Key Takeaways
- Backlink programs for multi-location practices fail when built clinic by clinic; authority compounds only on top of a single canonical provider data spine that feeds every citation, schema block, and outreach asset.
- Directory accuracy is the accuracy floor under every link, since CMS verification found only 29% of sampled provider records fully accurate across audited fields 6, turning link strategy into a data-governance problem.
- Patients are taught to trust government, academic medicine, hospital systems, and professional associations above commercial .com publishers 12, 13, so the authority budget belongs in those four tiers rather than in generic directories or social.
- Focus next on consolidating execution at the account level, holding refresh cadence to monthly or the Medi-Cal quarterly floor 4, and auditing on-site NAP, schema, and appointment paths so earned authority actually converts.
Why link strategy breaks at the location level
Most healthcare backlink programs are built location by location, then bolted together at the brand level. This approach is flawed. A 40-site dermatology group cannot achieve authority by purchasing citation packages for each clinic when its provider data is already inconsistent across federal directories, payer networks, and state systems. Every link points at a moving target.
The compliance baseline also continuously shifts. CMS has stated that federal and state requirements for provider directories expand annually, and provider-directory obligations now fall under broader No Surprises Act transparency rules that apply to physicians and other healthcare providers 7, 8, 1. A national directory effort highlighted in the Federal Register reinforces this issue: existing directories contain inaccurate information and are costly to maintain 2. This is not a traditional marketing problem; it is a data-governance problem that marketing inherits.
For a VP of Marketing overseeing 10 to 300 sites, the consequence is significant. Per-location agency proposals optimize the wrong unit. They price link acquisition against the clinic, while the actual asset that earns and retains trust is the provider data spine underlying every clinic. When that spine is inaccurate, even high-authority editorial coverage can misdirect patients to the wrong phone number, incorrect specialty tag, or a closed location. The subsequent sections outline how to build a link program on top of that spine, in the correct operational sequence.
The accuracy floor under every healthcare backlink
What federal auditors actually found in provider directories
The clearest empirical data on directory accuracy in U.S. healthcare comes from a CMS review of Medicare provider-directory notices from 2017 through 2021. Out of 1,215 records sampled and verified at the point of contact, only 360 records, or 29%, contained fully accurate data across all audited fields 6. This figure should inform a multi-location operator's understanding of the gap between policy and reality.
The scope of this audit is important. The CMS sample was drawn from Medicare plan-year directory notices, not the public web. Verification involved point-in-time outbound contact against documented fields, not a continuous audit. The 29% figure represents fully accurate records; a single incorrect digit in a phone number or an outdated specialty tag rendered a record inaccurate. This narrow methodology suggests that the underlying error rate across the broader directory ecosystem, including state Medicaid systems, commercial payer directories, and Google Business Profiles, is likely no better.
Two patterns emerge from the audit. First, common errors are not complex; they involve phone numbers, addresses, specialties, and acceptance status—the same fields a backlink uses to target a location page. Second, this data does not self-correct. The Federal Register notice on a national directory effort describes directories as widely inaccurate and expensive to maintain, framing the accuracy problem as systemic 2. For a VP of Marketing, this changes the link conversation. Earned authority routes patients through the existing data layer at the moment of click. If that layer is wrong 70% of the time, the link isn't failing; the data is.
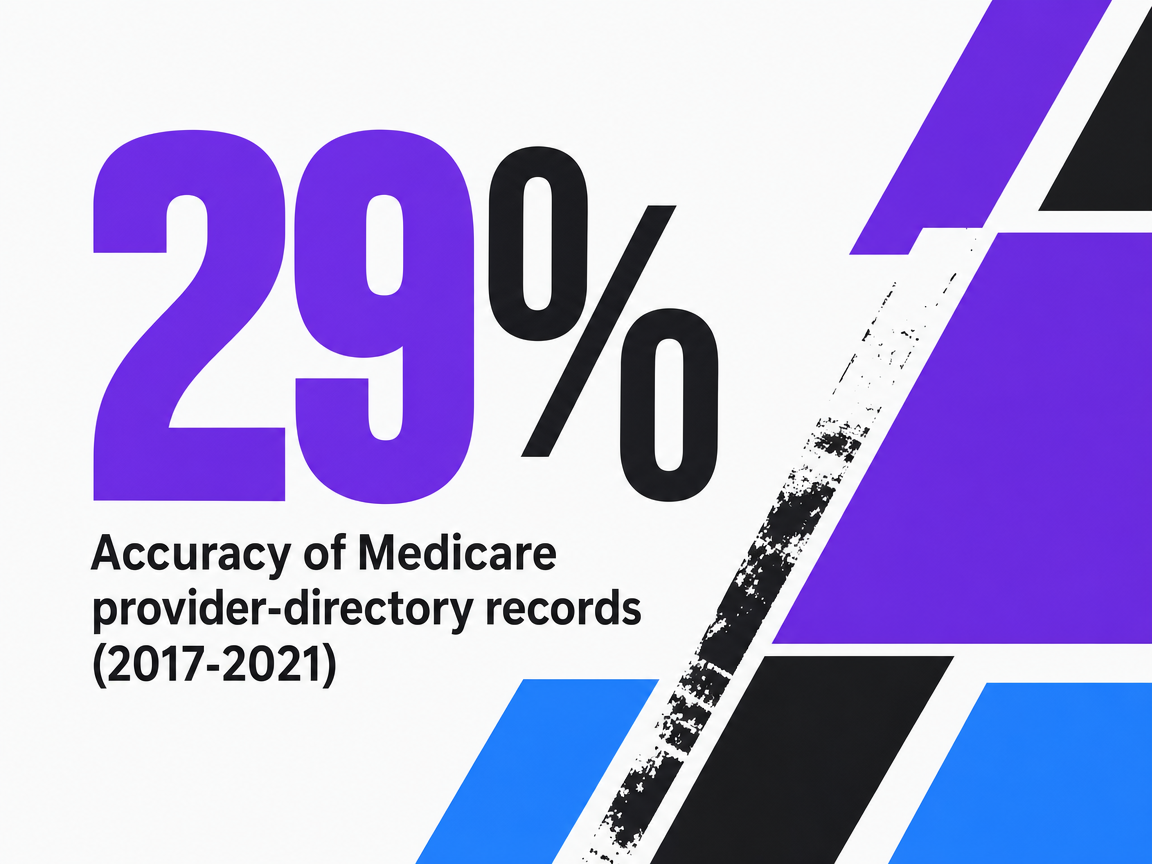 Accuracy of Medicare provider-directory records (2017-2021)
Accuracy of Medicare provider-directory records (2017-2021)
Accuracy of Medicare provider-directory records (2017-2021)
The public fields that must match across every location
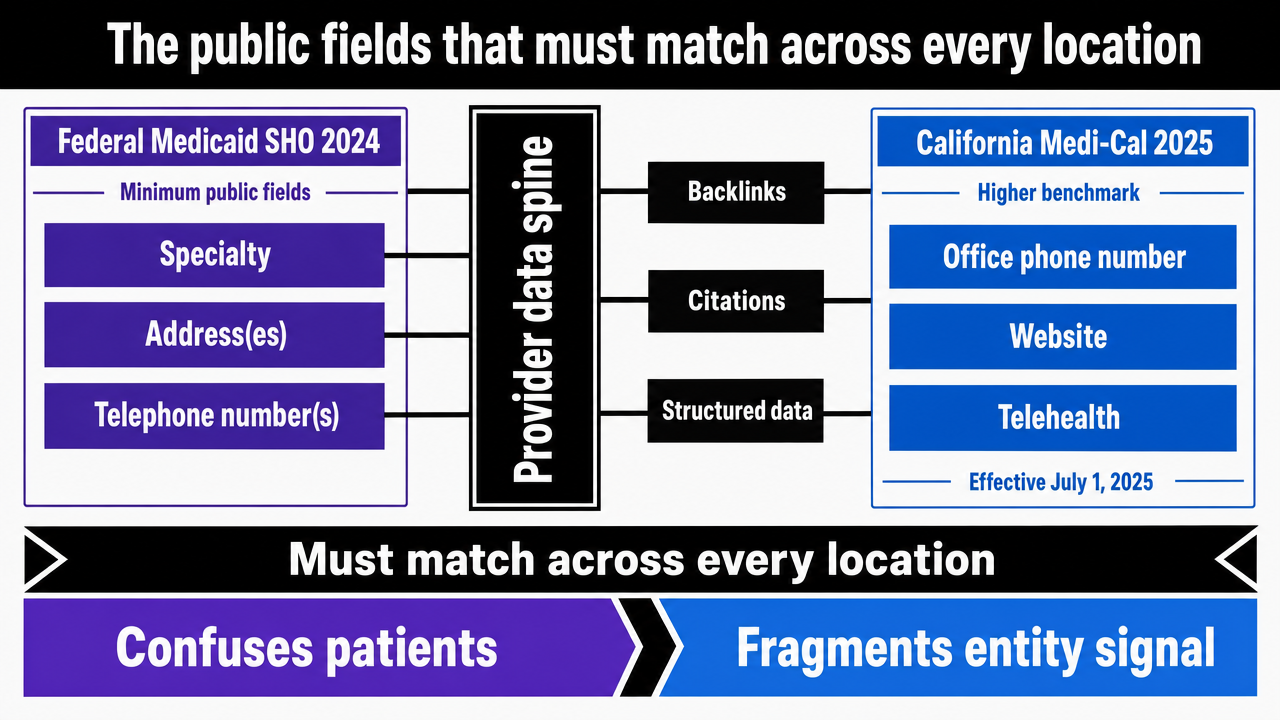
Federal Medicaid guidance issued to State Health Officials in 2024 specifies the minimum public fields every directory must include for each provider record: specialty, address(es), and telephone number(s) 3. These are the core components of the provider data spine and the anchors for every backlink, citation, and structured-data block a multi-location operator publishes. If a hospital association page lists one phone number for a location while the operator's own location page lists another, this inconsistency not only confuses patients but also fragments the entity signal that an earned link is meant to consolidate.
California's Medi-Cal requirements, effective July 1, 2025, set a higher benchmark, which is relevant even for operators without Medi-Cal exposure. The state mandates that office phone number, website, telehealth status, and accessibility accommodations appear in the directory, and requires providers to update this data at least quarterly 4. Telehealth status and accessibility are not traditional NAP fields; they are newer attributes patients use for filtering, and local search increasingly highlights them. A behavioral health network with inconsistent telehealth availability across its hospital-system citations, state Medicaid record, and its own location pages will appear ambiguous in high-intent queries.
State directories also reveal patient search behavior. Wisconsin's consumer guide allows users to filter by county, city, state, or distance from a ZIP code 5. This is the discovery surface where earned links ultimately compete. For a 40 or 300-site footprint, the operational implication is clear: specialty, address, phone, website URL, telehealth status, accessibility, and acceptance fields must all resolve to the same canonical values everywhere they appear. They also require a refresh cadence at least as stringent as the strictest jurisdiction the operator encounters. Quarterly is the minimum; monthly is safer for groups with frequent provider movement, new openings, or service-line changes.
 Visualize the canonical provider-data fields required across all locations, drawing from Medicaid SHO 2024 and Medi-Cal 2025 requirements cited in the section
Visualize the canonical provider-data fields required across all locations, drawing from Medicaid SHO 2024 and Medi-Cal 2025 requirements cited in the section
How one bad NAP record erodes earned-link value downstream
Consider a single physician record with an outdated suite number. This record resides within the operator's enterprise master data and then propagates: into the state Medicaid directory, several commercial payer directories, a hospital-system affiliation page, the Google Business Profile for that clinic, the location's schema markup, and numerous secondary citations that scrape from these upstream sources. Each downstream system trusts the system above it, with no independent verification.
Now, add an earned link. A state medical society publishes a clinical update and links to the operator's location page for an affiliated specialist. The link points to a page whose schema conflicts with the payer directory, which conflicts with the Google Business Profile, which conflicts with citation aggregators. Search engines interpret this conflict as entity ambiguity. The link still carries authority, but it routes that authority to a fractured entity rather than a consolidated one.
This is the governance problem that the No Surprises Act frames as a compliance issue for healthcare providers subject to public disclosure 1, and it is the problem a national directory effort aims to solve at scale 15. For a marketing leader, the actionable point is upstream. Before any outreach campaign begins, the provider data spine must be canonical, versioned, and propagate consistently. Otherwise, every earned link diminishes its own value due to the inconsistency it encounters.
Test AI-Driven Backlink Campaigns for All Locations
Evaluate real-time healthcare backlink strategies and publish live results across your entire practice network during your trial.
The referring domains patients are actually taught to trust
Government, academic, hospital, and professional-association sources
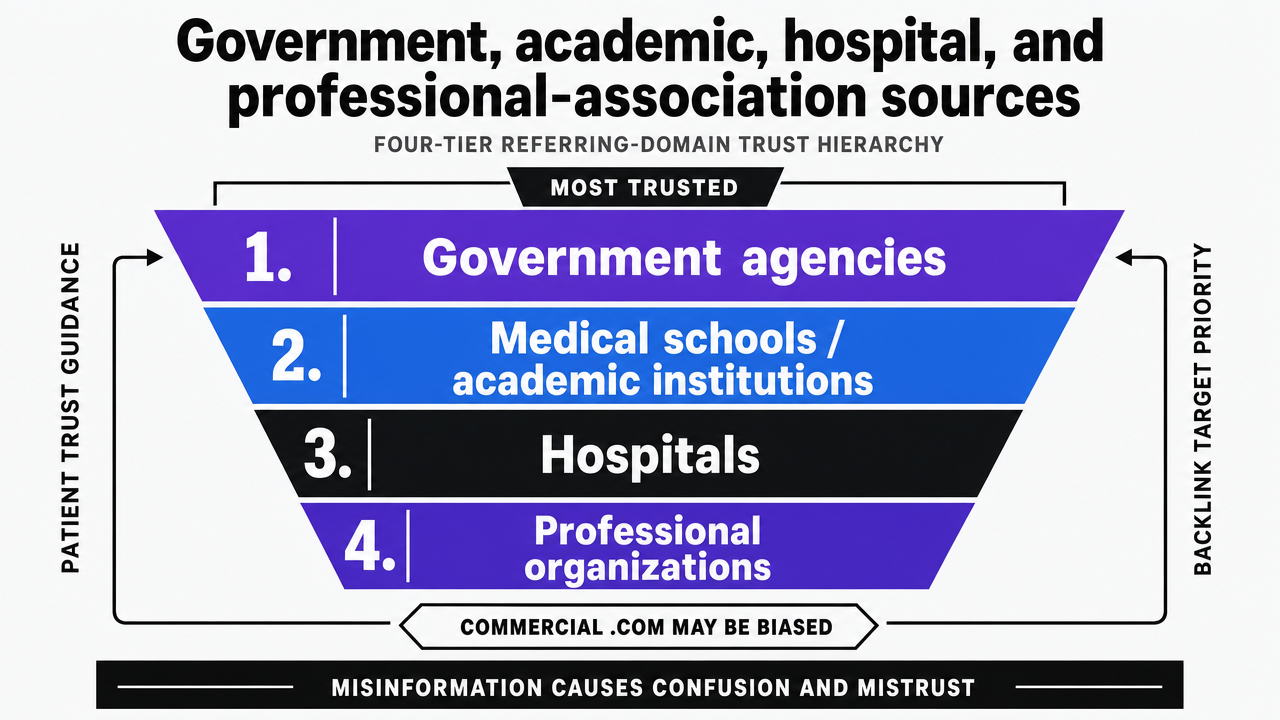
Federal patient-education resources are explicit about which referring domains patients should trust. MedlinePlus, the consumer arm of the U.S. National Library of Medicine, advises patients to favor websites from government agencies, medical schools, hospitals, and professional organizations, explicitly noting that .com sites may be biased due to commercial interests 12. The National Institute on Aging reinforces this hierarchy, stating that health websites sponsored by federal government agencies are accurate, and medical organizations, hospitals, and academic institutions can also be reliable 13. The U.S. Surgeon General's misinformation advisory supports this stance, warning that health misinformation can cause confusion, sow mistrust, and undermine public health efforts 11.
This guidance creates a useful tier structure for a multi-location backlink program:
- Top tier includes federal and state government domains: CMS, HHS, NIH, state departments of health, and state Medicaid agencies.
- The second tier is academic medicine: medical schools, teaching hospitals, and peer-reviewed journal sites with .edu or affiliated institutional domains.
- The third tier comprises hospital systems and large integrated delivery networks, including affiliation pages where a multi-site group's specialists are credentialed.
- The fourth tier consists of professional associations: specialty boards, state medical societies, and condition-specific clinical organizations.
Commercial .com publishers and aggregators rank below this stack, regardless of their domain-authority scores 12.
For a VP managing 40 to 300 sites, the operational implication is direct. The target list for earned coverage is not generic health bloggers. It is the set of domains patients are already instructed to prefer. Affiliation pages at academic medical centers where the group's physicians hold appointments, state society directories for credentialed specialists, hospital-system referring-provider pages, and clinical-guideline citations on professional-association sites all carry trust that patients are primed to recognize. These are also the domains where a single, cleanly propagated canonical provider record compounds its value across every clinic in the footprint, rather than each location pursuing its own coverage.
 Visualize the four-tier referring-domain trust hierarchy patients are taught to use, which is the framework this section establishes for prioritizing backlink targets
Visualize the four-tier referring-domain trust hierarchy patients are taught to use, which is the framework this section establishes for prioritizing backlink targets
Why commercial directory and social links sit lower in the stack
Commercial directories and social platforms are not without value, but they are often overvalued when placed at the top of a healthcare link program. MedlinePlus warns patients that .com sites may have commercial bias 12. A 2025 Med Care study found that even among respondents with high trust in the healthcare system, 34.9% still perceived substantial health misinformation on social media 10. This indicates that a significant portion of the audience viewing a social citation approaches it with skepticism.
Research on social health information credibility further clarifies this. Studies on identifying credible sources in social media emphasize that high-quality health information must be understandable, engaging, and culturally competent to influence patient judgment 14. A systematic review on infodemics warns that careless linking or endorsement of low-quality content amplifies misinformation through the same digital channels operators use for outreach 16. A link from a commercial wellness aggregator that recycles unverified claims carries reputational risk not captured by domain-authority scores.
This does not mean ignoring Google Business Profile, Healthgrades-style directories, or social channels. These are demand-capture surfaces, not trust-conferring referring domains. They should be treated as distribution channels for the canonical provider record produced upstream, not as authority sources that enhance the brand's standing with patients or search engines. The link program's authority budget should be allocated to federal, academic, hospital, and professional-association tiers, where patients are already directed to look 13.
Vetting any site before you accept or pursue a link
Outreach lists in healthcare require a vetting step often overlooked in agency workflows. The University of Minnesota's research guide on health misinformation provides a practical standard: sources should be science-based, objective, transparent, and accountable, explicitly acknowledging that scientific knowledge evolves 17. The NIA adds practical screens: clear purpose, expert authorship or review, current updates, and transparent sponsorship and contact details 13. MedlinePlus similarly recommends information no more than two to three years old 12.
Translated into a vetting checklist for a marketing operations team before any outreach or inbound-link acceptance:
- Confirm the publishing entity and its credentials.
- Verify that clinical content has a named author or reviewer with verifiable credentials.
- Ensure the page or site shows a recent update date.
- Confirm transparent sponsorship and conflict-of-interest disclosure.
- Screen for any sites promising miracle cures or quick solutions, which the NIA flags as reputational risks 13.
Both the Surgeon General's advisory and the infodemics review emphasize that organizations are responsible for the associations they make through outbound and inbound links 11, 16.
Apply the same standard to unsolicited inbound links. A link from a low-quality wellness aggregator lacking authorship, update cadence, and disclosed sponsorship is not a victory; it is a signal to disavow.
Operating the strategy at account level, not per location
One provider data spine feeding every citation and outreach asset
The account-level model begins with a single authoritative record per provider and per location, maintained in one system from which all downstream surfaces read. Specialty, address, phone, website URL, telehealth status, accessibility accommodations, and acceptance fields all resolve to canonical values in this central location 3, 4. Every other system—including the website's location pages, schema markup, Google Business Profile, payer directories, state Medicaid records, and citation aggregators—syncs from this spine on a defined cadence. Outreach assets also draw from this same record. When a state medical society requests a bio, headshot, or affiliation page for a specialist, the marketing operations team pulls fields from the spine rather than retyping them.
This architecture transforms how earned links compound. A backlink from a hospital-system referring-provider page or a professional-association directory points to a location whose data matches every other public surface the patient encounters 15. Search engines consolidate the entity rather than fragmenting it. Patients calling the number on the link reach the correct front desk. The link's authority lands cleanly because the asset it points to is internally consistent.
The question of update cadence directly follows. Medi-Cal's quarterly floor is the minimum for any operator with frequent provider movement, new openings, or service-line changes 4. CMS has also indicated that federal and state directory requirements expand annually 7. A spine that updates monthly, with automated propagation to downstream citations and outreach templates, absorbs these changes without requiring a per-location scramble.
Comparing execution models for multi-location link and directory work
Four execution models are commonly used for this work by multi-location operators. Each differs in how it handles coordination, cost behavior, directory-accuracy ownership, citation refresh cadence, compliance review, and time-to-execution. These differences are amplified across a 40 or 300-site footprint.
| Variable | In-house SEO team | Traditional agency, per-location retainer | Distributed freelancer network | AI marketing platform, account-level |
|---|---|---|---|---|
| Coordination model | Centralized, internal | Account manager per region or brand | Per-task assignment, no central owner | Single account plan across all sites |
| Per-location cost behavior | Fixed FTE load, scales with team size | Linear with site count | Linear with task volume | Flat, account-level |
| Directory-accuracy ownership | Marketing ops or shared with credentialing | Often excluded from scope | Not owned | Built into the data spine |
| Citation refresh cadence | Depends on staffing | Quarterly at best, often slower | Ad hoc | Monthly or tighter, automated propagation |
| Compliance review | Internal counsel or compliance team | Variable, rarely structural | Not provided | Built into the workflow |
| Time-to-execution | Slowed by hiring and capacity | Weeks per location request | Days per task, no consolidation | Continuous |
The economics primarily depend on whether cost scales with site count. Per-location retainers price each clinic as a separate engagement, meaning a 40-site dermatology group pays for forty discrete coordination overheads, forty separate directory audits, and forty independent outreach lists 4. Work that should be consolidated, such as the provider data spine and canonical citation set, becomes fragmented. Freelancer networks reduce unit cost but eliminate the central owner, a role crucial for addressing the directory-accuracy problem.
In-house teams can solve the coordination problem if adequately staffed, but headcount becomes challenging beyond 20 sites. A senior marketing operations lead, a technical SEO, a citations specialist, and a content reviewer with clinical literacy represent a four-person minimum before any earned-outreach work begins. Loaded costs quickly escalate, and the team still inherits the directory-governance problem that spans credentialing, payer enrollment, and provider data management.
Account-level platforms redefine the unit. Vectoron, for example, operates at $599 per month after trial, billed at the account level rather than per location. Directory accuracy, citation refresh, and outreach coordination are managed within a single workflow. The key structural point is not the price itself, but that the cost no longer scales with site count, and the data spine is no longer fragmented across multiple vendors. For a marketing leader evaluating a program for 40 or 300 sites, this variable determines whether the link strategy compounds or dilutes.
Scale High-Authority Healthcare Backlinks Across Every Location—From One Unified Platform
See how enterprise healthcare marketers and agencies coordinate, track, and execute scalable backlink strategies for multi-site practices—reducing manual overhead and improving domain authority with centralized oversight.
Earned editorial coverage on top of a clean foundation
With a canonical data spine and defined referring-domain tiers, earned editorial coverage begins to compound rather than dilute. The process for generating this coverage differs from generic outreach. Pitches are anchored to clinically verifiable content the group already possesses: peer-reviewed publications by credentialed specialists, registry data, outcome reporting, or guideline contributions linked to professional-association work. This is the type of material federal patient-education guidance instructs readers to seek when evaluating a source, including named expert authorship, current update dates, and transparent sponsorship 13, 12.
Three patterns of earned coverage significantly benefit multi-location operators:
- Contributed clinical commentary in state medical society publications and specialty-board newsletters, attributed to a named physician with verifiable credentials.
- Citations within clinical guidelines, position statements, or CME materials published by professional associations in which the group's specialists already participate.
- Affiliation and referring-provider pages at academic medical centers and hospital systems where specialists hold appointments, which carry the trust tier patients are taught to recognize 12.
The vetting standard applies in both directions. Outbound links from the group's own content should meet the science-based, objective, transparent criteria described by the University of Minnesota guide 17. Conversely, inbound coverage from publishers that fail the Surgeon General's credibility criteria is a candidate for disavowal, not a win 11. Earned authority only compounds when its underlying foundation remains clean.
On-site usability decides whether earned authority converts
A peer-reviewed usability analysis of U.S. academic medical center websites revealed that even institutions with the highest off-site authority in healthcare can have on-site experiences that hinder patients from efficiently finding critical information 9. This is a crucial point for multi-location operators. If teaching hospitals with .edu domains, federal research funding, and decades of institutional reputation lose patients due to navigation friction, a 40-site specialty group cannot assume that earned coverage from a state medical society or hospital-system referral page will convert on its own.
Three on-site failures consistently diminish link equity at the location level:
- Location pages that bury the phone number below fold-deep clinician bios.
- Appointment paths that route to a generic brand-level form instead of the specific clinic named in the referring link.
- Schema markup that conflicts with the visible NAP on the page itself.
Each of these breaks the connection between an authoritative referrer and the patient action the link was intended to produce.
The solution is straightforward: ensure the visible NAP, schema, and appointment endpoint on every location page match the canonical provider record. Then, audit the click path from the three or four highest-authority referring URLs and time the process, focusing on patient experience rather than just dashboard metrics.
Frequently Asked Questions
References
- 1.The No Surprises Act's Continuity of Care, Provider Directory ....
- 2.Request for Information; National Directory of Healthcare Providers and Services.
- 3.SHO Provider Directory - Medicaid.
- 4.Provider Directory Requirements for Medi-Cal Fee-For-Service Providers.
- 5.Consumer Guide: Provider Search | Wisconsin Department of Health Services.
- 6.2017-2021 Plan Year Notices Review Summary Report.
- 7.HIMSS23: Directing the Future of Healthcare Connectivity.
- 8.Provider requirements and resources | CMS.
- 9.An Analysis of US Academic Medical Center Websites: Usability Study.
- 10.Perceived Health Misinformation on Social Media and Public Trust in the Healthcare System.
- 11.Health Misinformation.
- 12.Online health information - what can you trust?.
- 13.How To Find Reliable Health Information Online.
- 14.Identifying Credible Sources of Health Information in Social Media.
- 15.Building a Reliable National Provider Directory—Lessons From the U.S. Experience.
- 16.Infodemics and health misinformation: a systematic review of reviews.
- 17.Health Misinformation: Home - Research Guides.