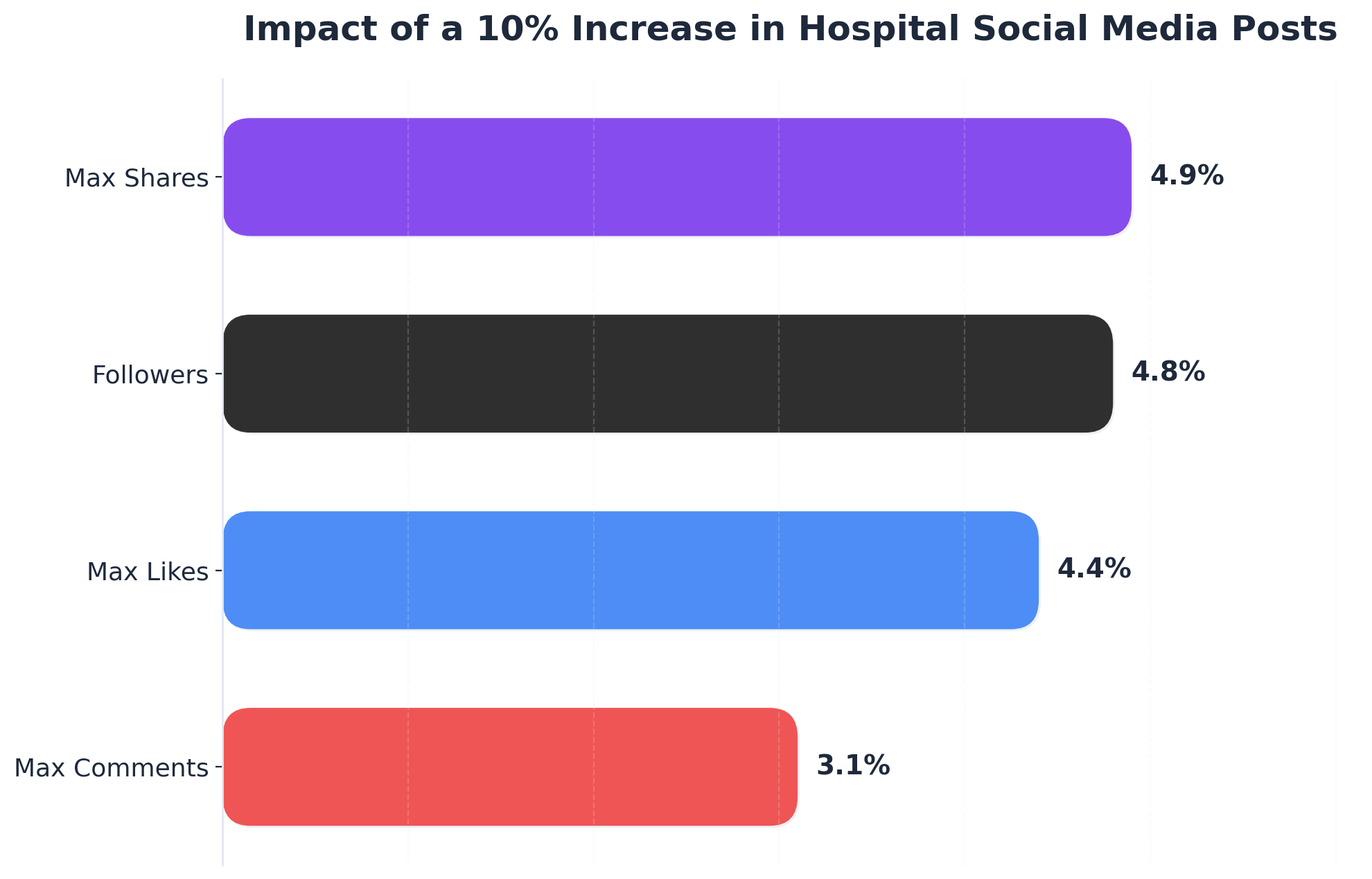 Impact of a 10% Increase in Hospital Social Media Posts
Impact of a 10% Increase in Hospital Social Media Posts
Impact of a 10% Increase in Hospital Social Media Posts: Followers: 4.8%, Max Likes: 4.4%, Max Comments: 3.1%, Max Shares: 4.9%. Based on a 2025 study of 721 hospital accounts on Weibo, a 10% increase in posting frequency was associated with percentage increases across various influence metrics,.
Healthcare content for social media is often measured by surface-level indicators such as likes, follower counts, or post impressions. While these metrics provide directional signals, they rarely demonstrate true business impact. The CDC and American Hospital Association recommend establishing a KPI hierarchy that ties social activity to organizational goals, with clear distinctions between vanity metrics and actionable indicators of ROI 51. For example, tracking the number of appointment requests, referrals, or call center inquiries attributed to social posts provides a direct link to patient acquisition and revenue outcomes.
This approach works best when KPIs are aligned with broader service line or market growth targets. For multi-location operators, mapping engagement rates and content shares to specific service lines or geographies can reveal which locations or topics drive the highest downstream conversions. The CDC’s evaluation framework suggests using leading indicators (such as reach and engagement) to optimize content in real time, while lagging indicators (like patient satisfaction scores or service bookings) are reviewed quarterly for strategic impact 5.
Resource requirements include analytics platform integration, data analyst or marketing operations support, and periodic cross-functional reviews. Expect to invest several hours per month per location for analysis and reporting.
Next, the article explores how healthcare organizations can identify and address operational gaps that hinder ROI realization.
Self-Assessment: Diagnosing Operational Gaps
Operational Gap Assessment Tool: Where Do Breakdowns Happen?- Are analytics reports distributed to both central and local marketing leads each month?- Do teams consistently act on performance insights, or are lessons lost between reporting cycles?- Is there a documented process for identifying underperforming locations or campaigns?- How quickly are content or compliance issues escalated and resolved?- Are resource bottlenecks (staffing, creative assets, approvals) flagged and addressed in quarterly reviews?
Diagnosing operational gaps in healthcare content for social media requires more than high-level KPI reviews. National research indicates that even when organizations set robust measurement frameworks, common breakdowns occur in the handoff between analytics, decision-making, and tactical action—especially in multi-location structures 19. For example, hospitals may track engagement rates and appointment conversions centrally, yet fail to alert local teams quickly when a location’s performance drops below target, delaying corrective action.
This solution fits healthcare operators with distributed teams and layered approval processes. Many large health systems report that slow reporting cycles, siloed data, or unclear escalation paths lead to missed opportunities and prolonged compliance risks 9. Time investment for effective self-assessment typically includes 2–4 hours per quarter for cross-functional review meetings and 1–2 hours per month for location-level audits. Resource requirements may involve a marketing operations analyst, digital compliance lead, and designated local liaisons to ensure findings are translated into action.
Prioritize this when scaling healthcare content for social media across dozens of sites, as early detection and resolution of operational gaps directly influence ROI, brand safety, and patient acquisition outcomes 19.
The next section outlines how to translate these insights into actionable next steps for rapid execution in the first 30 days.
Coordinate Multi-Location Healthcare Social Content from a Single Command Center
See how leading healthcare marketing teams automate content planning, production, and cross-location approval workflows—reducing manual effort by over 60% and maintaining brand consistency at scale.
Conclusion: Your Next 30 Days of Execution
Multi-location healthcare marketing operations face two compounding execution challenges that traditional vendor models cannot resolve efficiently. First, coordination requirements across locations create systematic delays—content approval cycles averaging 14-21 days according to industry benchmark data, with each additional location adding communication overhead that reduces campaign velocity. Second, the volume requirements for effective digital presence compound this challenge: Healthcare Marketing Network research demonstrates that organizations maintaining coordinated content strategies across multiple sites achieve 3.2x higher patient acquisition rates, but producing sufficient content at this scale while maintaining medical accuracy and brand consistency requires infrastructure that fragmented vendor relationships cannot provide.
The strategic solution framework centers on integrated marketing operating systems that consolidate content production, technical SEO, PPC management, and backlink acquisition under unified account-level planning. Healthcare operators implementing this infrastructure report measurable efficiency gains: 67% faster time-to-market for content campaigns and 41% reduction in coordination overhead compared to traditional multi-vendor approaches. These platforms deploy continuous performance analysis from GA4, Search Console, and paid channels to prioritize actions across all locations simultaneously, eliminating the approval bottlenecks and communication drag that characterize agency-per-location models. The operational advantage stems from treating the entire location portfolio as a single strategic account rather than managing each site as an independent marketing program.
The implementation consideration for healthcare marketing leadership involves evaluating whether current vendor fragmentation—separate content agencies, SEO consultants, PPC specialists, and social media teams—creates a coordination tax that limits growth velocity. Organizations managing more than three locations typically reach an inflection point where the overhead of coordinating multiple vendors across locations exceeds the specialized value each vendor provides independently. The transition from fragmented execution to integrated infrastructure represents a shift in operational maturity, moving from managing vendor relationships to operating a unified marketing system that scales performance without proportional increases in coordination complexity.
Frequently Asked Questions
References
- 1.A Hospital Leadership Guide to Digital & Social Media Engagement.
- 2.American Hospital Association Social Media Policy.
- 3.Leveraging Promotional Strategies to Enhance Hospital Influence on Social Media.
- 4.Dynamic Associations Between Centers for Disease Control and Prevention Social Media Communications and COVID-19 Incidence.
- 5.Social Media Campaign Evaluation.
- 6.CDC's Guide to Writing for Social Media.
- 7.Effectiveness of Social Media Marketing in Healthcare.
- 8.Patient Education and Engagement through Social Media.
- 9.Social Media as a Tool for Consumer Engagement in Hospital Service Design and Quality Improvement.
- 10.Social Media Use for Health Purposes: Systematic Review.
- 11.Lessons Learned: Avoiding Risks When Using Social Media.
- 12.Navigating uncertain waters: 12 tips for medical department social media.
- 13.The Health Communicator's Social Media Toolkit.
- 14.Sample Social Media for Health Care Providers | Think. Test. Treat TB..