Key Takeaways
- Multi-location healthcare marketing is an operating-model question, not a tactics question, with HIPAA authorization 7 and the September 2025 FDA disclosure reforms 1213 now binding at the production layer.
- Compliance must be encoded across four stages — audience construction, brief approval, creative composition, and copy review — rather than sitting as a final blocking gate that breaks past five or six sites.
- AI carries three documented production functions — audience segmentation, CRM personalization, and predictive analytics on engagement 5 — while humans own three rule-level approval gates: brand, medical, and compliance.
- Before any vendor conversation, audit the data layer for PHI boundaries, walk an asset through the compliance sequence, count handoffs per launch, and run per-location output, cost, and review-hour math.
The Coordination Problem Hiding Inside the Monthly Retainer Invoice
A 40-site MSO publishing two location pages, one service-line update, and a clinician bio in a single sprint isn't running a content program. It's running a routing problem. The retainer invoice rarely shows what the operator is actually paying for: nine handoffs between an account manager, a strategist, a copywriter, an in-house brand reviewer, a clinical reviewer, a compliance reviewer, an SEO lead, the agency producer, and the local office manager who has to confirm the address block.
The retainer-plus-coordinator model was built for one brand and one website. It treats patient-needs research as a kickoff deliverable rather than something to refresh against live data 6. At five or six sites, that design holds. Past that, every new location adds review cycles that compound rather than divide.
The frame this article uses is deliberate. Healthcare marketing strategies for a multi-location operator is not a tactics question — SEO, paid social, email nurture, review management — it's an operating-model question. Under HIPAA marketing authorization rules 7 and the September 8, 2025 FDA and HHS disclosure reforms 1213, the constraints are now binding at the production layer. The right question is where compliance, production volume, and approval authority should sit.
Compliance as a Design Constraint, Not a Sidebar
HIPAA Authorization Reshapes Targeting and AI Training Data
HIPAA's marketing rule is narrower than most operators treat it. Written authorization is required before protected health information is used or disclosed for marketing, with limited exceptions for face-to-face communication and promotional gifts of nominal value 7. That rule was written long before lookalike audiences, CRM-fed retargeting pools, and AI segmentation pipelines existed, but it applies to all of them.
The operational consequence sits in the data layer. A 60-clinic behavioral health network cannot pipe diagnosis-coded visit data into a paid-social audience without authorization, even if the data is hashed before upload. The same constraint governs what an AI segmentation model is allowed to train on. If the training corpus contains PHI tied to identifiable individuals, the authorization requirement attaches to the model's downstream use in marketing — not just to the original record.
This reshapes how a multi-location operator structures the marketing data spine. Patient-level signals stay inside the covered entity's environment, governed by a BAA. Marketing-side audiences are built from de-identified or non-PHI signals: form fills, GMB engagement, Search Console queries, GA4 events scoped to non-clinical pages. The AI layer reads from the marketing-side spine, not the clinical one. Treating that boundary as a design rule, encoded once at the account level, eliminates the per-location authorization audits that retainer workflows tend to skip.
The September 2025 Disclosure Regime Changes What Creative Has to Carry
On September 8, 2025, HHS and FDA closed the 1997 "adequate provision" loophole that had let direct-to-consumer drug advertising point viewers to a website or toll-free number for safety information 1213. The reform requires full safety warnings in the ad itself. More than 60 warning letters went out alongside the announcement 12. The enforcement signal is unambiguous: digital placements that previously offloaded risk language to a landing page are now non-compliant on their face.
For multi-location operators, the immediate exposure isn't pharma ads — it's the adjacent creative running across service lines. Weight-management programs naming GLP-1 medications. Dermatology practices promoting prescription topicals. Behavioral health groups advertising MAT services. A 30-second paid social spot that mentions a drug class now has to carry the safety information on screen, not behind a click. The creative spec changes. The review queue changes. The asset library changes.
The four binding rules — HIPAA marketing authorization 7, FDA deceptive-advertising enforcement 12, full safety disclosure 13, and the plain-language consumer rule 14 — intercept the production pipeline at four distinct stages: audience construction, brief approval, creative composition, and final copy review. A pre-September-2025 workflow typically had compliance sitting at the end as a blocking gate. That sequencing breaks now. Audience rules must be enforced before a brief is written. Disclosure requirements must be encoded in the creative template itself, not bolted on at proof. Plain-language conversion has to happen during drafting, not as a redline pass three days before launch. The diagram an operator should keep visible: four checkpoints, four stages, no sidebar.
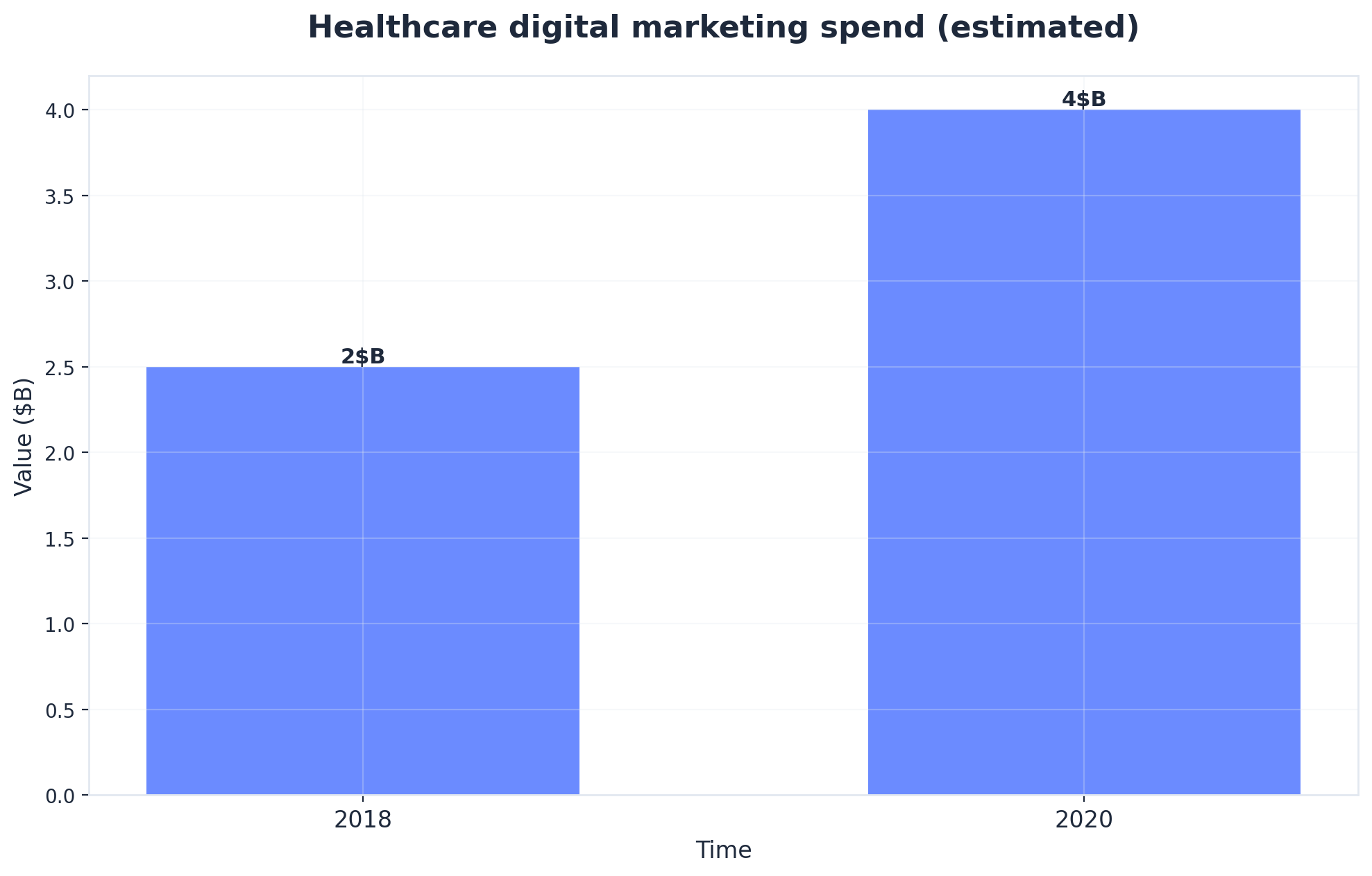 Healthcare digital marketing spend (estimated)
Healthcare digital marketing spend (estimated)
Healthcare digital marketing spend (estimated): 2018: $2.5B, 2020: $4B. Source: The impact of marketing strategies in healthcare systems - PMC - NIH.
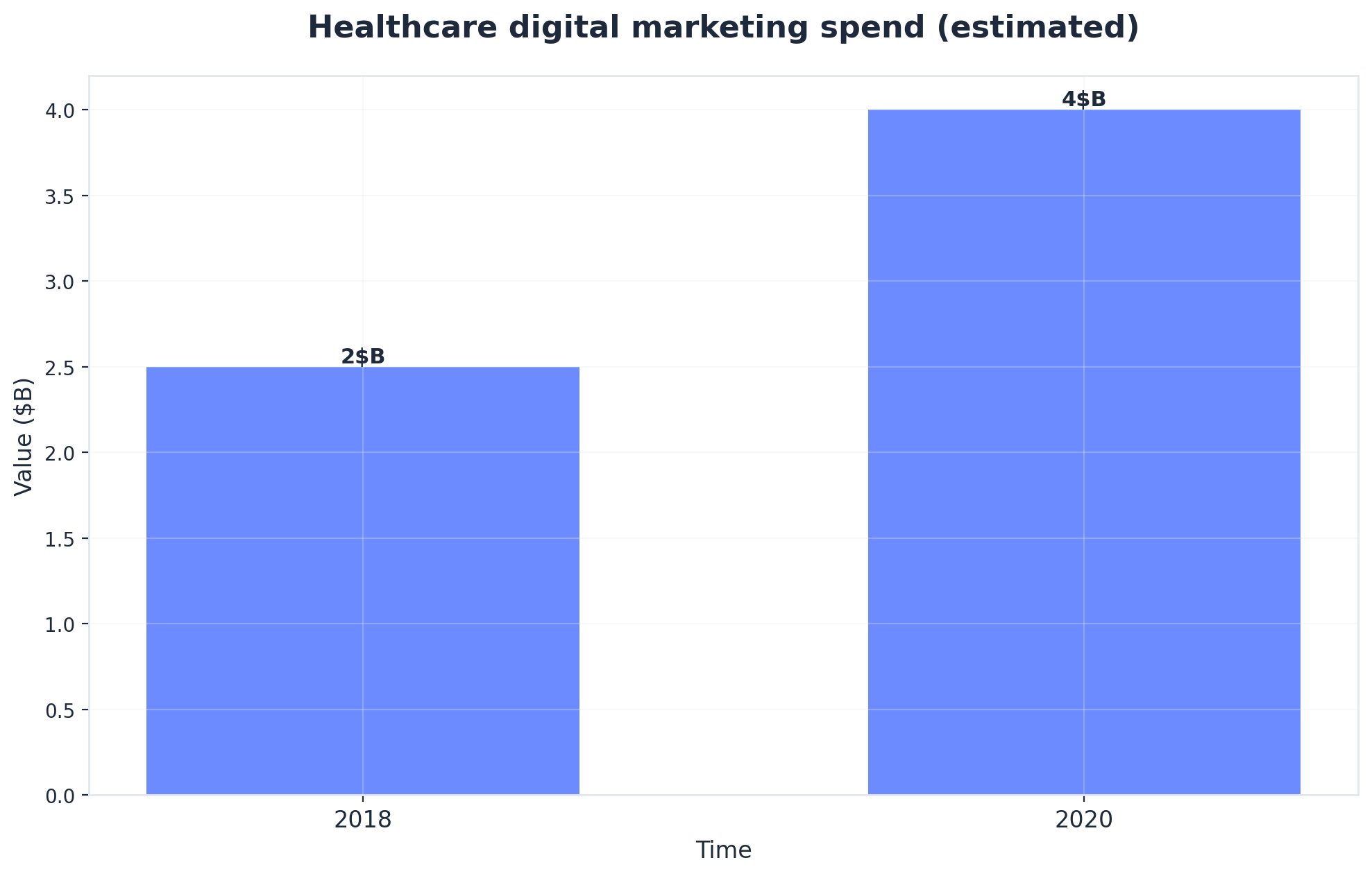 Healthcare digital marketing spend (estimated)
Healthcare digital marketing spend (estimated)
Healthcare digital marketing spend (estimated): 2018: $2.5B, 2020: $4B. Source: The impact of marketing strategies in healthcare systems - PMC - NIH.
Plain-Language Rules Make Copy Review a Production Workflow Problem
The FDA's plain-language rule requires consumer-facing drug information to use everyday words — "fainting" instead of "syncope," "high blood pressure" instead of "hypertension" — and to present risk information at a comprehension level a non-clinician can act on 14. Healthcare marketing teams have historically handled this with a final-stage medical reviewer who rewrites clinician-drafted copy. That works at one site with one reviewer. It does not work across 25 service-line landing pages drafted on overlapping deadlines.
Plain-language conversion is a production workflow problem, not a proofreading task. The reviewer's redlines need to feed back into the drafting layer so the next page on the queue starts closer to compliant rather than repeating the same conversions. In practice, that means terminology mappings, reading-level targets, and risk-presentation patterns are encoded as drafting inputs, not as post-hoc edits. The medical reviewer's role shifts from rewriter to approver, which is the only version of the role that scales past five locations.
Evaluate automated content workflows on real campaigns
Experience measurable improvements in patient acquisition efficiency using your own marketing data and published results.
The Three Operating Models on the Table
In-House Only: Headcount Scales With Locations
The in-house-only model concentrates strategy, production, compliance, and channel ownership under the marketing department. For a single-brand operator running six to ten sites, it produces the cleanest output: brand voice stays consistent, medical reviewers sit two seats away from copywriters, and HIPAA boundaries are enforced inside one set of access controls.
The math turns at the third service line. A behavioral health network that adds MAT services, adolescent IOP, and primary-care integration in the same fiscal year typically discovers that one writer, one designer, one paid-media manager, and one compliance reviewer cannot carry three new content programs without slipping launch dates. Hiring follows. A 25-site specialty group running a fully in-house team often staffs six to nine marketing FTEs before adding agency support for overflow. Patient-needs research that should refresh quarterly against live search and intake data instead becomes an annual offsite exercise 6. Headcount scales linearly with locations and service lines, which is the cost pattern operations leaders push back on hardest in a budget cycle.
Retainer Agency Plus Internal Coordinator: Built for One Brand, One Site
Most multi-location operators land here by accident. An agency relationship that worked at three sites carried over as the footprint grew, and an internal coordinator role was created to translate between the agency and the operations team. The retainer scope was written for one brand and one website, and never re-architected.
The coordination tax shows up in the calendar. A single service-line launch across 25 dental offices routes through the account manager, an agency strategist, an outside copywriter, the in-house brand reviewer, a clinical reviewer, the compliance reviewer, the agency's SEO lead, the agency producer, and the local office manager who confirms the address block and operating hours. Nine handoffs, each with its own queue. The agency's patient-needs research 6 was completed at onboarding and rarely refreshed against live Search Console data or intake-form drop-off patterns. Per-location billing means each new site adds a line item rather than absorbing into existing capacity. The model holds when the operator has one P&L and one site. It strains visibly past five or six locations and fails as a coordination layer at twenty-five.
Integrated AI-Augmented Execution: One Account-Level Data Spine
The integrated model inverts the structure. Compliance rules, brand standards, service-line taxonomy, and location metadata are encoded once at the account level. AI carries production volume across that spine — drafting location pages, service-line variants, paid-social copy, and email nurture sequences from a single brief that fans out into local outputs. Humans sit at three approval gates rather than nine handoff queues.
The evidence base for what AI actually carries in this layer is narrower than vendor decks suggest, which is the point. A scoping review screened more than 22,000 records published between 2014 and 2024 and identified 45 studies documenting AI's role in healthcare marketing under the patient-as-organization framework 5. Across those 45 studies, three production functions are consistently documented: audience segmentation, CRM personalization, and predictive analytics on engagement and retention signals 5. That is the working scope. AI is not the strategist, the medical reviewer, or the brand owner; it is the capacity layer that absorbs the volume retainers struggle to scale and that in-house teams cannot staff against.
For a 40-site MSO, the operational consequence is that one approved brief can produce 40 location-specific pages, 12 service-line variants, and the supporting paid-social and email assets in the same sprint window a retainer would spend on three deliverables. The data spine — GA4 events, Search Console queries, GMB engagement, intake-form completion — feeds the AI layer continuously rather than at quarterly review meetings.
Head-to-Head: Cost, Velocity, Compliance, Coordination, Time-to-Publish
A defensible operating-model decision requires comparison on the dimensions a VP actually argues in a budget review. Five matter: cost scaling pattern, monthly content output per location, compliance review ownership, multi-location coordination drag, and time-to-publish. The matrix below uses directional categorical language across the three models. No invented dollar figures.
| Dimension | In-House Only | Retainer + Coordinator | Integrated AI-Augmented |
|---|---|---|---|
| Cost scaling pattern | Linear with headcount; step-function on each new service line | Linear per location; line-item billing compounds past site five or six | Account-level; flattens as locations and service lines are added |
| Monthly content output per location | Constrained by FTE capacity; typically 1–2 assets per location | Constrained by handoff queue; agency throughput divided across sites | Higher volume on the same brief, drawing on documented AI roles in segmentation, CRM, and predictive analytics 5 |
| Compliance review ownership | Internal reviewer; concentrated risk if one role | Split between agency and internal; ambiguous accountability post–September 2025 1213 | Rules encoded once at account level; reviewer approves rather than rewrites 14 |
| Multi-location coordination drag | Low at fewer than 10 sites; rises with service-line expansion | Nine handoffs per launch; compounds with each new site | Three approval gates; coordination flat across locations |
| Time-to-publish | Days to weeks depending on FTE load | Weeks; gated by account-manager queue and review cycles | Days; gated by approval throughput, not production capacity |
The matrix is the artifact to walk into a budget review with. It reframes the conversation from "which agency" to "which operating model survives the next 15 locations and the post-September-2025 disclosure perimeter."
Where AI Sits in the Stack: Capacity Layer, Not Replacement
What AI Actually Carries in Healthcare Marketing Production
Vendor decks tend to overstate the surface area. The documented evidence base is narrower and more useful. The 45 studies surfaced by the patient-as-organization scoping review converge on three production functions where AI carries real load: audience segmentation against non-PHI signals, CRM personalization across email and SMS sequences, and predictive analytics on engagement and retention behaviors 5.
Inside a 40-site MSO, that translates into specific outputs. Segmentation models cluster GMB engagement, Search Console query patterns, and intake-form drop-off points into audience definitions a paid-media manager can act on without touching the clinical record. Personalization layers adjust subject lines, send times, and service-line emphasis per market. Predictive analytics flag which locations are losing organic visibility before the next quarter's reporting cycle catches it.
What AI does not carry is judgment about clinical accuracy, brand voice exceptions, or whether a given service line should be promoted at all. Reviews of AI in healthcare consistently frame reliability and safety as the gating concern, not capability 1011. The capacity layer absorbs production volume; it does not absorb accountability.
What Humans Still Own: Three Named Approval Gates
Three gates, three named owners. Anything more is coordination drag wearing a compliance costume.
The brand gate sits with the VP of Marketing or a delegated brand director. It approves the account-level brief — service-line taxonomy, voice standards, market-by-market positioning — once per cycle, not once per asset. The medical gate sits with a clinical reviewer empowered to approve rather than rewrite, because the plain-language conversion patterns and risk-presentation templates are already encoded in the drafting layer 14. The compliance gate sits with whoever owns HIPAA and FDA exposure for the operator. That reviewer approves the rules encoded at the account level — authorization boundaries 7, disclosure templates 1213, audience-construction constraints — and spot-checks outputs against them.
The shift is from line-by-line review to rule-level approval. A medical reviewer signing off on a terminology mapping covers every page that mapping touches. A compliance lead approving the disclosure template covers every paid-social variant rendered from it. The reviewer's hour count drops; their authority over what ships does not.
Org-Chart Contrast: Nine Handoffs vs. Three Approval Nodes
The retainer-plus-coordinator routing for a single service-line launch across 25 sites runs through nine queues: account manager, agency strategist, copywriter, in-house brand reviewer, clinical reviewer, compliance reviewer, agency SEO lead, agency producer, local office manager. Each queue holds the work for hours or days. The compounding effect is not additive — it is multiplicative against the location count.
The integrated routing collapses to three nodes sitting above an AI production layer: brand approval on the account-level brief, medical approval on encoded clinical rules, compliance approval on encoded regulatory rules. Production fans out to 25 location pages and 12 service-line variants from a single approved input. Local office managers confirm address blocks and hours through a structured data feed, not an email chain.
The org-chart contrast is the clearest artifact for an operations review. It shows where time goes, where accountability sits, and why the same headcount produces different output volumes across the two models.
See How Scalable Automation is Reshaping Healthcare Marketing Results
Connect with our team to benchmark your multi-location marketing efficiency, compare automation impact, and explore how AI-driven workflows deliver measurable improvements in patient acquisition at reduced operational cost.
If You Manage Multiple Locations: Coordination Drag Is the Real Cost
Per-Location Retainer Math Breaks Past Five Sites
This section addresses operators running ten or more locations, where the unit economics of a retainer relationship behave differently than they do for a single brand.
Retainer scopes typically price by deliverable count, not by complexity of distribution. A 25-location dental support organization buying "eight blog posts and four service-line pages per month" is buying a fixed pool that gets divided across the footprint, not multiplied. The agency's internal capacity is sized to the deliverable count, so adding a 26th office does not produce a 26th location page on the next sprint — it produces a line-item add-on, billed separately, queued behind whatever the existing 25 sites already have in motion.
The breakage point sits between sites five and six for most operators. Below that, an account manager can hold the routing in working memory and the patient-needs research done at onboarding 6 still describes the markets accurately. Above it, the handoff queue lengthens faster than throughput, address-block confirmations start blocking entire sprints, and per-location billing turns every new acquisition or de novo site into a procurement conversation. The cost pattern is not the headline retainer fee — it is the compounding line items, the coordinator headcount required to manage the agency, and the launch dates that slip when one office's compliance redline holds up the other 24.
One Brief, Many Pages: Centralized Production With Local Output
Centralized production inverts the unit of work. Instead of pricing per asset, the operator structures a single account-level brief — service-line definition, voice standards, disclosure templates, market segmentation logic — that fans out into location-specific outputs. A 60-clinic behavioral health network running a new MAT program approves one brief and renders 60 location pages, regional paid-social variants, and an email sequence keyed to each market's intake patterns from that single input.
The mechanics depend on a structured data layer the AI production layer can read against: GMB profiles, GA4 events scoped to non-clinical pages, Search Console queries, intake-form completion signals, and a location metadata table that holds clinician names, hours, accepted insurance, and address blocks. The documented AI production functions — segmentation, CRM personalization, predictive analytics on engagement 5 — operate on that spine. Local nuance is preserved through metadata, not through 60 separate copywriter assignments. The marginal cost of the 61st location is a row in the metadata table, not a new line item on next quarter's invoice.
Service-Line Velocity Under CMS Outcome Accountability
Service-line velocity matters more under outcome-accountable payment than under fee-for-service. CMS's TEAM model holds participating hospitals accountable for the cost and quality of episodes tied to specific surgical procedures for Original Medicare beneficiaries 8. The marketing consequence is direct: the operator needs to fill the right episodes with the right patients fast enough to hit volume targets while the bundled-payment math still works.
A 12-site orthopedic platform participating in TEAM-eligible procedures cannot wait six weeks for a retainer agency to produce procedure-specific landing pages, referral-physician outreach, and patient-education content across 12 markets. By the time those assets ship, the performance period has moved. Centralized production with local output collapses that timeline. One approved brief on lower-extremity joint replacement renders 12 location pages, 12 referral-targeted variants, and the supporting nurture content inside a single sprint. Velocity is the marketing input that outcome-accountable models reward, and it is the input retainer routing structurally cannot supply at footprint scale.
An Audit Sequence to Run Before Any Vendor Conversation
Four checks, in order. Run them before the next agency RFP, the next platform demo, or the next headcount request. Each one produces a number or a documented workflow that turns the operating-model question into a defensible recommendation.
1. Audit the data layer. Map every signal feeding marketing decisions today: GA4 properties by location, Search Console properties, GMB profiles, intake-form completions, CRM exports, paid-media audience sources. Flag anything that touches PHI. HIPAA authorization rules attach to AI segmentation models trained on identifiable patient data, not just to the original record 7. The output of this check is a two-column list — clinical-side signals governed by a BAA, marketing-side signals available for AI production — and a clear boundary between them.
2. Audit the compliance workflow. Walk a recent paid-social asset and a recent service-line page through the actual review sequence. Where do HIPAA authorization checks happen? Where do FDA disclosure requirements get encoded — in the creative template or as a redline pass? Where does plain-language conversion sit 14? If compliance reviewers are rewriting rather than approving, the workflow is sequenced wrong for the post–September 2025 perimeter.
3. Count the handoffs. For one typical multi-location launch, list every queue the work passes through, with name and average wait time. Nine handoffs is the retainer-plus-coordinator pattern. Anything above five is a coordination tax that compounds with each new site.
4. Run the per-location math. Three numbers, no estimates: monthly content output per location, fully loaded marketing cost per location, compliance review hours per location. Those numbers — not the headline retainer fee — show whether the current model survives the next 15 sites.
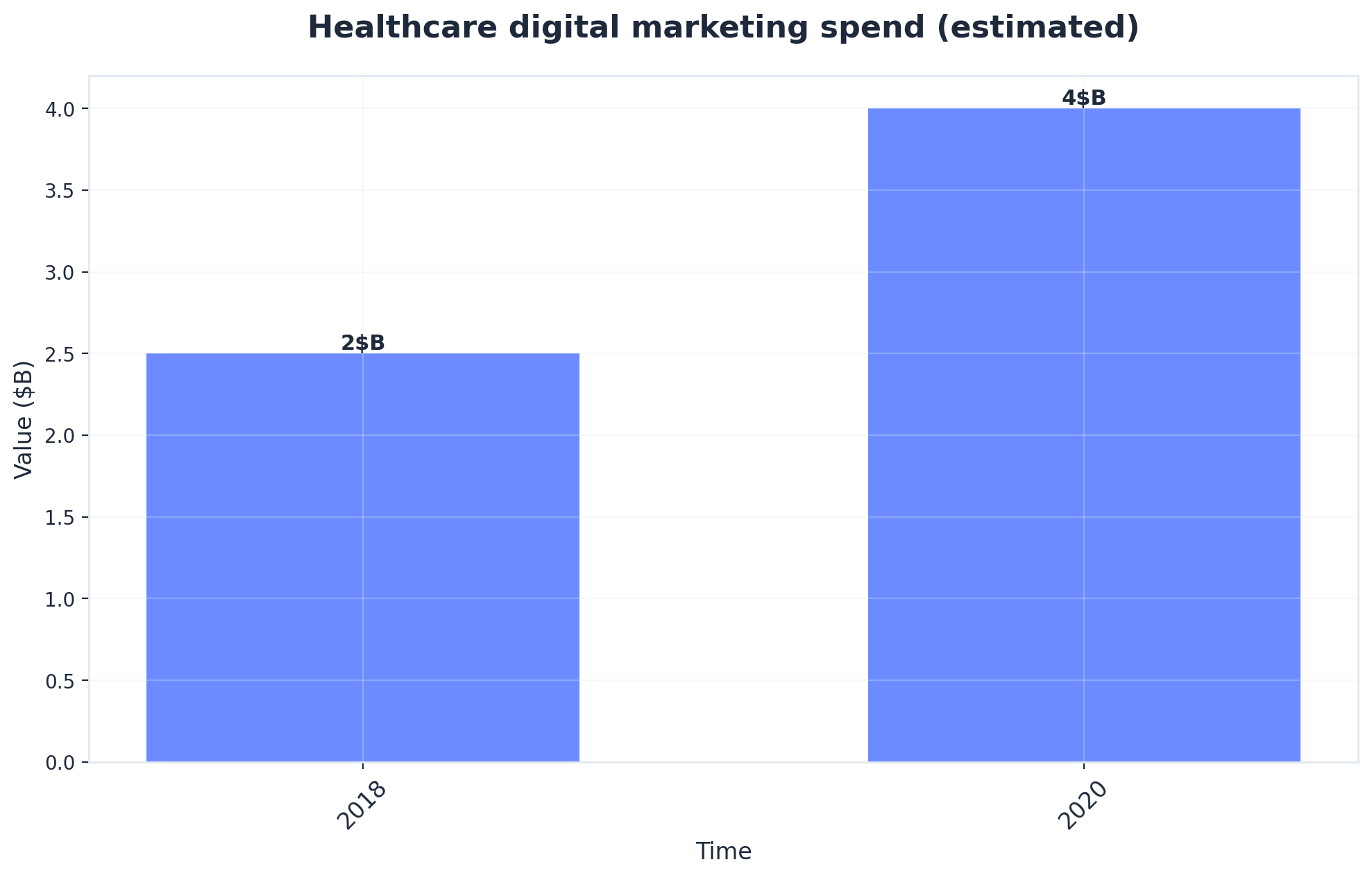 Healthcare digital marketing spend (estimated)
Healthcare digital marketing spend (estimated)
Healthcare digital marketing spend (estimated): 2018: $2.5B, 2020: $4B. Source: The impact of marketing strategies in healthcare systems - PMC - NIH.
Frequently Asked Questions
References
- 1.ACCESS (Advancing Chronic Care with Effective, Scalable ... - CMS.
- 2.Developing a direct-to-consumer telehealth strategy.
- 3.CMS' Value-Based Programs.
- 4.[PDF] Health Tourism Facility Use of Digital Marketing and AI.
- 5.Conceptual Model for the Integration of Marketing Strategies and ....
- 6.The impact of marketing strategies in healthcare systems - PMC - NIH.
- 7.Marketing | HHS.gov.
- 8.TEAM (Transforming Episode Accountability Model) - CMS.
- 9.AI Will Shape the Future of Marketing - Professional & Executive ....
- 10.Artificial intelligence in healthcare: transforming the practice of ....
- 11.2025 Watch List: Artificial Intelligence in Health Care - NCBI Bookshelf.
- 12.FDA Launches Crackdown on Deceptive Drug Advertising.
- 13.HHS, FDA to Require Full Safety Disclosures in Drug Ads.
- 14.Patients as Consumers: Reflections on the FDA's New Rule ... - PMC.