
Key Takeaways
- Portal-linked education converts lab views into follow-up bookings by pairing plain-language result explainers with direct scheduling links at high-intent moments.
- Plain-language production standards set a quality floor, since only 2.1% of patient materials meet the AMA's sixth-grade target, blocking patient action.
- SMS and reminder sequences should function as content surfaces with versioned, service-line templates measured by kept-appointment rates, not delivery rates.
- Email recruitment for service-line launches works when lists are segmented, subject lines tested by segment, and each send drives one specific behavior.
- Secure messaging journeys compress the path to a booked visit by routing structured questions to templated replies with embedded scheduling links.
- Social content built for evidence cites sources, names clinicians, and links to portal-hosted explainers, with governance preventing misinformation risk.
- Shared decision-making assets lift conversion on high-consideration services by equipping patients with comparison docs, recovery videos, and question prompt lists for consults.
- Condition-specific education tied to refill, lab, and visit behaviors outperforms generic disease overviews because each asset triggers on an observable patient action.
- Patient story content requires literacy calibration to a sixth-to-eighth-grade level and explicit consent scope covering channels, time frame, and edited formats.
- AI marketing operating systems serve as the execution layer, routing assets through a single approval queue while preserving clinical sign-off across locations.
- Consolidating execution is the eleventh play for multi-location operators, replacing fragmented per-region production with one library, one approval queue, and one audit.
- Measuring the plays against patient behaviors—bookings, kept appointments, consult-to-surgery rates—separates content libraries that drive growth from those that merely exist.
Why most healthcare content libraries underperform on patient acquisition
Most multi-location healthcare content libraries prioritize compliance over patient growth. They often present clinical information in a format that is legally approved but lacks engagement, resulting in inconsistent conversion rates. There's often no clear link between a content asset and a patient's subsequent actions.
A significant factor in this underperformance is the readability gap. A study of 2,585 patient education materials from prominent medical journals revealed that only 2.1% met the American Medical Association's recommended sixth-grade reading level. This, combined with varying eHealth literacy levels among patients, means that the audience reaching service-line pages may struggle to act on the information provided.
The following strategies focus on documented patient behaviors—such as portal logins, lab-result views, refill clicks, and appointment adherence—rather than just content channels. Each strategy connects a content asset to a measurable action, with the final section addressing how VPs managing multiple locations can consolidate execution.
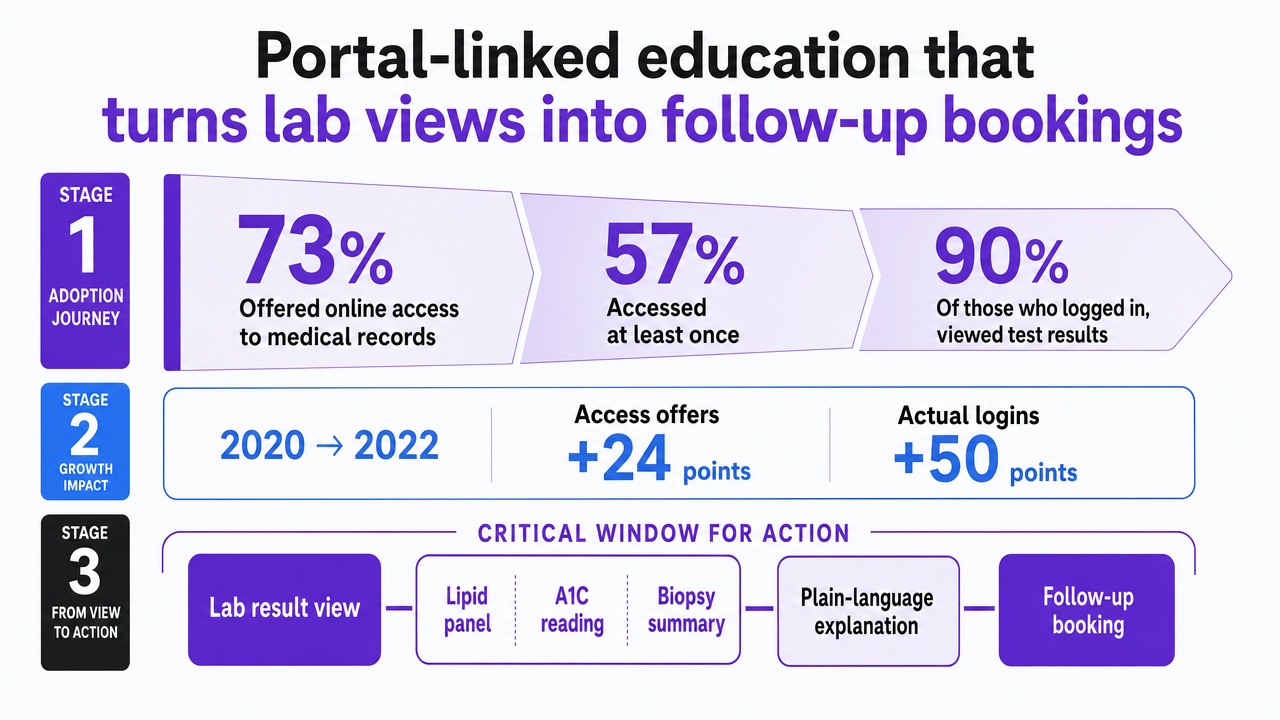
Portal-linked education that turns lab views into follow-up bookings
Patient portals represent a significant, yet often underutilized, content opportunity in healthcare. A 2022 national survey indicated that 73% of individuals were offered online access to their medical records, with 57% accessing them at least once that year. Of those who logged in, 90% used the portal to view test results. This trend shows a substantial increase in portal engagement between 2020 and 2022, with access offers rising by 24 points and actual logins by 50 points.
The moment a patient views a lab result is a critical window for action. Whether it's a lipid panel, A1C reading, or biopsy summary, this moment can be leveraged to convert curiosity into a booked follow-up. Instead of just presenting raw numbers, a growth-oriented approach pairs each common result type with a concise, plain-language explanation and a direct link to schedule an appointment with the relevant specialist.
Research on patients with HIV found that viewing labs in the portal was positively associated with viral load suppression, and that tools for refills and appointment viewing correlated with antiretroviral therapy adherence. This suggests that when educational content is strategically placed alongside high-intent portal actions, it can effectively influence patient behavior.
For marketing leaders, this requires treating result-release events as triggers within a content map. These should be linked to specific service lines, managed by marketing rather than IT, and measured by the number of downstream bookings they generate.
 Visualize the portal adoption statistics cited in this section that establish the addressable digital audience for portal-linked content
Visualize the portal adoption statistics cited in this section that establish the addressable digital audience for portal-linked content
Plain-language production standards as the quality floor
A primary determinant of whether a patient acts on content is its readability. A study examining 2,585 patient education materials from high-impact medical journals found that only 2.1% met the American Medical Association's sixth-grade reading target, and only 8.2% met the National Institutes of Health's eighth-grade recommendation. This persistent gap highlights that clinical content production has historically been optimized for the wrong audience.
Effective content for patient growth demands different production standards than content solely for compliance. The CDC's eHealth literacy synthesis identifies a skills gap among patients, noting that many adults struggle to evaluate online health information or apply it to decisions. This widespread issue should inform all content briefs. The federal Health Literacy Online guide provides practical rules: use plain language, chunk information, design for mobile-first, and conduct user testing with the target population before publishing.
For a VP of Marketing, the practical step is to establish a measurable readability standard at the production-system level. This involves three key rules: first, all patient-facing content must be at or below an eighth-grade Flesch-Kincaid score, with a sixth-grade requirement for any landing page prompting a booking. Second, content should be structured into three- to five-sentence blocks, with one key decision per block, as dense paragraphs hinder comprehension more than complex vocabulary. Third, every asset must undergo a quarterly readability audit to prevent gradual decline in clarity across the content library.
SMS and reminder sequences as content surfaces, not just nudges
Reminders are an underutilized content channel in healthcare. A systematic review of appointment reminder systems found that while reminders consistently reduce no-shows, their effectiveness can be further optimized through better timing, modality, and message content. This suggests the channel works even with generic messaging.
The strategic approach is to view each reminder as a content opportunity, not just a transactional ping. For example, a three-message sequence for a cardiology consult could include:
- a 72-hour reminder explaining the visit's purpose and what to bring,
- a 24-hour reminder linking to a short prep video, and
- a same-day message with parking and check-in details.
Each message aims to reduce a specific friction point—like incorrect forms or unclear location—that could lead to a no-show.
Marketing should manage the message library, not just the scheduling platform. This entails creating versioned templates per service line, tested for reading level, and routed through the same approval process as other patient-facing assets. The key metric to track is the kept-appointment rate for each template variant, rather than just delivery rates.
Email recruitment mechanics for service-line launches and screening pushes
Email remains an effective tool for driving patient appointments when lists are segmented and offers are specific. A 2025 study on an email-based recruitment campaign in primary care demonstrated measurable yield from a single send, with engagement influenced by list selection, subject line, and personalization. These mechanics are directly applicable to screening campaigns, new location launches, and service-line introductions, though the study focused on a single health system.
Many health systems err by sending a single mass email per service line and judging its success solely by open rates. A successful campaign, such as one designed to fill a colonoscopy schedule or a new sleep clinic, requires a different approach. It involves segmenting by age and prior visit history, leading with a personalized reason for the recipient's qualification, and linking directly to a single-page booking flow instead of a generic service description. Subject-line tests should be conducted in parallel by segment, as what resonates with a 55-year-old eligible for screening will differ from what appeals to a 32-year-old with a recent OB visit.
For VPs managing screening campaigns across regions, the principle is "one email, one behavior." A mammography campaign should focus solely on booking. A new orthopedic location launch might aim for a "save for later" action or a referral acknowledgment. Combining multiple calls to action in a single email dilutes the message and complicates post-campaign analysis.
Test AI-Driven Healthcare Content Execution Free
Experience producing and publishing real healthcare content with measurable results before making a commitment.
Secure messaging journeys that compress the path to a booked visit
Secure messaging is a highly valuable portal feature that marketing often overlooks. A study of portal messaging among patients with chronic conditions found that patients use messages when they perceive a clear advantage over traditional methods like calling or visiting the clinic. This indicates that message volume reflects the ease of the digital path compared to the analog one. Content integrated within the messaging interface can leverage this preference.
The strategy involves creating concise, branching message journeys that guide a patient from a clinical question to a booked visit without leaving the portal. For instance, a post-visit message could ask two structured questions, route the answers to a templated reply with an embedded scheduling link, and conclude with a brief care instruction. This approach is more effective than a lengthy follow-up email. Specialty groups can pre-stage these message threads for specific procedures, such as post-op orthopedic check-ins, dermatology lesion follow-ups, or behavioral health prompts between sessions.
The HIV portal cohort study showed that the use of secure messaging tools, along with refill and appointment-viewing activity, correlated with antiretroviral adherence. While this population is specific, the underlying pattern—structured digital touchpoints reducing the steps between intent and action—is a valuable model for any service line where the next visit is a key growth metric.
Social content built for evidence, not impressions
While social channels reward consistent activity, reach metrics rarely translate directly into booked visits. A review of patient education via social media indicated that platforms like Facebook, YouTube, and Twitter can enhance health knowledge and reinforce behaviors when content is evidence-based and actively moderated. However, the same review highlighted misinformation and privacy risks as central threats to trust in health brands. A broader systematic review identified ten distinct uses for social media in health, from promotion to peer support, concluding that effects on knowledge and behavior are real but varied, with study quality differing significantly.
For multi-location operators, this means shifting the focus from social impressions to two more critical questions: did the post guide a specific audience toward a screening, second opinion, or service-line page, and did it pass clinical review without being diluted? The most effective posts cite sources, name clinicians, and link to portal-hosted explainers that support the claims. Conversely, generic stock graphics with awareness-month hashtags are less impactful.
Governance is a significant cost factor. Regional marketers cannot make independent medical claims, and central marketing cannot become a bottleneck for every post. A shared evidence library, pre-approved talking points by service line, and a single approval queue enable social media to operate at the speed of the news cycle while mitigating the risk of misinformation.
Shared decision-making assets that lift conversion on high-consideration services
High-consideration services—such as joint replacement, bariatric surgery, fertility treatments, oncology second opinions, and spine procedures—rarely convert on the initial page visit. Patients considering these services weigh risks, recovery, and costs, often discussing these factors with family, a process marketing typically doesn't observe. Shared decision-making assets are designed to support these crucial conversations.
A review on patient education and health literacy concluded that efficient, patient-centered education significantly supports shared decision-making and subsequent adherence. The AHRQ systematic review on health literacy interventions further emphasized that multi-modal education—including text, video, and structured comparison tools—improves understanding and decision quality across diverse literacy levels. For a content portfolio, this translates to three types of assets per high-consideration service line:
- a risk-and-benefit comparison document for family discussions,
- a recovery-timeline video under three minutes, and
- a list of questions for patients to bring to their consult.
The key conversion mechanism here is the question list. When patients arrive at a consult with pre-written questions, the visit is more likely to convert because the clinician can directly address their specific concerns. Marketing should track which decision aids precede a booked surgery, rather than focusing solely on pageviews.
Condition-specific education tied to refill, lab, and visit behaviors
Generic disease overviews are often ineffective because they fail to account for the patient's current stage in the care cycle. A patient refilling metformin requires different content than one whose A1C result just arrived in the portal, and both need something distinct from a newly diagnosed patient seeking an explanation. Condition-specific education is effective when each asset is linked to an observable patient behavior.
A review of digital health technologies for patient education found that structured programs combining education, coaching, and tracking improved knowledge and self-management skills for chronic conditions. The strongest effects were observed when content was directly tied to the behaviors it aimed to influence, rather than being delivered as standalone reading. The HIV portal cohort study reinforced this pattern: refill clicks, secure messages, and lab views correlated with antiretroviral adherence and viral load suppression when content was presented alongside these actions.
For a diabetes program, this means developing three distinct asset tracks instead of a single library:
- Refill events could trigger a brief adherence prompt and a side-effect FAQ.
- New A1C results could trigger a result-specific explainer with a direct link to a diabetes educator.
- Annual visit reminders could include a question prompt list tailored to the patient's last lab results.
Marketing should map these tracks for each service line and measure each asset's effectiveness against the specific downstream behavior it was designed to influence, rather than against pageviews.
Patient story content with literacy and privacy guardrails
Patient stories often resonate more than generic service-line copy because they address the fundamental question prospective patients ask: "Did someone like me achieve a positive outcome here?" A systematic review of social media use for health identified peer support and patient narratives as effective tools for influencing knowledge and behavior. However, it also highlighted concerns about study quality and the persistent risk of misinformation when narratives deviate from evidence.
Two critical guardrails distinguish effective patient story content from potential liability. First, literacy calibration is essential: stories should adhere to the same sixth-to-eighth-grade reading level as other patient-facing assets. This involves simplifying clinical jargon in quotes without misrepresenting the patient's words. Second, consent scope must be clearly defined. A written release should specify the channels, time frame, and whether the story can be edited into shorter formats for SMS or social media. A patient who agrees to a website testimonial may not consent to its use in a paid advertisement.
Marketing should measure the success of patient stories by their correlation with booked consults in the same service line, rather than by emotional impact alone.
Centralize Content Marketing Execution for Consistent Patient Acquisition
See how leading healthcare marketing teams use unified AI-driven workflows to streamline content, PPC, and SEO across all locations—reducing manual coordination and accelerating measurable patient growth.
AI marketing operating systems as the execution layer
The preceding strategies outline what content to produce. This section addresses the systems that manage their execution. Portal-linked result explainers, SMS sequences, segmented email pushes, secure messaging journeys, decision aids, condition-specific tracks, and consented patient stories are not isolated campaigns. They form a cohesive content portfolio that must be deployed, versioned, and measured against patient behaviors across all locations on a consistent schedule.
This is where many healthcare marketing teams encounter challenges, particularly those managing around 20 locations. Briefing cycles become extended, regional marketers duplicate assets already present in the central library, and readability standards may decline due to a lack of centralized auditing. AI marketing operating systems streamline this process into a governed loop. Specialist strategists develop content based on the source library, route every asset through a single approval queue, and deploy approved content across portals, SMS, email, and social media, with citations and reading levels attached to each record.
This category includes platforms specifically designed for multi-location service verticals, such as Vectoron, which coordinates content, SEO, PPC, and backlink execution under account-level approval, eliminating per-location handoffs. The key test for any such system is its ability to maintain clinical sign-off while significantly reducing the production overhead that currently limits the scope of marketing initiatives.
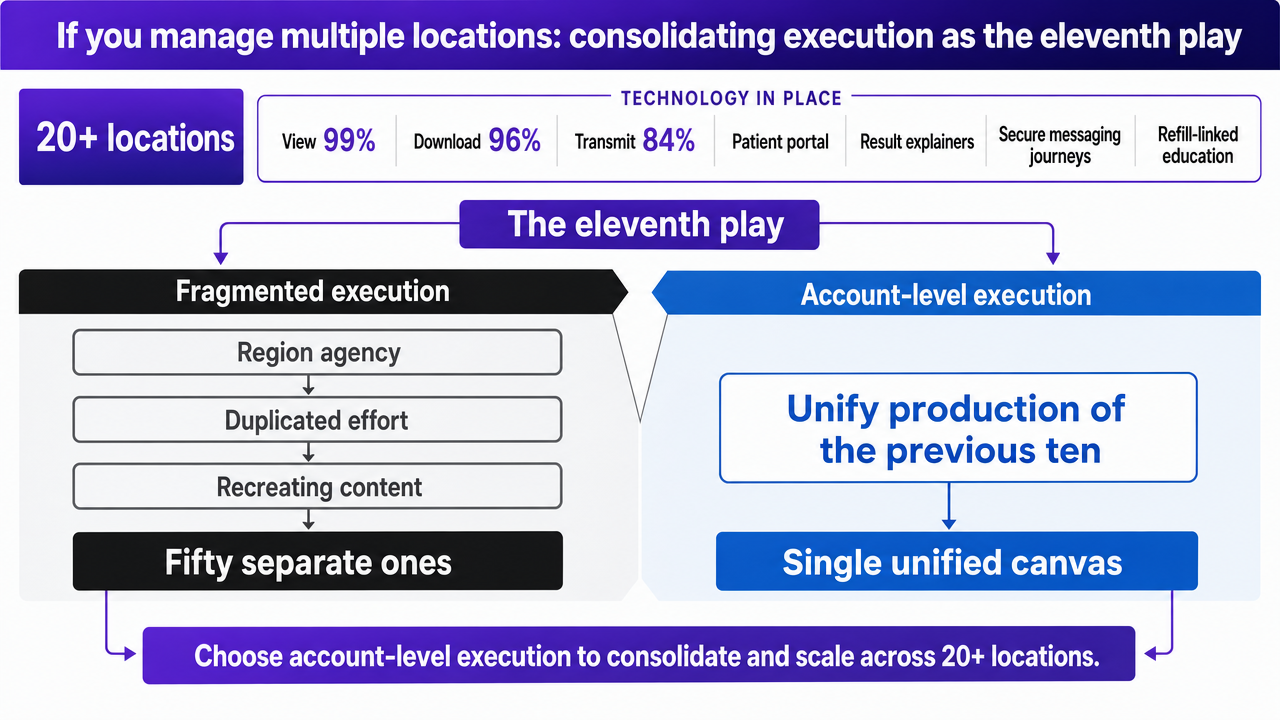
If you manage multiple locations: consolidating execution as the eleventh play
For health systems operating 20 or more locations, the eleventh strategy isn't another content type, but rather the decision to unify the production of the preceding ten strategies. The technological infrastructure is already in place: by 2024, 99% of U.S. hospitals supported electronic viewing of patient health information, 96% supported download, and 84% supported transmission, according to federal data. The patient portal, which hosts result explainers, secure messaging journeys, and refill-linked education, is virtually universal. The challenge lies in whether marketing teams treat it as a single, unified canvas or as fifty separate ones.
Fragmented execution manifests consistently across multi-location operators. Each region may engage its own agency, leading to duplicated efforts, such as recreating a diabetes explainer that already exists in the central library. Compliance reviews the same asset multiple times under different brand variations. Readability standards often drift because no single entity audits the entire catalog quarterly. Consequently, by the time a screening campaign reaches patients, different locations may be using outdated or inconsistent versions of the same content.
Account-level execution reverses this fragmentation. It involves a single source library, one approval queue, and a set of versioned templates syndicated to local pages with location-specific provider names, hours, and booking flows. Clinical sign-off occurs once per asset, not once per market. Readability audits are conducted on the entire library, rather than on thousands of disparate pages. This approach allows regional marketers to focus on localization, their primary role, instead of content production.
The effectiveness of any consolidation effort is measured by its ability to preserve clinical control while eliminating redundant production. For example, if a system with 40 locations briefs 6 assets monthly, that amounts to 240 briefing cycles. By centralizing the briefing process, the same content calendar can be managed with significantly reduced coordination, while maintaining consistent governance for each asset record.
 Visualize the comparison framework between fragmented and account-level content execution described in this section's variables-only comparison
Visualize the comparison framework between fragmented and account-level content execution described in this section's variables-only comparison
Fragmented vs. account-level content execution: a variables-only comparison
For multi-location operators considering consolidation, the benefits are quantifiable in terms of operational variables. Let L represent locations, A represent assets produced per location per month, and R represent compliance review cycles per asset. Fragmented execution costs scale approximately as L × A × R, plus the additional cost of duplicate creative production when the same content is rebuilt across multiple regions.
| Variable | Fragmented execution | Account-level execution |
|---|---|---|
| Brief cycles per month | L × A | A (one library) |
| Clinical sign-offs per asset | L × R | R (once per asset) |
| Readability audits | Per-location, often skipped | One quarterly catalog audit |
| Regional marketer role | Producing | Localizing |
The primary savings from this consolidation are realized through reclaimed coordination hours and a consistent readability standard, rather than direct line-item discounts.
Measuring the eleven plays against patient behaviors that matter
The true measure of a healthcare content portfolio's success is not impressions, sessions, or open rates, but rather the count of specific patient actions that lead to a booked or kept visit. Each of the eleven strategies outlined maps to a primary behavior and a designated owner.
- For portal-linked education, the key metric is follow-up bookings within seven days of a result view.
- For SMS sequences, it's the kept-appointment rate per template variant, not just delivery rate.
- For email pushes, it's the segment-level booking yield per send.
- For secure messaging journeys, it's the proportion of threads that conclude with a booked visit.
- For decision aids, it's the consult-to-surgery rate among patients who downloaded the question prompt list.
Marketing leaders should maintain a single, weekly updated dashboard that links every asset in the library to its target behavior and current conversion rate. Assets that consistently fall short of their target rate for two consecutive quarters should be retired or revised. This disciplined approach is what differentiates a content library that actively drives system growth from one that merely exists.
 Individuals offered online access to medical records (2022)
Individuals offered online access to medical records (2022)
Individuals offered online access to medical records (2022)
Frequently Asked Questions
References
- 1.Utilizing Digital Health Technologies for Patient Education and Self-Management.
- 2.Patient Education and Engagement through Social Media.
- 3.Social Media Use for Health Purposes: Systematic Review.
- 4.Individuals' Access and Use of Patient Portals and Smartphone Health Apps: 2022.
- 5.Relationship Between Patient Portal Tool Use and Medication Adherence and HIV Outcomes.
- 6.eHealth Literacy.
- 7.Health Literacy Online: A Guide for Simplifying the User Experience.
- 8.Design and Performance of an Email-Based Patient Recruitment Campaign.
- 9.An Assessment of Patient Portal Messaging Use by Patients With Chronic Conditions.
- 10.Growth of Health IT-Enabled Patient Engagement Capabilities Among U.S. Hospitals, 2021–2024.
- 11.Empowering Patients: Promoting Patient Education and Health Literacy.
- 12.Health Literacy Interventions and Outcomes: An Updated Systematic Review.
- 13.Readability of Patient Education Materials From High-Impact Medical Journals.
- 14.Appointment reminder systems are effective but not optimal: results of a systematic review and evidence-based recommendations.
- 15.Text Message Reminders Increase Appointment Adherence in a Pediatric Clinic: A Randomized Controlled Trial.