
Key Takeaways
- Scaling local SEO across a multi-location portfolio is a governance and data-systems problem first; inconsistency between website, GBP, citations, and schema is the dominant failure mode, not weak tactics.
- Patient choice turns on four observable, location-level attributes—distance, waiting time, provider qualification, and cost—so landing pages and GBPs should be assembled from modules that answer each one 6.
- A five-layer operating system—data, content, signal, governance, and measurement—routes every location through one source-of-truth record, with HIPAA and FTC checks built into the publishing queue rather than reviewed after the fact 8, 10.
- Report qualified calls per location per week segmented by drive-time, and tier locations by access context so underserved rural markets get deeper transparency modules while saturated metros get sharper differentiation copy 11, 7.
Forty Profiles, One Team, Inconsistent Signals
A DSO running 40 Google Business Profiles with a four-person marketing team faces a predictable pattern: a handful of flagship locations rank in the local pack, a middle tier drifts, and a long tail bleeds qualified calls to competitors whose only advantage is a fresher post cadence and faster review responses. The team is not under-skilled. It is under-systematized.
Inconsistency is the real failure mode. Hours are correct on one profile and stale on three. A new service line is published on the website but missing from 22 GBP service items. Review responses arrive within an hour at the home market and three days everywhere else. Schema fires on some location pages and silently breaks on others after a template update.
Patient choice does not forgive that drift. Discrete-choice research on dental care preferences shows distance, waiting time, dentist qualification, and cost all carry significant weight when a prospective patient picks a provider 6. Those signals live at the location level, not the brand level. Scaling Google local SEO across 20, 50, or 500 practices is therefore a governance and data-systems problem first, and a tactics problem second. The rest of this article treats it that way.
Patient Choice Drivers Define the Optimization Target
What Patients Actually Weigh: Distance, Wait Time, Qualification, Cost
Most local SEO playbooks optimize for what crawlers read. Patients optimize for something else entirely. A 2023 discrete choice experiment on preferences for preventive dental care found that waiting time, dentist qualification, cost, and clinic distance each carried statistically significant weight in how respondents chose a provider 6. The study sampled a Saudi adult population, so the absolute coefficients do not transfer cleanly to a US DSO catchment, but the structure of the decision—four observable, location-level attributes—maps directly to what a location landing page and a Google Business Profile can communicate.
That mapping is the operational point. Each of the four attributes corresponds to a content element the marketing team already controls:
- Clinic distance. Address precision, neighborhood and landmark references, embedded map, parking and transit notes, and accurate service-area definitions in GBP.
- Waiting time. Same-week or same-day availability copy, average wait disclosures where defensible, real-time booking widgets, and GBP appointment links.
- Dentist qualification. Named providers per location with credentials, residency, specialty focus, languages spoken, and per-provider schema rather than a single brand-level About page.
- Cost. Insurance accepted by location, membership plan pricing, financing options, and transparent ranges for common procedures.
None of those elements rank a page by themselves. Together they answer the four questions the research says a prospective patient is actually weighing before clicking the call button. A keyword tool will not surface this content schema because it is not a keyword problem. It is a patient-preference problem that GBP and the location landing page are the closest digital proxies for. Sections later in this article treat each as a module to be templated once and approved centrally.
Why Proximity Beats Keyword Density at the Location Level
Distance is not just one attribute among four. It dominates the others in healthcare contexts. A systematic review of UK studies on travel time and health outcomes found that 77% of included studies showed a distance-decay association: as travel distance increased, access and outcomes generally worsened 12. The review covered adult populations in the United Kingdom and noted inconsistent travel-time methodologies across studies, so the percentage describes the direction of evidence rather than a precise US effect size. The signal is still hard to ignore for a DSO planning content priorities across a 40-location footprint.
The implication for local SEO is structural. A location page that ranks in the three-pack but buries hours, ZIP-level service area, parking guidance, and route-from-major-corridor copy underperforms a page two positions lower that surfaces those signals above the fold. Proximity is communicated, not just measured. Patients triangulate it from address, neighborhood markers, drive-time references, and the absence of friction in scheduling.
This reframes the optimization target. Aggregate keyword rank across a portfolio is a lagging, noisy metric. Qualified calls per location, segmented by whether the caller is inside a defensible drive-time radius, is the variable that compounds. Content investments that improve convenience signals on a location page tend to lift both rank and call quality at the same time, because Google and the patient are looking for the same thing: evidence that this specific practice is actually convenient for this specific searcher. Keyword density does not produce that evidence. Location-specific operational detail does.
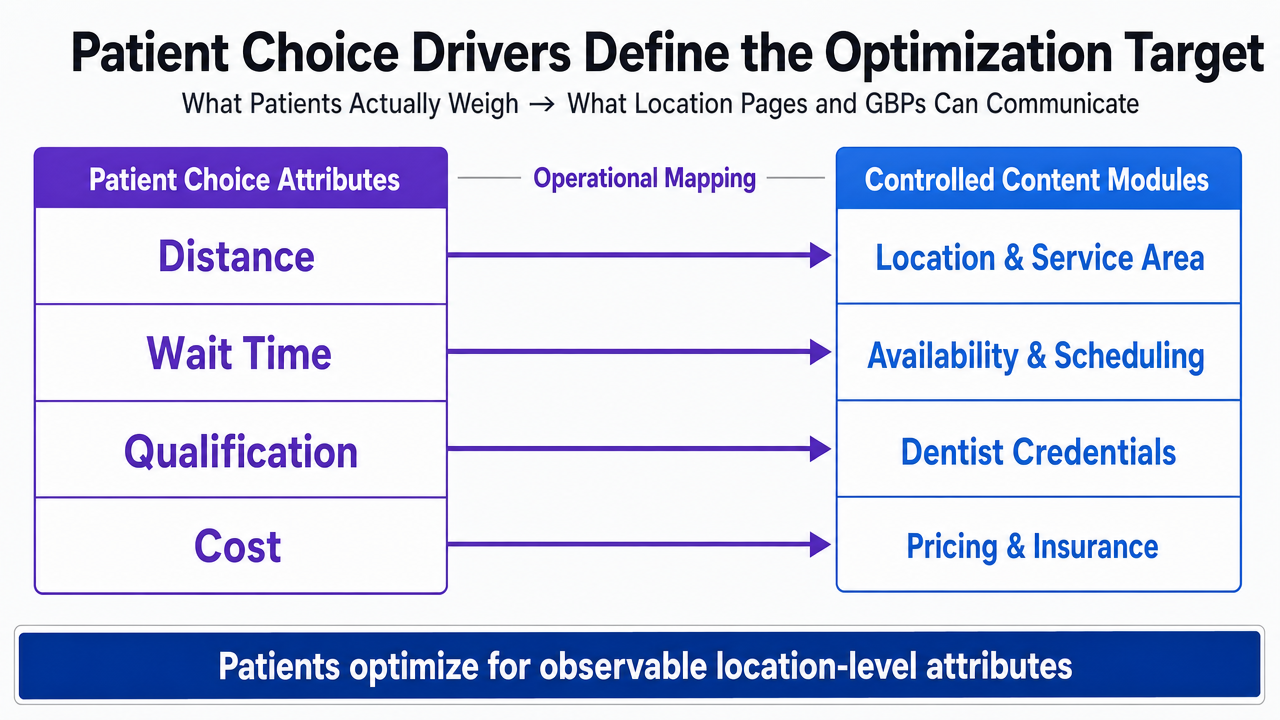 Visualize the four patient-choice attributes from the discrete choice study and map each to a corresponding content module on location pages and GBPs
Visualize the four patient-choice attributes from the discrete choice study and map each to a corresponding content module on location pages and GBPs
A Five-Layer Operating System for Multi-Location Local SEO
Data Layer: Location Records as the Source of Truth
Before any content ships, the portfolio needs a single, authoritative location record per practice. Not a spreadsheet that the SEO vendor maintains separately from the operations roster. Not a GBP export that drifts from the website footer. One record, owned by the marketing team, treated as the upstream source for the website, GBP, citation aggregators, schema markup, and call-tracking provisioning.
The CDC's NHSN manual offers a useful structural analogy. It instructs facilities to define both physical locations and virtual locations—splitting a single physical unit into multiple logical units when surveillance criteria differ 5. The intent is infection tracking, not marketing, but the data discipline transfers directly. A DSO often has one street address hosting a general practice and an orthodontic specialty, or a satellite office that operates only on Thursdays, or two providers sharing a suite under different brand names. Each needs its own record with explicit fields, not an implicit assumption that one address equals one node.
The minimum schema per location: legal name, public-facing name, address normalized to USPS format, geocoordinates, phone with tracking-number overlay, fax, primary and secondary categories, services offered, accepted insurance plans, languages spoken, named providers with NPI, hours by day including holiday exceptions, accessibility attributes, and the parent brand identifier. Every downstream system reads from this record. When a location adds Saturday hours, the data layer updates once and propagates. When it doesn't, the inconsistency surfaces in a daily reconciliation report instead of in a patient complaint three weeks later.
Content Layer: Landing Page Modules and GBP Service Items
The content layer converts the data record into the artifacts patients actually see: a location landing page and a Google Business Profile. Both should be assembled from templated modules, not authored from scratch per practice. Templating is what makes the four patient-choice attributes—distance, wait time, qualification, cost—answerable everywhere at once 6.
A defensible landing page template carries roughly a dozen modules, each populated from the data layer or a per-location override:
- Hero with location name, address, and primary phone mirroring the GBP exactly.
- Drive-time and route block referencing the nearest major corridor and a parking or transit note.
- Hours module including same-week availability copy and an appointment link tied to the booking system.
- Provider cards with named clinicians, credentials, residency, specialty, and languages spoken—each with Person schema.
- Services offered mapped one-to-one with GBP service items and Service schema, not a generic services menu.
- Insurance and payment module listing accepted plans and membership options for that specific practice.
- Accessibility and transportation details addressing the access barriers documented in oral health disparities research 3.
- Reviews module pulling location-scoped reviews with structured response history.
- FAQ block answering location-specific questions, not brand-wide ones.
- LocalBusiness and DentistOffice schema with sameAs pointing to that location's GBP CID URL.
GBP service items mirror the landing page service list field for field. When the website adds clear aligners to a location's service menu, the GBP service item for clear aligners is created in the same workflow, with the same description, the same price range disclosure, and the same internal taxonomy ID. Drift between website services and GBP services is the most common silent failure across multi-location portfolios, and it costs ranking visibility on category-level queries because the entities Google sees do not agree with each other.
Signal Layer: Reviews, Citations, and Call Intelligence
Signals are what Google and patients use to rank trust. The signal layer governs three flows: review velocity and response, citation consistency, and call tracking that closes the loop on conversion quality.
Review operations run on per-location SLAs, not a brand-wide average. A workable standard is response within 24 business hours, escalation paths for one- and two-star reviews routed to the location's clinical lead, and a templated response library that follows HHS guidance on PHI—meaning no acknowledgment of treatment, no diagnosis confirmation, and no patient identifier in a public reply absent written authorization 8. A response that says "thank you for being our patient" has already disclosed PHI to a public audience. The template library should make that mistake structurally impossible.
Citations are a maintenance function, not a campaign. The data layer feeds primary aggregators and the top 30 to 50 directories per market. The exception list—directories that refuse to update, niche dental directories with regional reach, hospital affiliation sites—gets manual reconciliation quarterly. Citation accuracy is binary: either every record matches the data layer or it doesn't.
Call intelligence ties the signal layer to revenue. Each location gets its own tracking number pool, a routing rule that preserves the published number on the GBP for ranking purposes, and call scoring that classifies inbound calls as new patient, existing patient, billing, or non-patient. Without that classification, every location reports calls; only some report qualified calls. The measurement layer below depends on this distinction.
Measurement Layer: Qualified Calls per Location, Not Aggregate Rank
Aggregate keyword rank across a 40-location portfolio is a metric that hides more than it reveals. A brand can lift average position by two spots while losing qualified calls in eight markets, because rank moves on commodity queries while the four locations that matter to the quarter are flat on commercial intent terms. The measurement layer should report at the location-and-intent grain.
Three reports do most of the work:
- Qualified calls per location per week, segmented by new patient versus existing, with caller drive-time bucketed against the practice's defensible radius.
- Conversion rate from GBP profile views and website sessions to qualified call, by location, with a four-week trailing comparison.
- Coverage report showing the percentage of priority queries—branded, category, and service-modifier—where the location appears in the three-pack and on page one organically.
Rank is included, but as a diagnostic input to call volume, not as the headline. When a location's qualified calls drop, the rank report explains whether the cause is visibility loss or conversion loss on the landing page. That distinction routes the fix to the content layer or the signal layer instead of to a generic "do more SEO" directive that wastes a sprint.
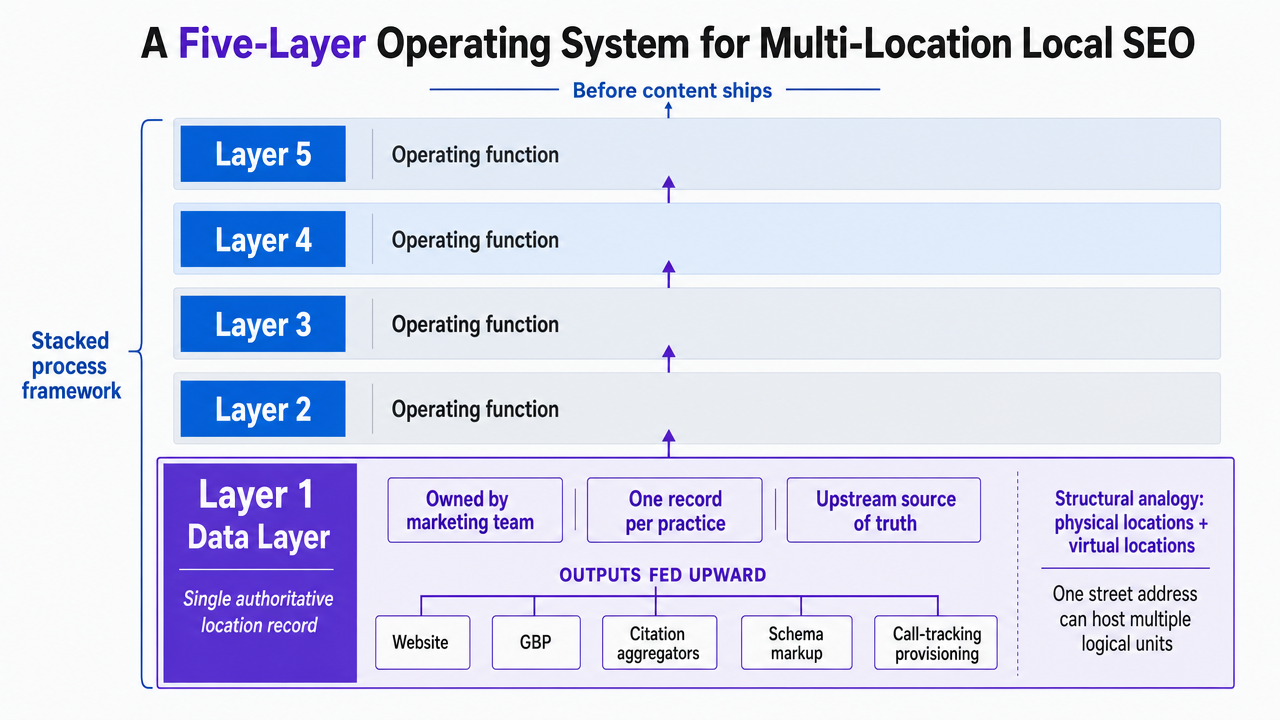 Visualize the five-layer operating system described in the section as a stacked process framework with each layer's function
Visualize the five-layer operating system described in the section as a stacked process framework with each layer's function
Test multi-location SEO execution in real time
Experience unified Google Local SEO workflows live across all your locations before making a commitment.
Governance and Substantiation as Workflow, Not Appendix
Compliance fails when it lives at the end of a process. The pattern is familiar: a location landing page goes live with a claim like "the area's most experienced implant team," a GBP post promotes "95% patient satisfaction," and a review response thanks a named patient for completing their root canal. Legal sees none of it until something surfaces. The fix is structural, not educational—governance has to be a gate inside the publishing workflow, not a memo circulated after the fact.
Two regulatory regimes set the design constraints. The FTC requires that advertising be truthful, not misleading, and supported by a reasonable basis of objective evidence for any express or implied claim, with the level of substantiation scaled to the nature of the claim 1, 9, 10. HIPAA, as interpreted by HHS, requires written patient authorization before protected health information is used for marketing, with narrow exceptions 8. Both rules apply identically across every location, which is precisely what makes them suited to centralized enforcement.
A workable governance gate has four components built into the same approval queue that pushes content live:
- Claim register. Every superlative, percentage, outcome figure, and comparative phrase used on location pages, GBP posts, or review responses is logged against its supporting evidence. "Most experienced" requires a defined metric and a current source. Without one, the claim does not ship.
- PHI filter on review responses. Templates strip any acknowledgment of treatment, diagnosis, or identifying detail. A response confirms the brand cares about feedback; it never confirms the reviewer is a patient 8.
- Per-location scope check. A claim approved for one practice does not auto-propagate. Provider credentials, accepted insurance, and outcome figures are location-bound and must clear the data layer before appearing anywhere they apply.
- Versioned audit trail. Every published asset carries its approver, evidence references, and publish timestamp. When the FTC standard for substantiation depends on what was known at the time of the claim 10, the audit trail is the defense.
Treating this as workflow rather than appendix changes the unit cost of compliance. The same gate that prevents a HIPAA disclosure in a Tuesday review response also prevents a substantiation gap in a Friday GBP post, across all 40 locations, without a legal review cycle per asset. That is the only model that scales.
Access Gaps Shape Which Locations Deserve Which Content
Not every location in a 40-practice portfolio earns the same content investment. The instinct is to template once and ship uniformly, but geographic context changes what a landing page has to do. The CDC has documented that geographic location remains a primary contributor to whether patients receive timely screening and treatment, with measurable metro versus nonmetro gaps in service access 11. Oral health follows the same pattern: low-income, uninsured, rural, and minority populations face compounding barriers that brand-level messaging does not address 3.
For a rural or exurban practice, the content priority shifts. A 2026 narrative review of rural healthcare access identified distance, transportation, broadband limitations, and workforce shortages as the persistent barriers, and cautioned that telehealth complements but does not substitute for local presence 7. A landing page serving that catchment needs explicit transportation guidance, ride-share or shuttle program details if available, expanded hours that reduce the number of trips required, and accepted insurance copy that surfaces Medicaid participation where applicable. Generic "convenient location" copy does no work in a market where convenience is the binding constraint.
Dense urban locations carry a different content load. Multiple providers within a short radius mean the page has to differentiate on qualification, languages spoken, same-day availability, and insurance breadth—not on proximity, which competitors match.
The operational rule is straightforward: segment locations into access tiers before assigning content cadence. Underserved markets get deeper transparency modules and higher publishing priority because the gap between what patients need to know and what is currently published is wider. Saturated metros get sharper differentiation copy and faster review-velocity targets. Aggregate publishing schedules that ignore this segmentation waste cycles on locations that already convert and starve the ones that could.
See How Enterprise DSOs Automate Local SEO Consistency Across All Locations
Request a walkthrough of unified workflows for multi-location Google Local SEO—enabling your team to manage listings, monitor ranking shifts, and centralize approvals without scaling headcount or losing oversight.
If You Manage a 25-Location Portfolio: Operating Model Economics
The scope shifts here from operating principles to a portfolio operator's build-versus-outsource-versus-platform decision. Assume a 25-practice DSO, four-person central marketing team, and the system described above—data layer, content modules, signal SLAs, governance gate, measurement at the location-and-intent grain. The question is who executes the per-location work week after week.
Three operating models cover most portfolios. Model A hires a marketing coordinator embedded at each practice. Model B keeps a small central team and contracts a traditional agency on a per-location retainer. Model C centralizes the team and runs execution through an AI marketing platform that produces GBP posts, landing page updates, review responses, and citation reconciliation under central approval. The CDC NHSN discipline of defining every node—physical and virtual—once and consistently applies regardless of which model executes the work 5. The choice is about who fills the templates, not whether the templates exist.
| Variable | Model A: Coordinator per location | Model B: Central team + agency retainers | Model C: Central team + AI execution platform |
|---|---|---|---|
| Headcount cost | 25 × $X FTE salary | 2–3 × $X FTE salary | 2–3 × $X FTE salary |
| Per-location execution cost | Included in FTE | 25 × $Y agency retainer/mo | Platform fee (reference: $599/mo trial tier) |
| GBP posts per location / month | Variable by coordinator | 2–4, agency-dependent | Centrally scheduled, uniform cadence |
| Review response SLA | Local hours only | Agency business hours | 24-hour SLA, templated under PHI filter |
| Landing page updates | Per-coordinator skill | Change-order cycle | Approval queue, same-day publish |
| Compliance audit trail | Decentralized | Per-agency contract | Versioned, centralized |
Two patterns surface as the portfolio grows past 25 nodes. Headcount scales linearly in Model A and the variance in output between coordinators widens, not narrows, because the central team cannot enforce cadence on 25 direct reports. Model B caps headcount but exposes the portfolio to agency-by-agency drift, which is the same inconsistency problem at a different layer. Model C holds headcount flat and shifts the unit of work from a person-hour to an approved artifact, which is what makes per-location output cadence comparable across the footprint.
What Changes When the System Is in Place
A DSO running the five-layer system stops debating tactics in standups. The data layer answers whether a location's hours are correct everywhere. The content layer answers whether clear aligners exist on both the website and the GBP. The signal layer reports review response time by practice, and the governance gate has already filtered the PHI risk out of the queue 8.
The headline change is what the marketing director presents to the CMO. Aggregate rank gives way to qualified calls per location per week, segmented by drive-time. Coordinator-by-coordinator output variance compresses into a uniform cadence under central approval. Substantiation is logged at publish time, not reconstructed during an FTC inquiry 10.
Vectoron operates this loop—specialist strategists producing the per-location work, the central team approving it. The system is what scales. The platform is how the team stops being the bottleneck.
 Percentage of Jordanian dentists who consider dental advertising appropriate
Percentage of Jordanian dentists who consider dental advertising appropriate
Percentage of Jordanian dentists who consider dental advertising appropriate
Frequently Asked Questions
References
- 1.Advertising and Marketing.
- 2.Medicare Marketing Guidelines.
- 3.Disparities in Access to Oral Health Care.
- 4.Evolving perspectives in dental marketing: A study of Jordanian dentists’ attitudes and practices.
- 5.CDC Locations and Descriptions and Instructions for Mapping Patient Care Locations.
- 6.Assessing Patients' Preferences for Preventive Dental Care.
- 7.Health care access from the rural perspective: A narrative review.
- 8.Marketing | HHS.gov.
- 9.Advertising FAQ's: A Guide for Small Business.
- 10.FTC Policy Statement Regarding Advertising Substantiation.
- 11.Advancing Health Equity, Eliminating Health Disparities, and Improving Population Health by Geographic Location.
- 12.Are differences in travel time or distance to healthcare for adults in the United Kingdom associated with health outcomes?.