Key Takeaways
- The May 2026 HHS Section 504 deadline requires WCAG 2.1 AA conformance across every location page, portal, and embedded widget tied to federal funding 15.
- A defensible medical web program operates as five layers: trust architecture with Physician schema, conversion architecture, Core Web Vitals, HIPAA and accessibility compliance, and an evidence-graded content engine.
- Standard GA4 is not HIPAA compliant on PHI-adjacent URLs; remediation requires server-side parameter stripping, a BAA-covered analytics tool, or a bifurcated property 7.
- Portfolio governance depends on locked components owned by marketing operations and unlocked local fields owned by location leads, enforced by the CMS rather than a style guide PDF.
The May 2024 Rule That Reset the Definition of 'Good'
On July 8, 2024, the Department of Health and Human Services issued a final rule requiring recipients of HHS federal financial assistance to bring their websites, mobile apps, and digital content to Web Content Accessibility Guidelines 2.1 Level AA conformance 1. The compliance runway is short: May 11, 2026 for entities with 15 or more employees, and May 10, 2027 for those under 15 5. For multi-location operators, this means every location page, patient portal entry point, and embedded scheduling widget across the portfolio is now on a fixed legal clock.
This rule changes what 'good' means in medical website design. Until last year, accessibility was often deferred. The new standard pulls it into the same compliance category as HIPAA's Security Rule 2. A 25-location orthopedic group cannot remediate one flagship site and consider the program complete. The obligation extends to every digital surface that receives federal funding.
The practical consequence for a VP of Marketing is that the redesign question is no longer whether to invest, but whether the existing creative, development, and agency stack can deliver portfolio-wide conformance on schedule. Most cannot. WCAG 2.1 AA touches color contrast ratios, keyboard navigation paths, focus states, alt text discipline, form labeling, video captioning, and PDF accessibility—across hundreds of templates and thousands of pages.
What follows is a five-layer operating model for evaluating a medical web footprint against the May 2026 deadline and the conversion benchmarks that determine patient acquisition cost. Design is the visible output. The system underneath is what gets audited.
The Five-Layer Operating Stack
Trust Architecture: Credentials as Structured Data
Trust on a medical website is built by machine-readable proof that a real, credentialed clinician stands behind the page. Schema.org's Physician type encodes the specifics search engines need: medical specialty, hospital affiliation, primary practice location, available services, and the relationship between a provider and the organization that employs them 8. When that markup is present and accurate, Google can populate knowledge panels and rich results with credential data pulled directly from the page rather than from third-party directories the operator does not control.
Most multi-location operators ship provider bio pages that look polished but carry no structured data. The result is a portfolio of hundreds of clinician pages competing for branded provider searches against Healthgrades, WebMD, and Vitals, all of which mark up the same data correctly.
The operator move is to standardize a Physician schema template at the account level and enforce it as part of the page-publishing workflow. Each provider record carries a fixed schema block populated from a single source of truth: NPI, specialty taxonomy, hospital affiliations, and location IDs. When a provider transfers between locations, the schema updates everywhere the bio appears.
Beyond schema, trust architecture covers visible signals that map to verifiable data: board certifications shown as the issuing board's logo with an expiration date, malpractice history disclosure where state law requires it, and patient review aggregates pulled from Google Business Profile rather than self-curated quotes. Trust is what survives a skeptical patient cross-checking the page against an external registry.
Conversion Architecture and the Multi-Step Form Paradox
The intake form is where most medical websites lose the patient. Sixty-seven percent of users abandon forms before completing them, a figure that has been cited in conversion research for years. While operators often interpret this as a need to shorten forms, well-designed multi-step forms can lift conversions by as much as 300 percent over single-page equivalents, even with the same total field count.
This paradox resolves when perception is separated from arithmetic. A patient viewing a single-page form with 14 fields sees a wall. The same 14 fields presented across four steps—reason for visit, insurance, contact, preferred time—feel like a sequence of small decisions. Progressive disclosure also allows the form to branch: an orthopedic intake form can ask different questions for a sports-injury visit versus a joint-replacement consultation, without showing irrelevant fields.
Conversion architecture extends beyond the form. The primary action on every service-line page should be consistent in verb and vertical position: schedule, request, or call. Phone numbers need to be tap-to-dial on mobile and linked to a tracked number that routes to the correct location. Calendar embeds should pre-filter by provider, location, and visit type before displaying availability; an empty calendar is less effective than no calendar.
The metric to govern this layer is appointment-request rate per session, segmented by service line and location, not a generic site conversion rate. An aggregate conversion rate can obscure issues, such as an orthopedic location converting at 4.2 percent next to a dermatology location converting at 0.8 percent, indicating a failure in the form architecture for the latter.
Two architectural choices must be resolved before any visual redesign: whether the booking flow resides within the website domain or hands off to a third-party scheduling subdomain, and whether the form posts directly to the EHR or to a marketing CRM requiring manual reconciliation. Both choices have downstream consequences for HIPAA scope and lead-source reporting that front-end polish cannot fix.
Technical Foundation: Core Web Vitals and Content-Driven Breakpoints
Core Web Vitals are the floor, not the ceiling. Largest Contentful Paint, Interaction to Next Paint, and Cumulative Layout Shift are direct Google ranking signals and the closest proxy for how a real patient experiences the page on a mid-tier Android device on cellular 4. A one-second delay in load time correlates with a seven percent reduction in conversion rate 4, and this delay disproportionately affects patients searching urgent-care queries on mobile when practices are closed.
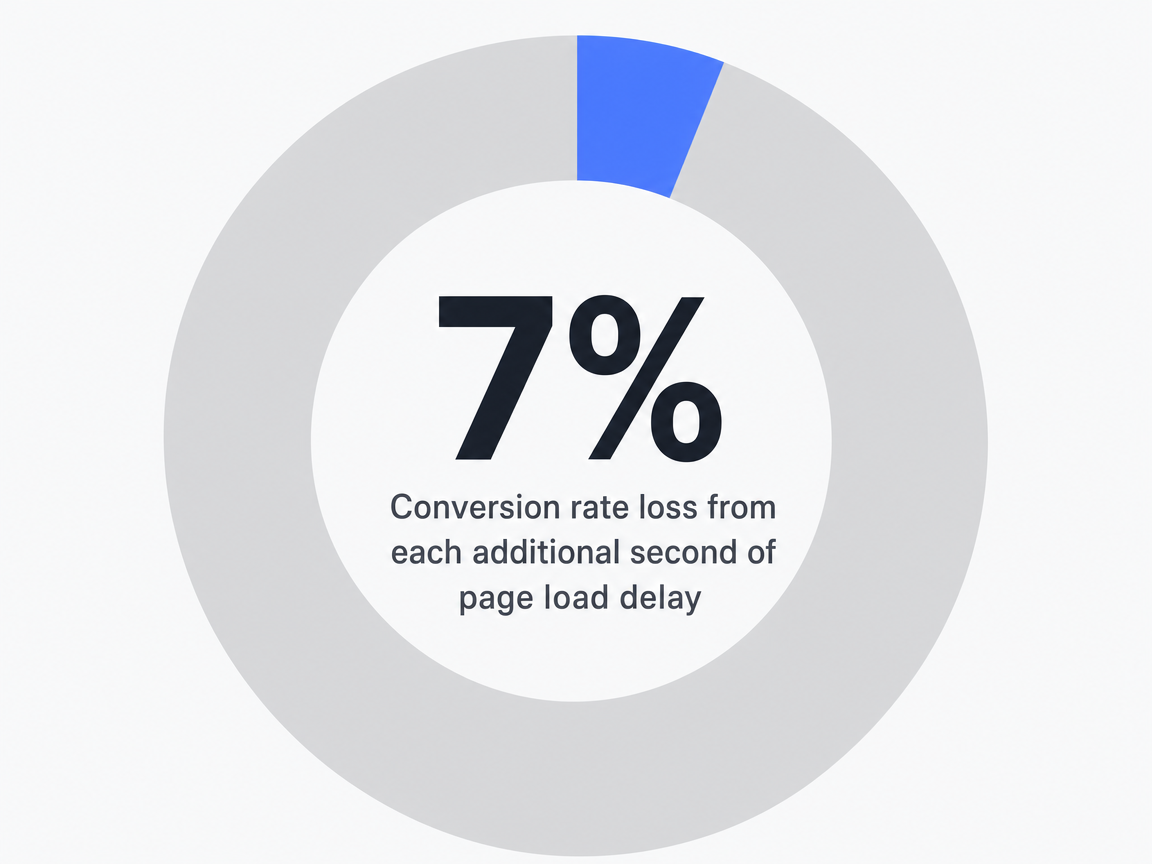 Conversion rate loss from each additional second of page load delay: 7%
Conversion rate loss from each additional second of page load delay: 7%
Targets for location pages include: LCP under 2.5 seconds on the 75th-percentile mobile session, INP under 200 milliseconds, and CLS under 0.1. Achieving these numbers is rarely a CSS problem; it is almost always due to third-party scripts—chat widgets, marketing pixels, review aggregators, and analytics tags—that load synchronously and block rendering. An audit that strips the homepage to first-party assets and then reintroduces tags one at a time will identify offenders faster than synthetic tests.
Responsive design has evolved beyond device-width breakpoints. Current best practice uses content-driven breakpoints: layout adjusts where the content itself starts to break, not at a memorized list of pixel widths 9. For a provider directory, this might mean the card grid drops from four columns to two at 920 pixels because that is where the provider name starts to wrap awkwardly, regardless of the device class.
The technical foundation also covers image discipline. Provider headshots and facility photography are typically the largest assets on a medical site and offer the easiest LCP win. Serving them as AVIF or WebP at the actual rendered dimensions, with explicit width and height attributes to prevent layout shift, eliminates a category of performance regressions that often reappear when non-developers upload large JPEGs through the CMS.
Compliance Perimeter: HIPAA, Section 504, and the GA4 Problem
The compliance perimeter involves two layered regulatory regimes, and most marketing teams inherit a stack that satisfies neither.
HIPAA's Security Rule requires administrative, physical, and technical safeguards for electronic protected health information (ePHI) 2. The Section 504 final rule adds WCAG 2.1 AA conformance as a separate obligation tied to federal financial assistance 1. These rules do not overlap cleanly. A site can be fully accessible yet leak ePHI, or be HIPAA-tight yet fail keyboard navigation. Both audits must run in parallel.
The GA4 problem is one most marketing teams are unaware of. Standard Google Analytics is not HIPAA compliant. Google does not offer a Business Associate Agreement for GA4, and the platform collects persistent identifiers—client IDs, IP addresses, device fingerprints—that, when combined with URL paths containing condition names or appointment-type parameters, can constitute disclosure of PHI to a third party without authorization 7. A URL like /schedule/oncology-consultation?provider=jones loaded by an identifiable user is a HIPAA event, not just a pageview.
The remediation path has three options. First, strip every PHI-adjacent parameter from URLs and event payloads before GA4 sees them, using a server-side tag manager. Second, replace GA4 on PHI-adjacent paths with an analytics platform that signs a BAA and self-hosts data. Third, used by larger systems, bifurcate the property: a marketing GA4 install on top-of-funnel pages, and a BAA-covered analytics tool on patient-portal and scheduling paths.
The Section 504 work runs in parallel. WCAG 2.1 AA conformance is testable: contrast ratios above 4.5:1 for normal text, all interactive elements reachable by keyboard, visible focus states, alt text on every meaningful image, captions on every video, programmatically labeled form fields, and PDFs either remediated or replaced with HTML equivalents. The compliance deadline for entities with 15 or more employees is May 11, 2026 5. Inventory work not started by Q1 of that year will not finish on time, especially for operators with thousands of legacy PDFs in resource libraries.
Content Engine: Evidence Over Narrative
The content layer is where most medical websites either earn organic acquisition or quietly subsidize paid search indefinitely. Behavioral data is unambiguous: 75 percent of online health information consumers report that the content they find online has a minor or major impact on their health decisions, and over 60 percent search for health information at least weekly 3. The audience is large, returning, and engaged.
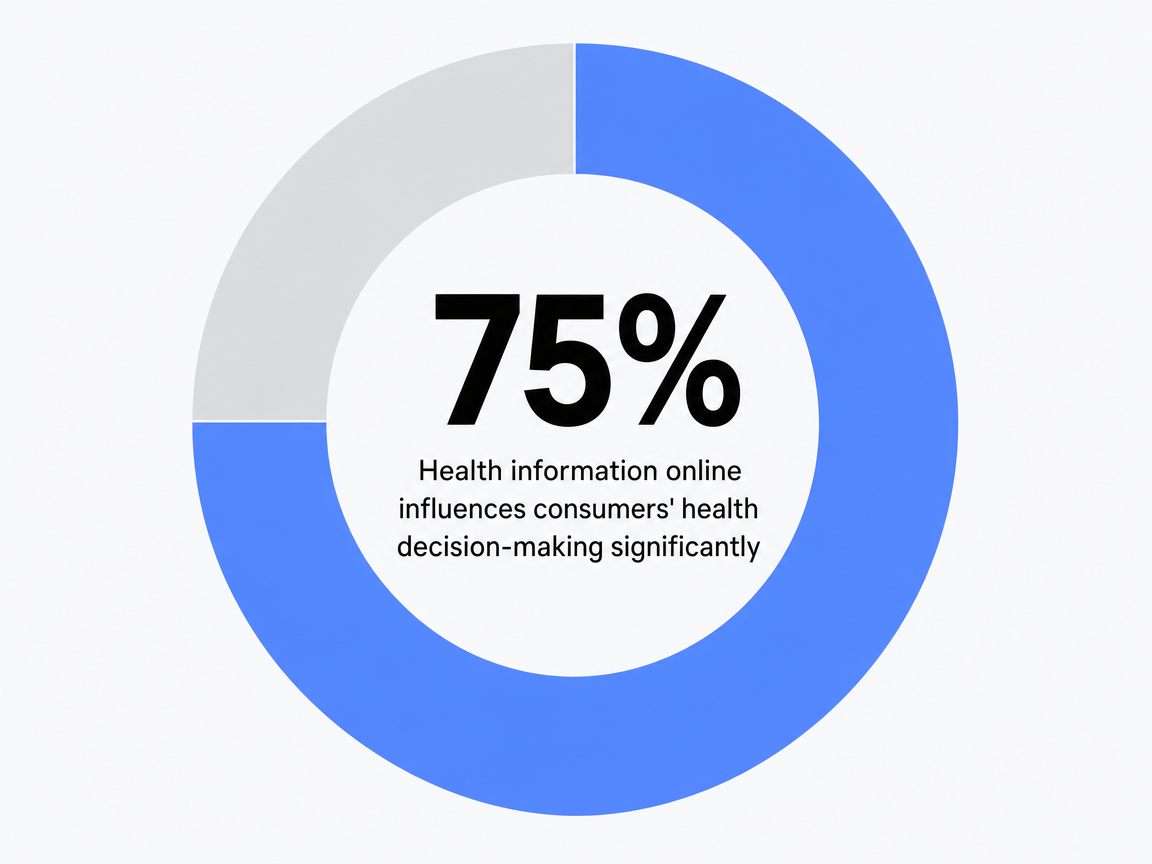 Health information online influences consumers’ health decision-making significantly: 75%
Health information online influences consumers’ health decision-making significantly: 75%
What they read matters. A study of medical blog readers found that 53 percent took preventative health action after reading—self-checks, asking a physician about risk factors, requesting screenings—and that evidence-based content with statistics outperformed personal-narrative content in motivating that action 6. While patient stories drive identification, numbers drive behavior.
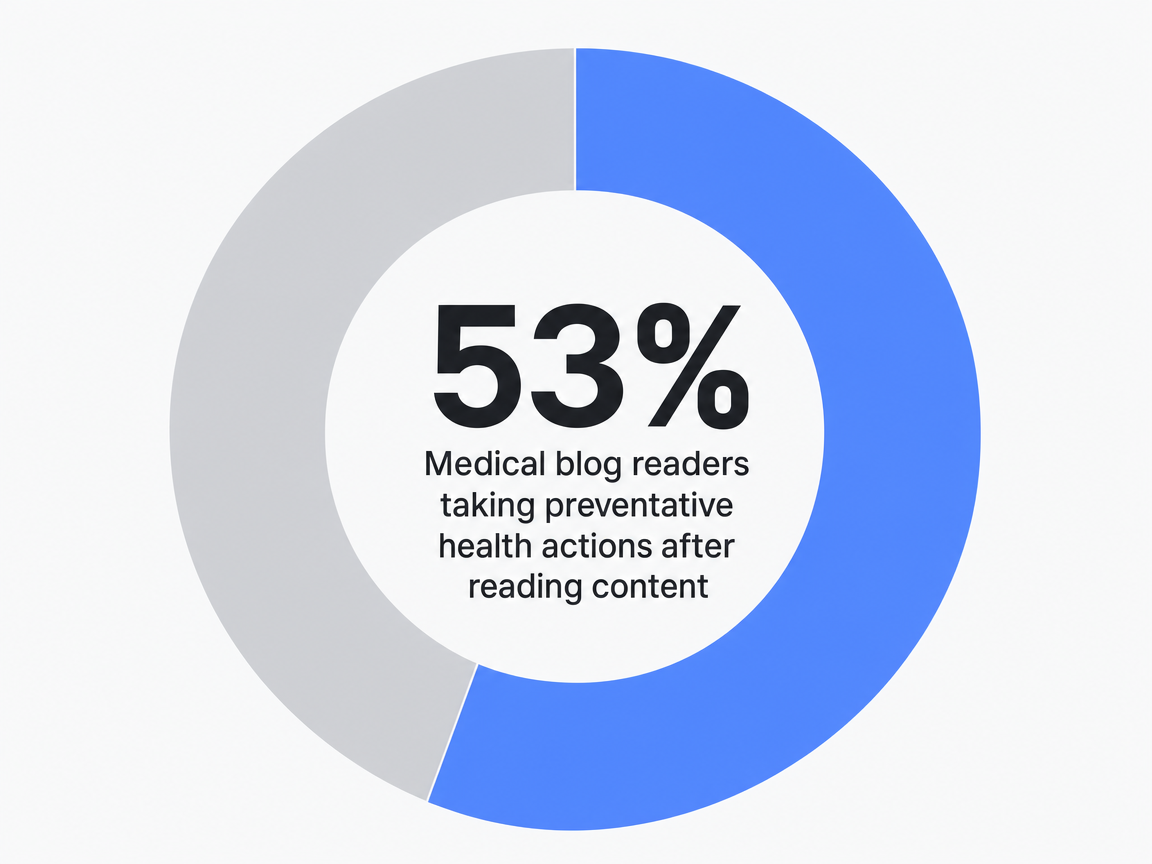 Medical blog readers taking preventative health actions after reading content: 53%
Medical blog readers taking preventative health actions after reading content: 53%
The operator implication is to build the content engine around clinical depth rather than lifestyle adjacency. A condition page that includes prevalence data, evidence-graded treatment options, and recovery timelines outperforms one that opens with a metaphor about taking the first step. Similarly, a 1,200-word piece by a fellowship-trained surgeon, reviewed for medical accuracy, outperforms five 400-word pieces by a generalist freelancer without clinical review.
For a multi-location operator, the engine must produce at portfolio scale. A 25-location group covering six service lines needs approximately 150 service-line pages, plus ongoing condition coverage, location-specific procedure pages, and provider bios. This volume cannot be sustained by a small in-house team or by per-location agency contracts that reauthor the same orthopedic content repeatedly. The economic question—how to produce evidence-graded medical content at the required cadence and breadth—is addressed in the following sections.
Test Data-Driven Medical Website Content Live
Experience a measurable impact by publishing and analyzing real medical website content during your trial.
Visual System: Color, Photography, and Consistency
Blue dominates healthcare branding because it consistently performs well. Eighty-five percent of leading healthcare companies use blue in their identity systems 10, not for fashion, but for function: cool palettes reduce visible tension in patients who are already anxious. The decision for operators is not whether to use blue, but whether to commit to a single accent color that signals primary action across the portfolio—every schedule button, phone link, and form submit—or to allow each location's web vendor to choose its own.
Photography requires similar discipline. Stock images of smiling clinicians in unrelated facilities undermine credibility. Authentic photography of real providers in actual exam rooms, shot once for the entire portfolio and recropped per page, costs less per location than licensing fees for multiple rounds of stock photos and looks unmistakably genuine.
The visual system works effectively when governed and fails quietly when not. The challenge is how to govern it across multiple locations without flattening their individual distinctions.
Governing Design Across 25 Locations
Locked vs Unlocked Components in a Portfolio Brand System
A portfolio brand system that scales across 25 locations relies on a clear distinction between what every page must share and what each page is allowed to change. Locked components are those where deviation creates compliance risk, brand drift, or measurement chaos. Unlocked components are where deviation is intended.
The locked list is short and non-negotiable: the global header and footer, the primary navigation taxonomy, the typography scale, the accent color for primary actions, the appointment-request component, the Physician schema template 8, accessibility patterns required for WCAG 2.1 AA conformance 1, and the analytics tag configuration that keeps the property within HIPAA scope 7. If a single location modifies these components, the portfolio risks audit failure or inaccurate reporting.
The unlocked list is where each location earns its local search position: provider bios with specialty-specific schema fields, service-line copy reflecting actual procedures at that site, hours, parking, physical accessibility details, location-specific photography of exam rooms, accepted insurance, and local trust signals like hospital affiliations or community partnerships.
The governance model that makes this work involves component-level publishing rights: marketing operations owns the locked layer, location managers and clinical leads own the unlocked layer, and the CMS enforces this boundary directly in the editor, rather than through a disregarded PDF style guide.
Consolidation Economics: Per-Location Agency vs Account-Level Execution
The cost structure of managing 25 location websites under a per-location agency model often delays real redesigns for multi-location operators. Each location typically has its own retainer, scope of work, and receives repeated versions of the same orthopedic content. The accessibility remediation required by the May 2026 deadline 5 then becomes a separate, additional per-location project.
The account-level alternative consolidates strategy, content production, technical SEO, accessibility remediation, and PPC coordination under a single program operating against one brand system. The table below outlines variables operators should populate from their own contracts to evaluate both models.
| Workstream | Per-Location Agency Model | Account-Level Execution Model | Delta |
|---|---|---|---|
| Strategy | Retainer × 25 locations (variable) | Single account-level plan | Operator-calculated |
| Content production | Per-location authoring fee × service lines (variable) | Portfolio content engine, locked templates with unlocked local fields | Operator-calculated |
| Technical SEO | Per-site audit and implementation (variable) | Account-level audit, templated fixes deployed once | Operator-calculated |
| Accessibility remediation | Per-location WCAG 2.1 AA project before May 2026 (variable) | Locked accessibility patterns enforced once across the portfolio | Operator-calculated |
| PPC coordination | Per-location campaign management fee (variable) | Account-level bid and budget logic across geographies | Operator-calculated |
| Reporting | 25 separate dashboards reconciled manually | Single account view, segmented by location and service line | Operator-calculated |
| Trial entry point | Not applicable | $599/mo after a two-week trial (Vectoron) | Hard reference price |
The deciding factor is not the per-line-item comparison, but how many of the 25 locations genuinely receive differentiated strategic thinking under the agency model versus how many receive the same playbook with only the location name swapped. If 23 locations receive the same playbook, the agency model charges 25 times for work that should be priced once.
Unlock Data-Driven Medical Website Design for Scalable Growth
Connect with our experts to see how unified, AI-powered design and strategy deliver measurable ROI, faster site launches, and seamless brand governance across all healthcare locations.
An Audit Checklist Before the 2026 Deadline
The work required before May 11, 2026, is not creative; it is inventory, measurement, and remediation against fixed standards. Operators who approach the next 18 months as a redesign project will miss the deadline. Those who treat it as a portfolio audit with a remediation backlog will succeed.
The checklist below represents the minimum scope an internal team or outside auditor should apply to every location domain before the WCAG 2.1 AA deadline 15.
- Accessibility inventory: Catalog every page template, PDF in resource libraries, embedded video, and third-party widget. Flag PDFs older than three years for replacement with HTML rather than remediation.
- Contrast and keyboard audit: Conduct an automated scan plus a manual keyboard-only walkthrough of the appointment-request path on each location's primary service line.
- Analytics scope review: Map every URL pattern touching scheduling, conditions, or provider names against the GA4 property to identify HIPAA exposure 27.
- Schema coverage: Confirm Physician markup on every provider bio and Organization markup on every location page 8.
- Core Web Vitals baseline: Capture 75th-percentile LCP, INP, and CLS per location, per service line 4.
- Form architecture review: Analyze abandonment rate by step and location, creating a remediation list ranked by appointment volume.
- Component governance: Establish a written locked-vs-unlocked specification that the CMS actively enforces.
The output is a remediation backlog scored by deadline risk and patient acquisition impact. This document, not a moodboard, defines a successful medical website program in 2025.
Frequently Asked Questions
References
- 1.Accessibility for Web Content, Mobile Apps, and Kiosks.
- 2.Summary of the HIPAA Security Rule.
- 3.Online Health Information Seeking Behavior among Patients in a Tertiary Care Hospital in a Developing Country.
- 4.Core Web Vitals for Healthcare Websites.
- 5.HHS Issues Final Rule on Digital Accessibility Requirements for Section 504 Recipients.
- 6.Impact of Medical Blog Reading on Disease Prevention and Health Promotion Behaviors.
- 7.Is Google Analytics HIPAA Compliant?.
- 8.Schema.org - Physician.
- 9.Responsive Design Breakpoints: A Guide.
- 10.The Psychology of Color in Healthcare Branding.