
Key Takeaways
- Treat E-E-A-T as conversion infrastructure rather than an SEO checklist, since the credentials, licensure, and payer signals Google evaluators check are the same ones prospective patients scan before calling 9.
- Prioritize above-the-fold licensure blocks, named clinical directors with credentials, accreditation marks linked to issuing bodies, specific payer lists, and same-day verification paths over brand copy or testimonial galleries 3.
- For multi-site operators, centralize the clinical review board, editorial policy, citation library, and ownership disclosures at the brand level while keeping licensure, payers, on-site clinical lead, and verification path local 11.
- Close the loop by tagging thirty days of inbound calls against the pages that generated them, then audit licensure, payer accuracy, reviewer bylines, citations, and ownership pages each quarter.
Why Intake Yield Lives or Dies on Trust Signals
Admissions teams face the challenge of rising paid traffic and stagnant qualified-call rates, with intake coordinators spending significant time on inquiries unlikely to convert. The root cause often lies not in the media plan, but in the crucial period between a click and a call, where prospective patients or family members assess the credibility, credentials, and insurance acceptance of a program.
This decision is not primarily driven by aesthetics. A 2022 Journal of Patient Experience study of US adults highlighted that medical license, certification, and insurance acceptance were the most critical factors in choosing a provider 9. Softer signals like testimonials or lifestyle photography were less influential. The signals patients use to decide whether to call are consistent with what Google's quality evaluators look for on "Your Money or Your Life" (YMYL) pages.
This alignment presents an opportunity. By treating experience, expertise, authoritativeness, and trust (E-E-A-T) as foundational conversion infrastructure, rather than just an SEO checklist, programs can significantly improve intake yield. This article explores where these signals reside, which ones boost qualified-inquiry rates, and how recorded-call evidence can confirm their effectiveness.
What Prospective Patients Actually Scan Before They Call
The Credentials and Coverage Hierarchy
When prospective patients and their families view a level-of-care page, their initial scan is for critical information: licensure, certifications, and clear insurance network status. These elements are prioritized over clinical narratives.
The 2022 Journal of Patient Experience study confirmed that medical license, certification, and insurance acceptance were paramount in provider selection 9. While demographic groups may value softer attributes like bedside manner differently, these should not overshadow the essential credentialing information. This hierarchy dictates the optimal placement of information on a page.
Key information should be prominently displayed above the fold, including:
- State licensure numbers
- Verifiable credentials for the clinical director
- ASAM levels of care offered
- Accreditation marks (e.g., Joint Commission, CARF)
- A specific list of accepted insurance carriers
Audits of underperforming programs often reveal that essential credentialing information is buried, with hero sections dominated by brand language.
Two important operational considerations: First, the payer list must be accurate; listing non-contracted carriers generates unqualified calls and reduces intake yield. Second, certification badges (e.g., LegitScript, state behavioral health authority) should link directly to the issuing body's verification page, not an internal anchor. Patients who prioritize credentials will verify them, and these are the qualified inquiries admissions teams seek.
Structural Friction in Behavioral Health Choice
Behavioral health decisions differ significantly from retail choices. A 2018 study on adults with serious mental illness indicated that psychiatrist supply, out-of-pocket costs, and insurance type heavily influenced treatment decisions 10. While this data is specific to SMI and a few years old, these structural variables—provider scarcity, cost exposure, and plan design—remain significant challenges in many markets.
For admissions, this means a program's webpage competes against factors beyond its direct control: regional clinician shortages, unmet deductibles, and insurance plans that may not cover residential treatment. If a prospective caller cannot quickly ascertain payer fit and cost, they encounter silent friction. Most will close the tab and move to the next program on the search engine results page (SERP).
An earlier economic paper on mental health care highlighted that out-of-pocket price significantly impacts initial provider choice 8. This suggests that price visibility is crucial for the initial decision to call. Programs that clearly outline an insurance verification process, provide a baseline self-pay range, and commit to same-day verification effectively remove the friction that research shows influences initial choice. Conversely, programs that obscure cost behind a form gate risk filtering out qualified inquiries along with unqualified ones.
The Patient Evaluation Checklist Mirrored on Your Pages
Federal consumer guidance, such as MedlinePlus, provides a clear checklist for evaluating health information: who runs and funds the site, content review and currency, and visibility of author credentials, scientific references, and contact information 3, 4. Patients apply this checklist, consciously or unconsciously, when assessing a treatment program's website.
Applying this guidance to a treatment center site means ensuring an "About" or "Ownership" page clearly names the operating entity and any parent organization. Clinical pages should feature a medical reviewer attestation with a date of last review. Clinicians should be named with license numbers and specialties, rather than generic "our team" photos. Clinical claims (e.g., DSM-5-TR criteria, ASAM levels, FDA labels for MAT) require citations to primary sources. A visible phone number and physical address, without scrolling, are also essential. MedlinePlus also cautions that persuasive personal stories can mislead by substituting for evidence 3, indicating that testimonial-heavy pages may convey a false sense of trust by failing to meet patients' actual verification criteria.
Mapping Each E-E-A-T Pillar to a Funnel Stage
Experience as Impression-to-Call Signal
In the context of Google's quality guidelines, "experience" refers to demonstrating firsthand familiarity with a subject. For behavioral health, this means providing specific details that only an operating program would know. Examples include:
- A realistic description of the first 72 hours of detox
- A detailed hourly schedule for a Partial Hospitalization Program (PHP)
- The family communication policy during blackout periods
- Commonly prescribed medications for co-occurring anxiety during stabilization
Such specificity improves the impression-to-call rate by addressing unspoken questions prospective callers have before dialing. Vague statements like "compassionate, individualized care" offer little value. In contrast, a page detailing ASAM 3.5 staffing ratios, psychiatric medication review schedules, and discharge planning cadence demonstrates operational reality. Patient-reported experience of care, as measured by CAHPS and HCAHPS 1, 2, reflects the same informal evaluation patients conduct before making a call.
Expertise as the Clinician Byline Test
Expertise is both easy to feign and easy to verify. The true test is whether a clinician is named, credentialed, and accountable on the page, rather than simply using clinical jargon. A medical reviewer byline, including license number, state, specialty, and date of last review, transforms marketing content into a clinical reference.
Patients have a clear hierarchy for evaluating expertise. The 2022 Journal of Patient Experience study found that medical license, certification, and insurance acceptance were the most important factors for choosing a provider 9. Applied to the conversion funnel, visible expertise signals—named clinicians, license displays, and specialty alignment with the presenting condition—boost impression-to-call rates and streamline the call-to-assessment process by reassuring hesitant families of the program's legitimacy.
The byline test is straightforward: either every clinical page features a verifiable clinician attribution, or it does not. Programs that meet this standard build cumulative expertise across their site, while those that do not rely solely on paid traffic to persuade callers.
Authoritativeness Through Guideline-Grade Governance
Authoritativeness reflects how the broader field perceives a program, alongside the program's internal editorial processes. Admissions teams can draw parallels from clinical guideline development. A 2023 methodological paper on trustworthy clinical practice guidelines emphasizes transparency in development, conflict-of-interest disclosure, and rigorous evidence review 11. While patients may not read such papers, they implicitly apply a similar checklist.
For a treatment center's content, this translates to a documented editorial policy, a named clinical review board with affiliations, citations to primary sources for all clinical claims, and a disclosed funding and ownership structure. External markers of authority also contribute, such as speaking engagements at professional conferences (e.g., ASAM or NAATP), peer-reviewed publications by staff clinicians, and citations from state behavioral health authorities or academic medical centers. These are long-term assets that build authority over time, unlike the transient nature of paid traffic.
Trust as Call-to-Assessment Conversion
Trust is the final pillar that facilitates call conversion. Once a prospective patient or family member calls, the focus shifts from "is this program real?" to "will this program be honest about fit, cost, and timing?" Trust signals on the website establish expectations that the call must then confirm. When these align, the call progresses to assessment; otherwise, the inquiry stalls.
Federal consumer guidance offers a clear framework for "trust signals" at the page level: who operates and funds the site, whether content is reviewed and current, and the visibility of contact information and author credentials 3. A program that transparently publishes its operating entity, payer list, baseline cost, and a commitment to same-day insurance verification provides the intake coordinator with verifiable information rather than requiring them to defend vague claims. Trust, in this context, is not a subjective tone but a set of specific disclosures that callers can verify within the first few minutes of a conversation.
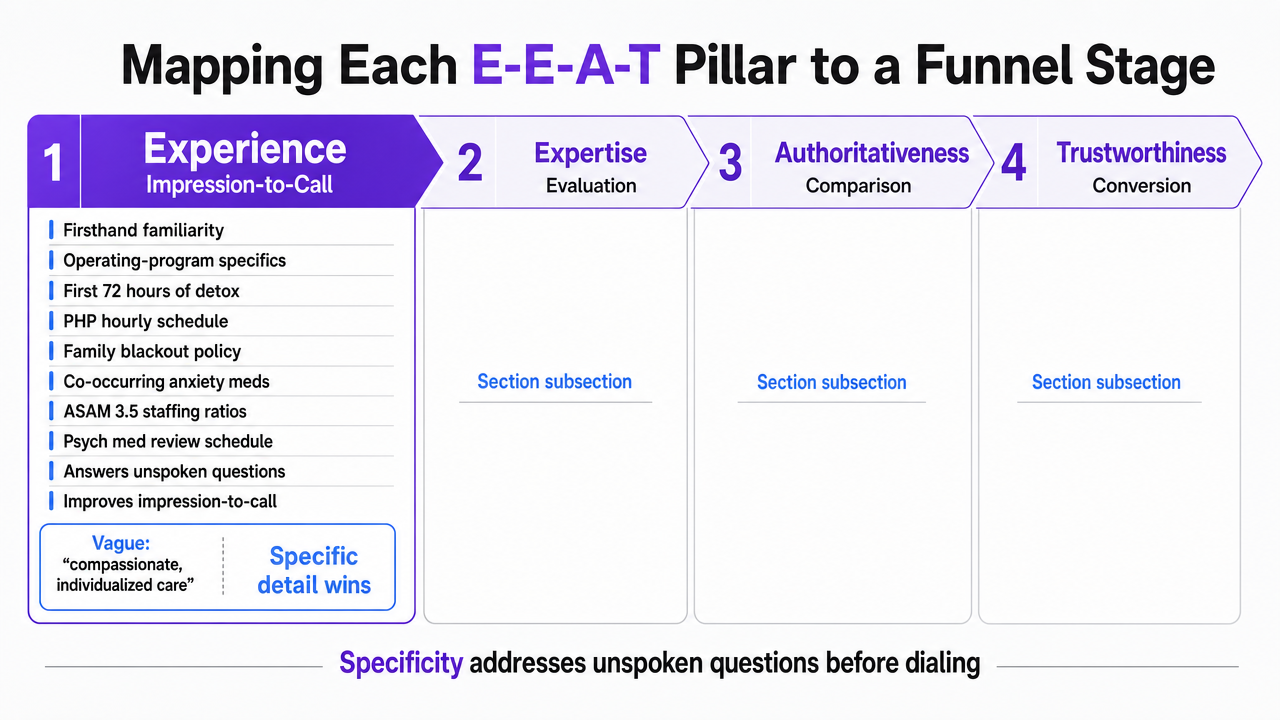 Visualize the four E-E-A-T pillars mapped to specific funnel stages and conversion signals described in the section's four subsections
Visualize the four E-E-A-T pillars mapped to specific funnel stages and conversion signals described in the section's four subsections
Test data-driven E-E-A-T optimization in practice
Evaluate real-world improvements in patient inquiry quality and compliance using live E-E-A-T insights.
The Trust-Source Mix: Where Patients Actually Place Belief
A 2026 Pew Research Center report on health information sources revealed that while many adults use the internet for health topics, trust levels vary significantly. Clinicians are rated as more trustworthy than social media 5. The internet serves as the search layer, while clinicians represent the belief layer; social media ranks considerably lower as a reliable source for healthcare decisions.
This hierarchy dictates the purpose of an admissions site: it should not replace a clinician but rather emulate their credibility. Named clinicians on bylines, license numbers, citations to primary sources, and review dates effectively transfer clinician trust to a digital platform. Lifestyle galleries and curated social feeds do not achieve this.
The unreliability of social-led trust strategies is well-documented. A review of health information on social media found that reliability assessments are often poorly defined and inconsistently applied, raising questions about their accuracy 12. For behavioral health admissions, this has two implications: First, social-proof galleries and testimonial reels are weak trust assets, even before considering HIPAA implications. Second, investing in clinician-authored, citation-backed content aligns with channels patients already trust more.
The practical reallocation of resources is clear: shift budget and review hours from testimonial production to clinician bylines, medical reviewer attestations, and primary-source citations for all clinical claims. The goal is to leverage the trust patients already place in clinicians, rather than relying on social media, which they have largely discounted.
Closing the Loop: From Site Signals to Recorded-Call Evidence
Website trust signals establish expectations, which the intake line either confirms or disproves. Without analyzing the calls generated by these signals, admissions teams are only evaluating half of the conversion funnel—the half that doesn't directly produce revenue.
The process unfolds sequentially: a prospective patient lands on a level-of-care page, reviews the licensure block, scans the payer list, sees a named clinician with a recent review date, and then calls. The subsequent conversation reveals the page's effectiveness. If the caller references specific insurance, ASAM levels, and asks about admission timing, the trust signals successfully attracted a qualified inquiry. Conversely, if the caller is confused about the level of care, expects unoffered services, or names an unlisted payer, the signals generated noise.
Recorded-call analysis completes this feedback loop. By tagging inbound inquiries based on qualification status, mentioned payer, requested level of care, and disqualification reason, admissions teams gain data that the website alone cannot provide. Patterns emerge quickly: a surge in unqualified Aetna calls might point to an overstated network status on the payer list, or a drop in PHP inquiries could be linked to a recent edit removing a staffing-ratio paragraph. The webpage serves as a hypothesis, and the call data provides the evidence.
To maintain an honest feedback loop, two operational habits are crucial: regularly review call tags against their source pages, and integrate intake coordinators' notes into editorial reviews, as they are the first to identify questions the page failed to answer.
See How Leading Patient Acquisition Teams Operationalize E-E-A-T for Measurable Results
Request a data-driven walkthrough tailored for enterprise brands and agencies—learn how to audit, benchmark, and optimize E-E-A-T signals to increase qualified patient inquiries while maintaining compliance.
If You Manage Multiple Locations: Where E-E-A-T Governance Sits
Brand-Level vs. Location-Level Asset Split
For admissions directors overseeing multiple sites, the key is determining which E-E-A-T assets belong at the brand level and which must remain specific to individual location pages. An incorrect split can lead to either redundant clinical reviews across all locations or location pages lacking the specificity needed for ranking and conversion.
The brand layer should manage reusable assets that scale efficiently: the clinical review board roster, medical reviewer bylines with credentials and license numbers, the editorial policy, the citation library supporting clinical claims, and disclosed ownership and funding structures, along with conflict-of-interest disclosures. These align with the trustworthiness criteria for clinical practice guidelines, emphasizing transparency, conflict-of-interest management, and rigorous evidence review 11. A single review board can attest to numerous condition pages, reducing duplicate review hours without compromising signal strength.
The location layer must retain unique, site-specific information: the state licensure number for that facility, accreditation marks specific to the physical site, payer contracts applicable to that address, the named clinical director on-site, and local patient experience signals. Federal consumer guidance explicitly states that visible contact information, site ownership, and named author credentials are what readers verify 3, 4. A prospective family researching a Tucson PHP will seek the Tucson license, not the parent company's Delaware filing.
Editorial Review Hours and Cost-Per-Qualified-Inquiry Tradeoffs
The economic implications of the brand/location split are evident in two key metrics: editorial review hours per page per quarter and cost per qualified inquiry. Centralizing the clinical review board, citation library, and reviewer attestations significantly reduces review hours per condition page, as one medical review can apply to multiple location pages.
While these savings are substantial, misapplication can be detrimental. Over-centralizing content can result in templated location pages that lack the specificity crucial for impression-to-call rates. A 2018 study on adults with serious mental illness found that provider supply, out-of-pocket cost, and insurance type were significant factors in provider choice 10—all of which are local variables that a brand-level page cannot adequately address. Consequently, cost per qualified inquiry rises when location pages fail to include location-specific payer lists, clinician names, and licensure details.
Most multi-site operators find an effective balance by having the brand manage reusable trust infrastructure (review board, citations, editorial policy, reviewer credentials) while locations retain the four critical assets that determine call qualification: the licensure block, payer list, named on-site clinical lead, and a same-day verification path. Savings from centralized brand-level review hours can then be reinvested into monthly tagging of inbound calls against the specific location pages that generated them, providing direct insight into qualified-inquiry rates.
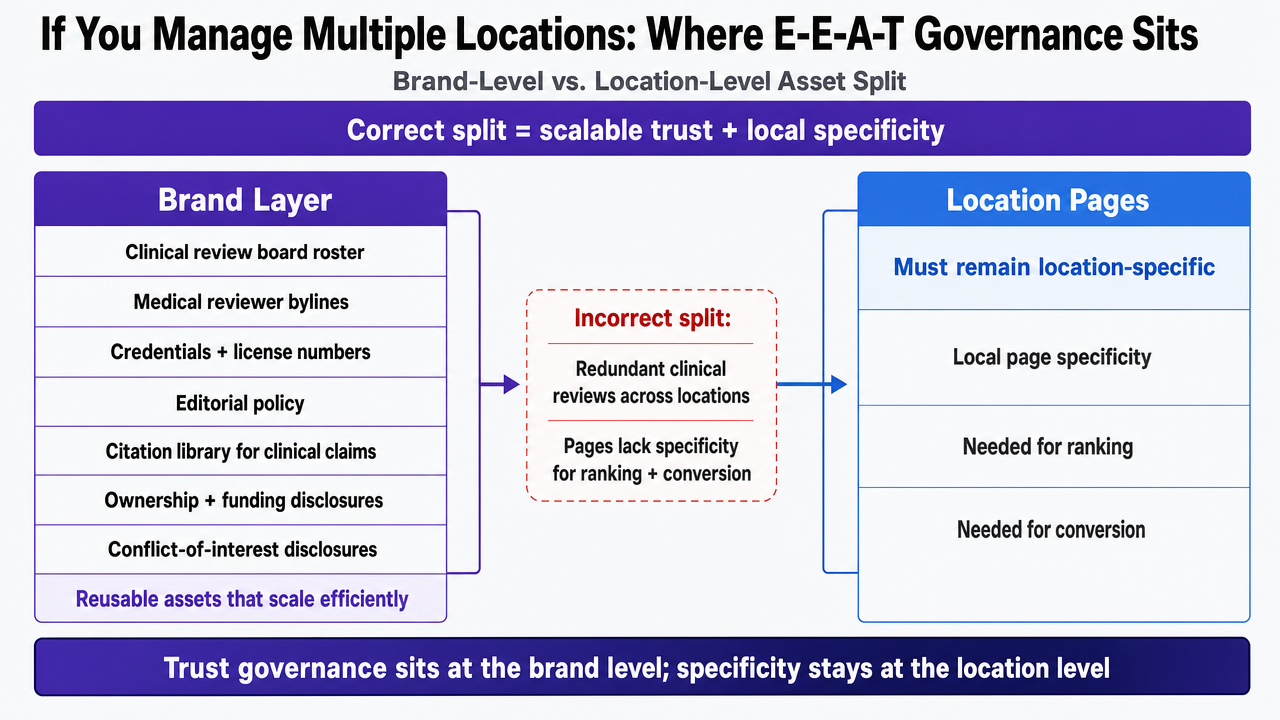 Visualize the brand-level vs. location-level asset split described explicitly in the section, showing which trust assets are centralized and which must remain local
Visualize the brand-level vs. location-level asset split described explicitly in the section, showing which trust assets are centralized and which must remain local
What to Audit on Your Site This Quarter
A quarterly E-E-A-T audit for a behavioral health site should be a focused internal effort. Gather every level-of-care page and perform six essential checks:
- Licensure Block: Verify the state license number, accreditation marks linked to issuing-body verification, and the named clinical director are visible above the fold.
- Payer List: Ensure carriers are explicitly named, with a clear same-day verification path, avoiding vague phrases like "most major insurance."
- Medical Reviewer Byline: Confirm every clinical page includes a medical reviewer byline with credentials, license number, specialty, and a review date within the past twelve months.
- Primary-Source Citations: Check for citations to primary sources (e.g., ASAM criteria, DSM-5-TR, FDA labels for MAT) for all clinical claims, aligning with consumer expectations for content review and visible sources 4.
- Ownership and Editorial Policy Pages: Confirm the operating entity, parent organization, funding, and conflict-of-interest disclosures are consistent with transparency criteria for clinical guidelines 11.
- Call-Evidence Layer: Analyze thirty days of inbound calls, tagged by qualified-versus-unqualified, payer mentioned, and level of care requested. Map each disqualification reason back to the specific page that generated the call.
The audit's output will be a prioritized list of edits, focusing on pages generating the most unqualified inquiries. Addressing these first can lead to a significant increase in intake yield on the same media spend, paying for the audit within one billing cycle.
Frequently Asked Questions
References
- 1.Consumer Assessment of Healthcare Providers & Systems (CAHPS).
- 2.HCAHPS: Patients' Perspectives of Care Survey - CMS.
- 3.Evaluating Health Information - MedlinePlus.
- 4.Online health information - what can you trust? - MedlinePlus.
- 5.Where Do Americans Get Health Information, and What Do They Trust?.
- 6.Person-Centered Preventive Healthcare: Gathering Stakeholder ....
- 7.AHRQ Projects Funded by the Patient-Centered Outcomes Research Trust Fund.
- 8.Provider choice and use of mental health care.
- 9.Choosing a Provider: What Factors Matter Most to Consumers and Patients?.
- 10.Factors that Affect Choice of Mental Health Provider and Accommodations Among Adults with Serious Mental Illness.
- 11.How to recognize a trustworthy clinical practice guideline.
- 12.Questioning reliability assessments of health information on social media.