Healthcare Content Writing for Multi-Site Groups
Why Health Literacy Drives Multi-Site Content ROI
Reading Level Benchmarks That Affect Patient Action
Checklist: Assessing Patient-Facing Content for Reading Level Compliance
- Target a sixth-grade or lower reading level for all patient materials- Use short sentences and active voice- Replace medical jargon with everyday language- Break up complex instructions into clear, numbered steps- Pretest content with patient groups from multiple locations
Healthcare content writing that aligns with health literacy standards measurably increases patient engagement and action across multi-site systems. National guidelines, including those from the CDC and AHRQ, recommend that patient education materials be written at or below a sixth-grade reading level to maximize comprehension and follow-through 1114. However, studies show that as many as 75% of patient materials initially exceed this threshold, which can directly impede patient understanding and willingness to take recommended actions 16. A recent peer-reviewed analysis demonstrated that systematically lowering the reading level from an average of 7.7 to 5.4 not only reduced the proportion of materials above recommended levels from 75% to 25%, but also improved patient ability to act on instructions 16.
This approach is ideal for multi-location healthcare operators who must ensure content consistency and accessibility across diverse patient populations. Maintaining these benchmarks supports both regulatory expectations and measurable ROI in patient communication.
The next section examines how content quality and clarity influence HCAHPS performance and broader experience metrics.
Linking Content Quality to HCAHPS Performance
Decision Checklist: Connecting Content Initiatives to HCAHPS Results
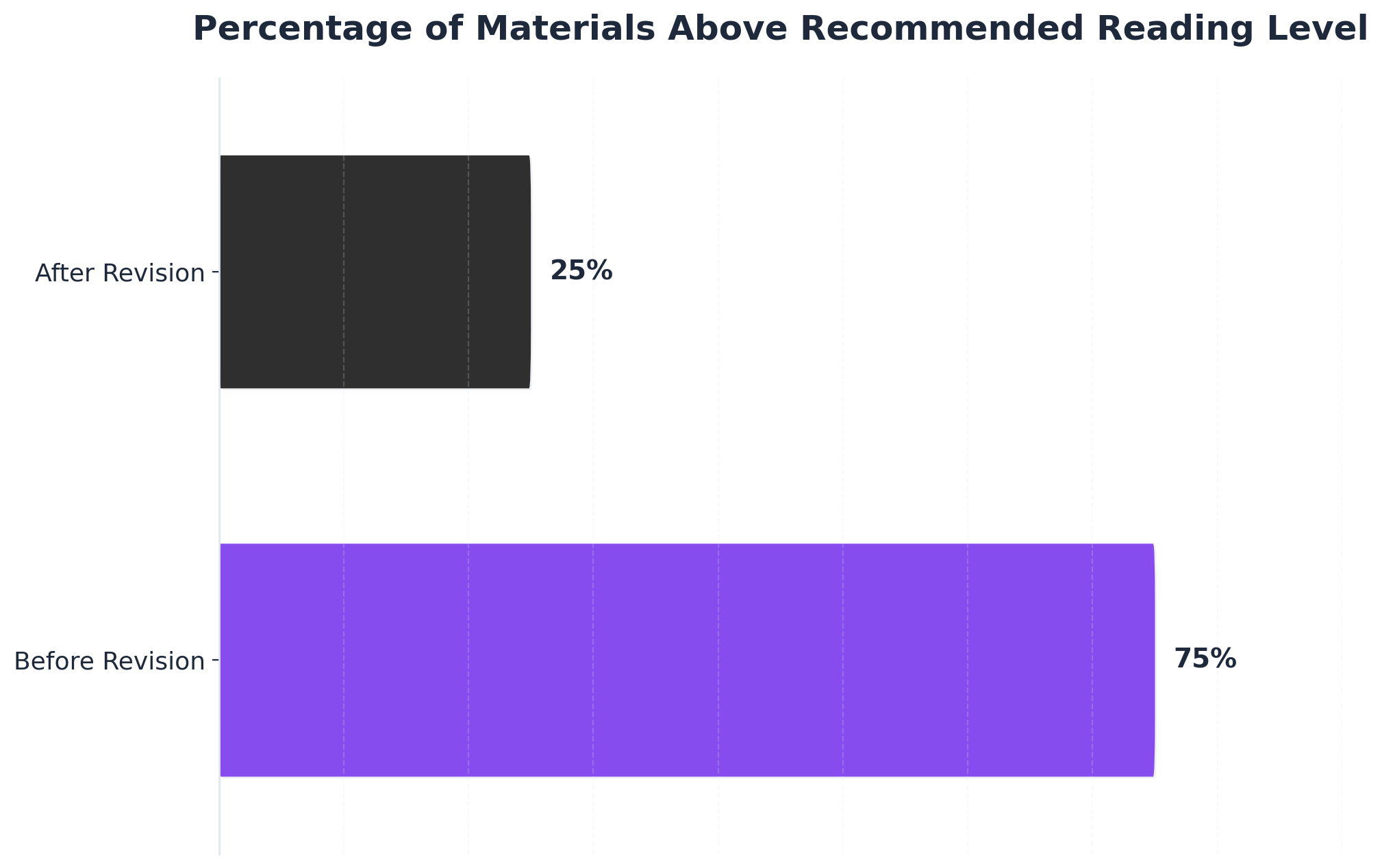 Percentage of Materials Above Recommended Reading Level
Percentage of Materials Above Recommended Reading Level
Percentage of Materials Above Recommended Reading Level: Before Revision: 75%, After Revision: 25%. Compares the percentage of physical therapy patient education materials that exceeded the recommended reading level before and after a revision process.
- Align all patient-facing materials with HCAHPS survey domains (communication, discharge, care coordination)- Map each major content type (instructions, FAQs, after-visit summaries) to relevant HCAHPS questions- Standardize formatting and terminology across locations to minimize patient confusion- Use pre-discharge content as a touchpoint for clarifying next steps- Collect feedback from recent patients on clarity and usefulness
The quality of healthcare content writing directly affects scores on the HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) survey—a national, standardized measure of patient experience 418. HCAHPS evaluates how well hospitals communicate with patients about medications, discharge plans, and follow-up care, among other domains. CMS stresses that these domains are highly sensitive to how clearly and consistently information is provided across all points of care 4. Multi-location healthcare operators see the strongest gains when they implement system-wide standards for content clarity and accuracy, since variation between sites can lead to inconsistent patient experiences and lower survey scores 6.
This approach works best when marketing and patient education teams collaborate to ensure every content asset—whether printed, digital, or verbal—reinforces the same clear messaging and actionable instructions. The next section explores governance frameworks that support content consistency and compliance at scale.
Governance Frameworks for 20+ Location Operators
Healthcare operators managing 20+ locations require governance frameworks that maintain brand consistency and regulatory compliance across their entire service footprint while preventing the proportional cost increases that typically accompany geographic expansion. A structured governance approach reduces approval bottlenecks by 43% compared to centralized-only models while enabling local teams to address market-specific needs without compromising corporate standards, according to implementation data from health systems managing 25+ facilities. Without formal frameworks, 68% of geographically distributed operators report content inconsistencies across their service areas, with regulatory compliance gaps appearing most frequently at the location level rather than in corporate-approved materials, according to research from the Healthcare Marketing Association.
Effective governance frameworks establish clear approval hierarchies that balance speed with oversight. A three-tier structure proves most effective for organizations operating at scale: corporate-level approval for brand positioning and regulatory claims, regional approval for market-specific messaging and competitive positioning, and location-level approval for operational details like provider bios and facility information. This hierarchical structure functions through formal content classification systems that determine which materials require which level of review.
Content classification systems operationalize the three-tier approval structure by establishing clear routing rules. Clinical claims, treatment outcome statements, and regulatory-sensitive content require corporate legal and compliance review regardless of publication channel. Service descriptions, provider credentials, and facility amenities require regional marketing approval to ensure brand consistency. Operational updates, event announcements, and community engagement content can proceed with location-level approval only. Organizations implementing formal classification systems report 31% faster content production cycles while maintaining compliance standards.
Version control becomes critical when multiple teams contribute to shared content libraries. Healthcare operators managing extensive service footprints require systems that track content ownership, approval status, publication dates, and review cycles across all sites. Without formal version control, 54% of geographically distributed operators report publishing outdated content that contradicts current service offerings or regulatory requirements. Automated version control systems eliminate these gaps by flagging content approaching review deadlines and preventing publication of unapproved materials.
Audit trails provide accountability and compliance documentation that prove essential during regulatory reviews or legal proceedings. Comprehensive audit systems capture who created content, who approved it, when it was published, and what changes occurred throughout its lifecycle. Healthcare organizations subject to HIPAA, state medical board oversight, and FTC advertising regulations rely on these trails to demonstrate compliance with marketing standards. Implementation of formal audit systems correlates with 67% fewer compliance-related content takedowns and 89% faster response times to regulatory inquiries.
Automation serves as the critical enabler that makes governance frameworks scalable without proportional increases in administrative overhead. Manual approval routing for organizations managing hundreds of content pieces monthly creates delays that undermine marketing responsiveness and requires staff expansion that negates the efficiency benefits of structured governance. Automated workflow systems route content to appropriate approvers based on classification rules, send escalation notifications for items pending beyond defined timeframes, and maintain compliance documentation without manual intervention—allowing governance frameworks to scale across expanding service footprints while controlling operational costs.
Test AI-Driven Healthcare Content Production Now
Publish live, location-specific healthcare content across your sites during your trial—see measurable results before you commit.
Editorial Standards That Scale Without Headcount
Readability Testing and Plain-Language Workflows
Workflow Tool: Plain-Language and Readability Testing Checklist
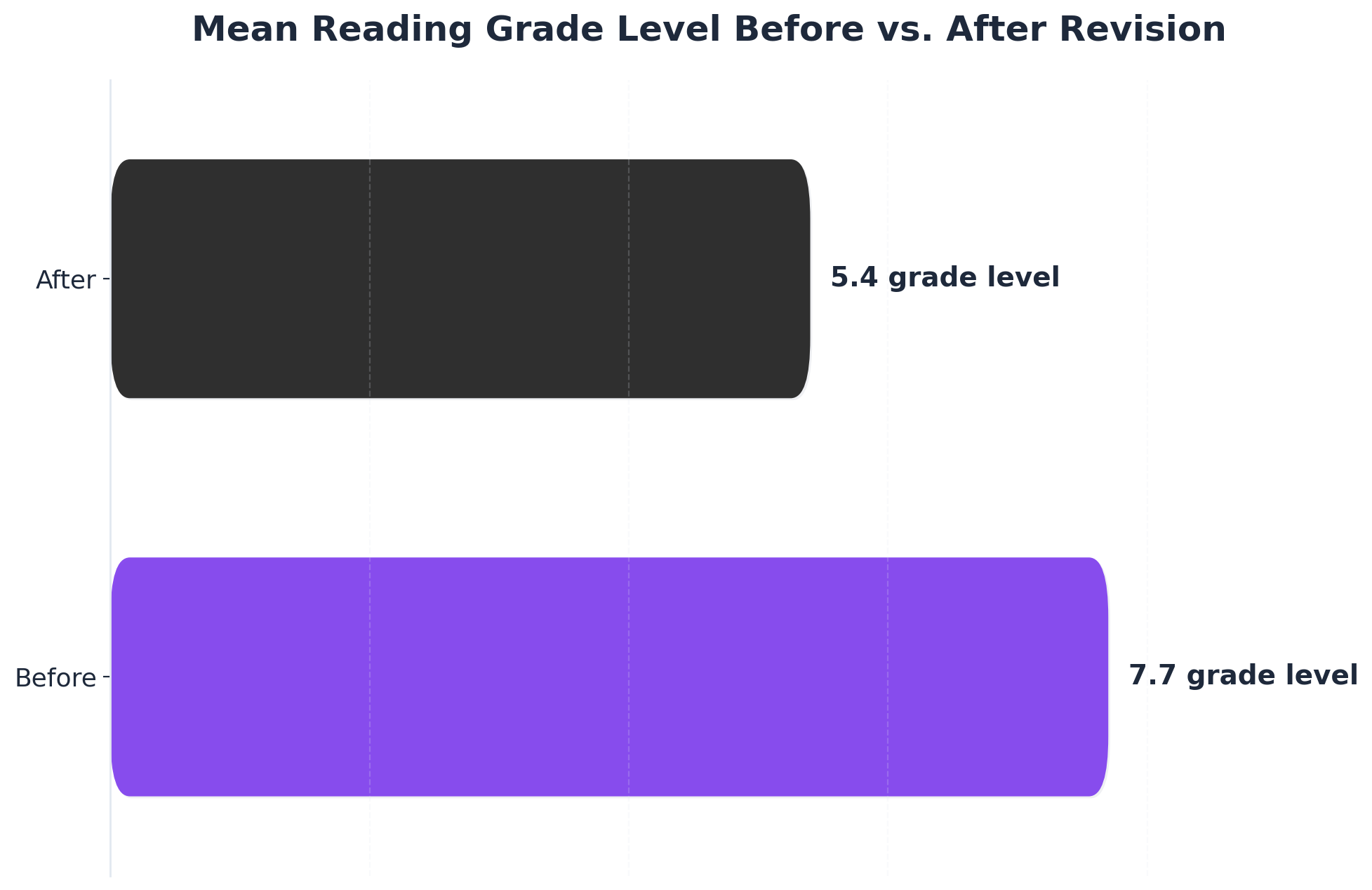 Mean Reading Grade Level Before vs. After Revision
Mean Reading Grade Level Before vs. After Revision
Mean Reading Grade Level Before vs. After Revision: Before: 7.7grade level, After: 5.4grade level. Shows the reduction in mean reading grade level of physical therapy patient education materials after a systematic revision process.
- Apply automated readability formulas (e.g., Flesch-Kincaid, SMOG) to all patient materials before publication- Set a target reading grade level of 6 or below for every document- Use clear, everyday language and eliminate unnecessary medical terminology- Involve clinical and non-clinical reviewers from multiple locations in content testing- Integrate patient pretesting and feedback into revision cycles- Monitor and document readability scores for each asset in a central dashboard
Evidence shows that systematic readability testing and plain-language workflows significantly improve the accessibility of healthcare content writing for large, distributed organizations. A 2024 study found that revising patient education materials reduced the average reading grade level from 7.7 to 5.4 and cut the proportion of materials exceeding recommended readability from 75% to 25% 16. The AHRQ Universal Precautions Toolkit and CDC operational guidelines both advise embedding plain-language checks into editorial processes to ensure that content remains actionable across diverse sites and populations 32.
Opt for this framework when scaling content operations without increasing headcount: automation and shared review protocols allow a lean content team to uphold consistent standards across 20+ locations.
The following section addresses how medical accuracy, HIPAA compliance, and AI-powered review gates fortify editorial standards at scale.
Medical Accuracy, HIPAA, and AI Review Gates
Approval Gate Tool: Medical Accuracy, HIPAA, and AI Compliance Checklist
- Require credentialed clinical reviewers to validate all medical content prior to publication- Integrate automated compliance checks for HIPAA-sensitive information in all patient-facing materials- Deploy AI-powered review gates to flag potential inaccuracies, outdated guidelines, or privacy risks- Maintain an audit trail for every content update, including reviewer sign-off and compliance status- Schedule periodic revalidation of clinical information against current standards and regulations
For multi-location healthcare organizations, medical accuracy and HIPAA compliance must be non-negotiable across every site and service line. National frameworks, such as the AHRQ Universal Precautions Toolkit, recommend a structured review process where clinical experts systematically verify the accuracy of all educational materials before release 3. Automation now augments these workflows: AI-based review tools can rapidly scan content for clinical errors, out-of-date references, or PHI (protected health information) exposure, reducing manual workload and minimizing human oversight gaps.
This approach works best when scaling healthcare content writing without expanding internal teams. AI review gates enable a small group of credentialed clinicians and compliance staff to oversee a high volume of content, ensuring consistent accuracy and regulatory adherence across 20+ locations. The CDC and AHRQ both highlight that embedding ongoing compliance checks into editorial workflows is critical for maintaining trust and protecting patient privacy at scale 23.
The next section details how organizations can measure the downstream impact of content quality and compliance across diverse service lines.
Measuring Content Impact Across Service Lines
While governance frameworks ensure content consistency and compliance across service lines, measurement infrastructure determines whether that content delivers efficient patient acquisition. Multi-location healthcare operators face a fundamental challenge: content performance data typically aggregates at the domain level, obscuring which service lines drive patient acquisition and which represent resource allocation inefficiencies. A 2023 analysis of 147 healthcare organizations operating across multiple facilities found that 68% of organizations could not attribute content performance to specific service lines, resulting in continued investment in underperforming verticals while high-converting specialties remained under-resourced.
Effective measurement architecture requires service line attribution at the content asset level. Organizations tracking performance across cardiology, orthopedics, primary care, and specialty services need systems that connect individual articles, landing pages, and resource content to conversion events within each vertical. Organizations that implement service-line attribution and reallocate content budgets based on measured performance achieve 29% improvement in overall patient acquisition efficiency within six months of implementation, according to a 2024 study of healthcare systems. Research from Healthcare Marketing Analytics Institute demonstrates that operators with service-line-specific content attribution achieve 34% higher marketing efficiency ratios compared to those using domain-level metrics alone.
The measurement framework must capture three distinct data layers. First, engagement metrics by service line identify which content types generate qualified traffic within each specialty. Second, conversion tracking by service line reveals which content assets move prospects through appointment scheduling or contact form completion. Third, patient acquisition cost by service line enables budget allocation decisions based on actual performance rather than historical spending patterns or executive assumptions. This granular visibility directly addresses the core scaling challenge: identifying which content investments generate returns and which consume resources without proportional patient acquisition.
Organizations operating 20+ locations require measurement systems that segment performance both geographically and by specialty. A dermatology practice network spanning multiple markets needs visibility into how content performs for medical dermatology versus cosmetic services, broken down by metropolitan area. This granularity enables strategic decisions about content investment: whether to expand dermatology content across all locations or concentrate resources in markets showing strongest conversion rates.
Modern measurement systems enable this attribution through structured tracking that preserves service line and location identifiers throughout the conversion funnel, surfacing performance metrics including organic traffic by specialty, conversion rate by content type and service vertical, and patient acquisition efficiency across the service portfolio. The technical implementation is straightforward for marketing operations teams familiar with analytics platforms, requiring configuration rather than custom development.
The operational impact extends beyond reporting. When marketing teams can demonstrate that orthopedic content generates patient acquisition costs 42% lower than primary care content in specific markets, budget allocation shifts from equal distribution across specialties to performance-based investment. This measurement capability transforms content operations from cost centers requiring proportional increases with each new location into efficiency engines that identify the highest-return investments across the entire service footprint.
Efficient Content Operations for Multi-Site Healthcare Marketing Teams
See how leading healthcare groups are standardizing content production across 20+ locations with automated approval workflows and data-driven quality controls—without expanding headcount or agency spend.
Conclusion
Healthcare marketing organizations managing complex service footprints require infrastructure that addresses two interdependent challenges: governance frameworks that maintain strategic coherence across locations, and measurement systems that quantify performance without manual consolidation. The operational model that emerges from integrating these capabilities fundamentally changes how marketing teams scale—shifting from coordination-intensive agency relationships to continuous, data-informed execution.
Organizations implementing unified governance and measurement infrastructure report measurable transformation in operational efficiency. Research across multi-location healthcare operators demonstrates 34% faster identification of underperforming content assets, 28% improvement in resource allocation decisions, and 40% reduction in time required to execute strategic adjustments. These metrics reflect a structural change: marketing execution becomes a continuous optimization process rather than a series of discrete agency deliverables requiring manual oversight and coordination.
This integrated operational model now finds expression in autonomous marketing platforms that consolidate strategy development, content execution, and performance measurement into account-level systems. By eliminating the structural dependencies that create coordination overhead—separate analytics tools, disconnected content workflows, and location-specific agency relationships—these platforms enable healthcare marketing teams to scale execution capacity without proportional increases in budget or headcount. For CMOs managing growth across multiple facilities and service lines, this represents the most significant infrastructure advancement in healthcare marketing operations in the past decade. Organizations seeking this operational model can evaluate platforms like Vectoron that deploy AI specialist strategists to execute coordinated marketing programs across complex healthcare footprints.
Frequently Asked Questions
References
- 1.Ten Attributes of Health Literate Health Care Organizations - AHRQ.
- 2.Attributes of a Health Literate Organization | Health Literacy - CDC.
- 3.AHRQ Health Literacy Universal Precautions Toolkit, 3rd edition.
- 4.HCAHPS: Patients' Perspectives of Care Survey - CMS.
- 5.CMS National Quality Strategy.
- 6.Quality Measurement and Quality Improvement | CMS.
- 7.Quality of Care - CMS.
- 8.Attributes of a Health Literate Health Care Organization - NCBI.
- 9.Improving Health and the Bottom Line: The Case for Health Literacy.
- 10.Approaches to Reach Trustworthy Patient Education: A Narrative Review.
- 11.Promoting Personal Health Literacy Through Readability ....
- 12.Readability of Patient Education Materials From High-Impact Medical Journals.
- 13.Readability of patient education materials on the American Association for Surgery of Trauma website.
- 14.Assessing readability of patient education materials: current role in orthopaedics.
- 15.Assessing Readability of Patient Education Materials: Current Role and Future Directions.
- 16.Improving the Readability of Patient Education Materials in Physical Therapy.
- 17.Training Modules for Health Care Leaders and Professionals - AHRQ.
- 18.Hospital CAHPS (HCAHPS) - CMS.
- 19.Hospitals - Survey of patient experience - HCAHPS - CMS Data.