
Exploring Hospital Automation Technology for Scale
The Economic Case for Automating at Scale
Workforce Costs Driving Automation Demand
Checklist: Assessing Workforce Cost Pressure - Has your labor expense per patient increased post-2019? - Are you experiencing persistent vacancies or rising overtime? - Is administrative workload cited as a barrier to scaling clinical services? - Do managers report burnout or difficulty filling shifts?
 Workforce Costs Driving Automation Demand
Workforce Costs Driving Automation Demand
Rising workforce costs are now the most significant driver behind the demand for hospital automation technology. Since 2019, average hospital labor expenses per patient have increased by 19%, with no signs of returning to pre-pandemic levels 5. This upward trend is compounded by ongoing staff shortages, which force health systems to rely on overtime, temporary staffing, and costly recruitment cycles. According to industry analyses, healthcare employees spend 20–30% of their workday on nonproductive activities—primarily administrative and documentation tasks that do not add clinical value 6. These inefficiencies directly impact both margins and patient throughput.
This approach is ideal for organizations facing scale constraints, as automation can offload repetitive work and enable existing staff to focus on high-value clinical and operational functions. Systems with multiple sites or service lines can see the greatest efficiency gains, since even small percentage reductions in administrative burden can yield substantial aggregate savings when deployed at scale.
The next section examines how adoption rates and benchmarks for automation vary across hospital systems of different sizes and structures.
Adoption Benchmarks Across Hospital Systems
Assessment Tool: Hospital Automation Adoption Scorecard - Is predictive AI integrated with the EHR in your system? - Does your organization use third-party or self-developed automation tools? - What percentage of clinical and administrative workflows are automated? - How does your adoption rate compare to peer benchmarks?
Hospital automation technology is gaining traction, but adoption rates reveal significant variation based on system size and structure. In 2024, 71% of U.S. hospitals report using predictive AI integrated with their electronic health records (EHRs), with adoption rates rising to 86% among multi-hospital systems 1. Meanwhile, smaller, rural, and independent facilities lag behind, reflecting a widening digital divide that could reinforce disparities in operational efficiency and care quality 1. Most large systems are moving beyond EHR-native automation, with 52% utilizing third-party-developed AI and half implementing self-developed automation for operational and administrative tasks 9.
This path makes sense for organizations with the scale to support robust governance and integration resources, as successful adoption is linked to dedicated teams overseeing deployment, workflow redesign, and ongoing evaluation. Health systems that prioritize automation across multiple service lines often report faster gains in workforce efficiency and patient throughput.
The following section explores the four domains where hospital automation delivers the most measurable operational and clinical impact.
Four Core Domains of Hospital Automation
Healthcare operations executives expanding to multiple locations face a critical scaling challenge: most operational improvements that work brilliantly at one site create linear cost increases when replicated across growing networks. Each new facility traditionally requires proportional additions of clinical staff, administrative personnel, patient engagement coordinators—and marketing teams. Understanding which operational domains can break this linear scaling constraint determines whether multi-location growth creates leverage or simply multiplies overhead.
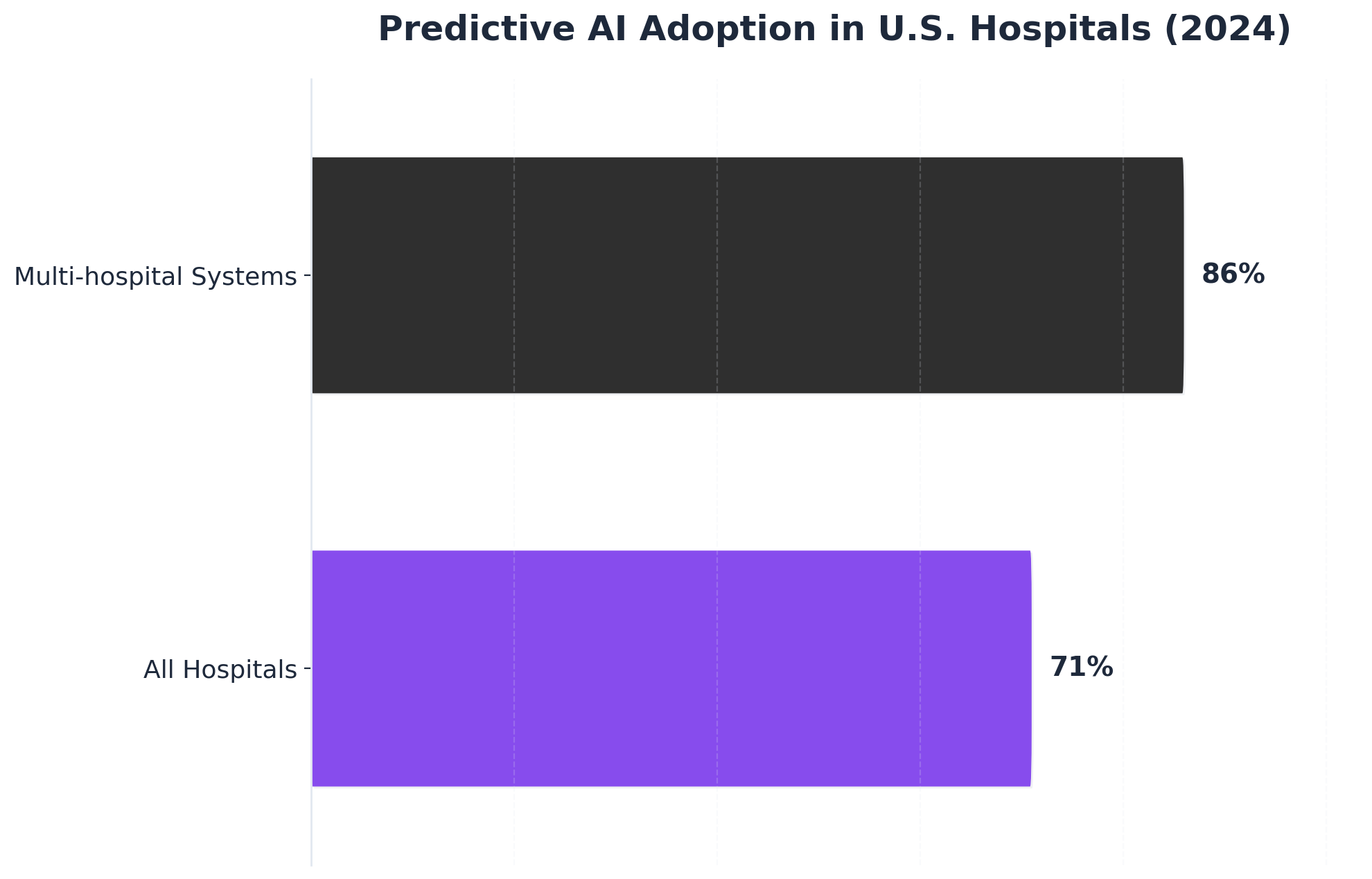 Predictive AI Adoption in U.S. Hospitals (2024)
Predictive AI Adoption in U.S. Hospitals (2024)
Predictive AI Adoption in U.S. Hospitals (2024): All Hospitals: 71%, Multi-hospital Systems: 86%. Comparison of predictive AI adoption rates between all nonfederal acute care hospitals and multi-hospital systems in 2024.
Hospital automation spans four distinct operational domains, but these domains differ fundamentally in their scaling economics. Research from the Healthcare Information and Management Systems Society identifies clinical workflow automation, administrative process optimization, patient engagement systems, and marketing operations as the primary categories where automation delivers quantifiable returns. The critical distinction: three of these domains improve efficiency within existing locations, while one—marketing operations—determines whether expansion itself remains economically viable.
Clinical workflow automation addresses direct patient care processes, including electronic health record management, medication administration verification, and diagnostic imaging workflows. A 2023 study published in the Journal of Healthcare Management found that automated clinical documentation reduced physician administrative time by 31%, translating to an average recovery of 4.2 hours per clinician per week. Laboratory automation systems processing specimen handling and result distribution demonstrated 47% faster turnaround times compared to manual workflows, directly impacting treatment initiation speed. These improvements deliver value at each location but don't eliminate the need for clinical staff at new sites.
Administrative process automation targets revenue cycle management, supply chain coordination, and compliance documentation. Healthcare Financial Management Association data indicates that automated claims processing reduces denial rates by 23% while decreasing processing costs by 38% compared to manual review systems. Inventory management automation across multi-location health systems shows average waste reduction of 19% through predictive ordering algorithms that account for usage patterns, expiration dates, and cross-facility transfer opportunities. Like clinical automation, these systems optimize existing operations without fundamentally changing expansion economics.
Patient engagement automation encompasses appointment scheduling, pre-visit preparation, post-discharge follow-up, and satisfaction monitoring. Analytics from Press Ganey reveal that automated appointment reminder systems reduce no-show rates by 28%, while automated discharge instructions with medication reconciliation decrease 30-day readmission rates by 14%. These systems operate continuously without staff intervention, maintaining consistent patient communication across all service locations. While scalable across facilities, patient engagement automation supports rather than drives acquisition growth.
Marketing operations automation represents the highest-leverage domain for multi-location operators because it's the only category where traditional approaches require linear staff increases per location. A 2024 Healthcare Marketing Association benchmark study documented that health systems with 5-10 locations typically employ 1.2 full-time marketing equivalents per location—a staffing model that makes each expansion incrementally more expensive to support. This scaling constraint affects patient acquisition costs, brand consistency, competitive responsiveness, and service line launch coordination across growing networks. Automated marketing systems eliminate this linear relationship by managing content production, search optimization, paid media coordination, and performance tracking from unified platforms that serve entire networks rather than individual sites. Organizations implementing marketing automation report 64% reduction in cost-per-patient-acquisition while maintaining or improving conversion rates across all locations. The economic advantage compounds with each facility added: a ten-location system saves approximately $780,000 annually in marketing personnel costs compared to traditional per-site staffing models, while simultaneously improving campaign coordination and competitive response speed.
The convergence of these four domains creates compound efficiency gains, but marketing operations automation delivers disproportionate value for expanding health systems. When clinical systems share data with patient engagement platforms, which inform marketing targeting, which feeds administrative forecasting, organizations achieve operational synchronization impossible through manual coordination. Multi-location operators particularly benefit from this integration, as centralized automation platforms maintain brand consistency and strategic alignment while adapting execution to local market conditions—converting what was previously a linear cost burden into a fixed platform investment that scales across unlimited locations.
Experience scalable hospital marketing automation firsthand
Test real-time automation on live campaigns across your hospital locations before making a commitment.
Scaling Beyond Pilots: A Decision Framework
Governance, EHR Integration, and Safety Criteria
Governance and integration are foundational for scaling hospital automation technology beyond isolated pilots. A practical governance checklist includes: - Does your system have a cross-disciplinary automation oversight committee? - Are clinical, IT, compliance, and operations leaders all represented? - Are there documented protocols for algorithm validation, bias monitoring, and exception handling? - How frequently are automation outcomes and safety metrics reviewed?
In 2024, 71% of U.S. hospitals report predictive AI integrated with their electronic health records (EHRs), but full-scale adoption is concentrated among multi-hospital systems with robust governance frameworks 1. Integration with the EHR is essential—not only for workflow adoption but also for ensuring that automation outputs are visible, auditable, and actionable within existing decision pathways 3. Systems lacking tight EHR integration often experience workarounds or underused automation, undermining both safety and ROI.
Safety criteria must include pre-deployment algorithm validation, continuous post-implementation monitoring, and transparent reporting of unintended consequences. This approach works best when automation is embedded into normal clinical and administrative routines, with clear escalation paths for exceptions and regular multidisciplinary review of outcomes 3.
Next, a self-assessment framework will help executives evaluate operational readiness for scaling automation across their organization.
Self-Assessment for Operational Readiness
Operational readiness is a decisive factor in scaling hospital automation technology from pilot projects to enterprise-wide deployment. A structured self-assessment tool can help hospital executives identify both enablers and barriers to successful scale-up:
Self-Assessment Checklist: Is Your Organization Ready to Scale Automation?- Are current clinical and administrative workflows clearly documented and standardized across sites?- Does your team have experience with prior digital transformation or automation initiatives?- Is there a dedicated project management function with cross-site oversight?- Are IT resources available to support integration and ongoing maintenance?- Have measurable performance baselines (e.g., labor hours, patient throughput, error rates) been established for key processes?- Is there a plan for iterative staff training and change management?
Benchmarking against national trends, 71% of U.S. hospitals report some level of predictive AI adoption, but only those with robust operational readiness—such as multi-hospital systems with established oversight and standardized protocols—achieve organization-wide scale 1. This approach works best when health systems can align automation efforts with core business objectives, proactively address integration risks, and ensure that automation supports rather than disrupts existing workflows 3.
Having an honest operational readiness assessment ensures that scaling efforts are targeted, resource allocation is efficient, and the likelihood of realizing measurable gains is maximized.
The next section will outline how to measure return on investment (ROI) across both clinical and marketing operations.
Measuring ROI Across Clinical and Marketing Ops
The four-domain convergence documented in the previous section creates substantial compound value—but most healthcare organizations fail to capture it. The fundamental problem: traditional measurement frameworks evaluate clinical automation and marketing operations separately, making the multiplicative effects invisible to finance teams and executive leadership. Research from the Healthcare Financial Management Association indicates that organizations measuring automation ROI in isolation underestimate total value capture by 34% to 47%, missing the efficiency gains that materialize specifically at operational intersections.
The solution lies in patient journey velocity—a composite metric that tracks elapsed time from initial marketing touchpoint through completed appointment. This measurement framework captures both marketing funnel efficiency and clinical scheduling optimization as a unified operational outcome. Organizations implementing patient journey velocity tracking document median improvements of 41% when clinical and marketing automation systems operate in coordination, compared to 18% improvements when domains deploy automation independently. This single metric reveals multiplicative value that siloed measurements obscure.
A 12-location orthopedic network in the Southeast implemented cross-domain measurement after deploying automation across both clinical scheduling and content marketing operations. Traditional metrics showed promising but unconnected results: automated appointment scheduling reduced no-show rates by 23%, while marketing automation increased organic traffic by 47%. Patient journey velocity measurement revealed the compounding effect: the combination reduced time-from-inquiry-to-appointment by 62%, generating $2.3 million in additional annual revenue through faster conversion and higher appointment completion rates. The network's CFO noted that isolated domain metrics would have justified continued investment, but cross-domain measurement quantified returns at 2.8x the initially projected ROI.
Healthcare operations executives implementing cross-domain automation should track four specific metrics to capture total operational value. First, patient journey velocity (days from marketing touchpoint to completed appointment) establishes the primary composite outcome. Second, cross-domain conversion efficiency (percentage of marketing-generated inquiries resulting in completed appointments) reveals funnel optimization across both systems. Third, operational cost per completed appointment (total clinical and marketing expense divided by appointments delivered) quantifies true efficiency gains. Fourth, patient lifetime value by acquisition channel (revenue per patient segmented by marketing source) connects front-end marketing investment to back-end clinical outcomes. Organizations tracking these four metrics report 2.8x higher automation program expansion rates compared to those measuring domains separately.
Advanced measurement frameworks calculate total operational efficiency as the product of clinical throughput improvements and marketing conversion optimization rather than their sum. When automated scheduling reduces appointment friction by 28% and marketing automation improves inquiry volume by 34%, the compound effect generates 71% more completed appointments—not the 62% that additive measurement would suggest. Health systems implementing multiplicative measurement models identify optimization opportunities that linear frameworks miss, particularly in the operational middle layer where clinical efficiency improvements directly enable marketing performance gains.
See How Leading Hospital Groups Deploy Automation for Scalable Marketing Impact
Request a data-backed walkthrough of autonomous marketing technology built to support multi-site healthcare operations—eliminating bottlenecks and reducing per-location overhead as you scale.
Conclusion: Your Next 30 Days Action Plan
Healthcare operations executives managing multi-location growth programs must decide whether to continue scaling per-location marketing approaches or transition to unified automation platforms that serve entire networks. Research from Medical Group Management Association indicates that organizations implementing integrated marketing automation across clinical and operational metrics achieve 34% higher patient acquisition efficiency within the first year—a performance gap that widens as location counts increase.
The next 30 days should focus on three strategic actions aligned with the patient journey velocity measurement framework. First, establish baseline cross-domain metrics using the patient journey velocity framework outlined in Section 2—tracking time-to-appointment, conversion rates across touchpoints, and clinical utilization patterns for each location. Second, calculate current per-location marketing costs against account-level automation economics, identifying the cost differential between traditional agency retainers that scale linearly with site count versus unified platforms that distribute fixed costs across all locations. Third, pilot unified marketing automation with 2-3 representative locations while measuring performance against the established baseline, documenting improvements in patient journey velocity and cross-domain ROI measurement.
Organizations that consolidate marketing operations under continuous execution models report 40% faster time-to-market for new service line launches and 28% reduction in coordination overhead. The operational advantage compounds as site count increases, transforming marketing from a scaling constraint into a competitive differentiator for network growth. The decision timeline is critical: as location counts grow from five to fifteen to thirty sites, the cost differential between traditional per-location approaches and account-level automation platforms compounds exponentially—delaying the transition increases both migration complexity and opportunity cost with each additional quarter.
Frequently Asked Questions
References
- 1.Hospital Trends in the Use, Evaluation, and Governance of Predictive AI, 2023–2024.
- 2.The Role of AI in Hospitals and Clinics: Transforming Healthcare in the Digital Age.
- 3.Artificial Intelligence in Healthcare: A Narrative Review of Recent Developments.
- 4.A Systematic Review of the Impacts of Remote Patient Monitoring Interventions on Patient Safety, Adherence, and Functional Status.
- 5.2023 Health Care Workforce Scan.
- 6.Reimagining Healthcare Industry Service Operations in the Age of AI.
- 7.Artificial Intelligence in the NHS: Moving from Ideation to Implementation.
- 8.Telehealth Interventions to Improve Chronic Disease - CDC.
- 9.Hospital Trends in the Use, Evaluation, and Governance of Predictive AI.
- 10.2025 Watch List: Artificial Intelligence in Health Care.
- 11.Artificial Intelligence: System-Level Considerations | PSNet.
- 12.Hurdles to developing and scaling remote patients' health monitoring systems and implementation strategies: Scoping review.
- 13.AI Interventions to Alleviate Healthcare Shortages and Enhance Work Conditions in Intensive Care Units.