Key Takeaways
 Analysis of Healthcare Implementation Strategies
Analysis of Healthcare Implementation Strategies
A systematic review identified 36 other reviews covering 30 different strategies for implementing clinical practice guidelines in healthcare organizations.
- Location pages should run through a production pipeline with structured local inputs — provider roster, services, insurance, access notes — rather than being treated as one-off copywriting assignments that drift at scale.
- Provider expertise scales as a portfolio asset when each clinician is stored as a structured record feeding bios, dedicated pages, and authored content, since trust signals influence patient choice 2.
- Patient experience data from sources like HCAHPS and CAHPS surfaces site-specific friction points that should direct content priorities, since determinants vary by setting and population 1, 3, 4.
- Reviews capture bedside manner, staff, and facility experience rather than clinical quality 5, 8, so reputation programs and content claims should be calibrated to what the signal actually supports.
- Review velocity needs to be engineered across both owned and third-party channels because hospital-owned surveys show higher volume and more favorable ratings than independent platforms 7.
- Review narrative text predicts patient experience domains with 93% to 99% accuracy 11, making it a dual-purpose input for content roadmaps and local quality improvement.
- NAP and Google Business Profile consistency only holds past fifteen locations when managed from a canonical data layer with automated audits, mirroring strategies that sustain multi-site healthcare standards 9.
- Structured service comparisons — insurance, in-network status, availability, language support — match how patients actually decide 10and feed schema that distinguishes one location from another.
- Schema markup and internal linking should generate from the same canonical data powering location and provider records, with audit and feedback patterns keeping markup integrity intact 9.
- The production model — in-house, agency, or AI platform — should be chosen based on which cost and coordination curves stay flat as the next twenty locations come online.
- Acquisition measurement should report booked appointments and service-line conversion at the location level, with experience signals as a leading indicator, rather than hiding bottom-quartile sites behind portfolio averages 4, 11.
Why Multi-Location Healthcare SEO Breaks at Scale
The tactics that rank a single clinic almost never survive contact with a 40-site portfolio. A solo dermatology practice can hand-write a location page, prompt every patient for a Google review, and keep its NAP consistent with a quarterly spreadsheet check. A regional behavioral health network running 80 sites across six states cannot. The work item count explodes, the coordination overhead compounds, and the small marketing team that owned a tidy 5-page strategy now owns a sprawling content liability.
What breaks first is content uniqueness. Templated location pages get cloned across the footprint, provider bios duplicate across sites where clinicians float between offices, and service descriptions drift out of sync with what each clinic actually offers. Reviews concentrate on the flagship while satellite locations stay invisible. Google Business Profiles fall out of date because no one owns them at the data layer.
The underlying problem is not tactic selection. It is execution architecture. Healthcare SEO at scale is a production engineering problem disguised as a marketing problem, and the ten tips below treat it that way — each one evaluated for how it holds up when location count moves from 3 to 30 to 300.
Treat Location Pages as Production Engineering, Not Copywriting
Location pages fail in multi-location healthcare for one reason: teams treat them as writing projects. A copywriter handles the first ten, a freelancer drafts the next twenty, an intern fills the spreadsheet for the remaining sixty. By month nine, the portfolio holds 90 pages with overlapping service descriptions, mismatched hours, and provider lists that no longer reflect who actually works where.
The fix is to model location-page output the way healthcare organizations model clinical guideline rollout. An overview of implementation research in healthcare settings identified 36 systematic reviews covering 30 distinct strategies, with audit and feedback, reminders, educational meetings, and care pathways emerging as the patterns that consistently produce reliable execution across sites 9. Marketing operations needs the same scaffolding. Each location page should pass through a defined pipeline with required inputs (provider roster, service line confirmation, insurance acceptance, local landmarks, parking and access notes), a content module library, a medical accuracy checkpoint, and a publishing audit that flags drift against the source of truth.
Uniqueness emerges from the input data, not from rewording boilerplate. A page for an urgent care clinic in a college town pulls different service emphasis, hours, and proximity references than the same chain's location in a retirement-heavy suburb — even though the underlying template is identical. The page-level differentiation comes from structured local inputs, not from a writer rewriting the same paragraph 40 ways.
Teams that ship 200 defensible location pages run a production line. Teams that ship 200 thin pages ran 200 separate writing assignments.
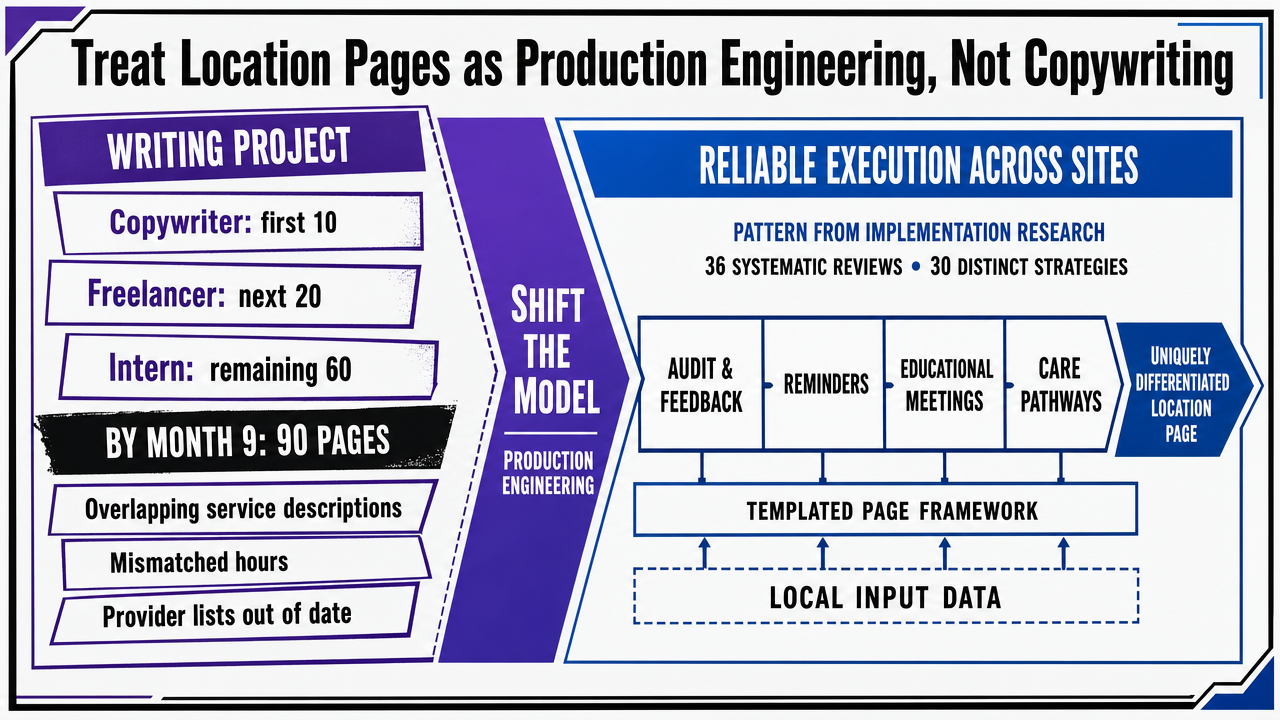 Visualize the structured production pipeline that turns a templated location page into a uniquely differentiated asset using local input data, directly supporting the section's argument
Visualize the structured production pipeline that turns a templated location page into a uniquely differentiated asset using local input data, directly supporting the section's argument
Build Provider E-E-A-T as a Portfolio Asset, Not a Page-Level Afterthought
Provider expertise is the highest-leverage trust signal a healthcare brand controls, and most multi-location operators waste it. The typical pattern: a single bio paragraph copied from a credentialing PDF, dropped on a location page, never updated, never cross-linked, never extended into long-form authored content. At 8 locations this is a missed opportunity. At 80, it is a compounding loss.
The fix is to treat each provider as a structured entity in a portfolio-wide system, not as page-level decoration. A provider record holds verifiable inputs — medical school, residency, board certifications, NPI, years in specialty, languages, conditions treated, procedure volumes where appropriate, and the locations where the clinician actually practices. That record powers the bio module on every location page where the provider appears, a dedicated provider page with its own URL and schema, and authored content tied to the provider's expertise areas.
The evidence on patient choice supports the investment. A peer-reviewed analysis of what drives provider selection found that review valence and trust signals significantly affect patient decisions, with effects most pronounced for higher-risk conditions 2. Verifiable provider detail is the trust input that scales — it does not depend on review volume, and it survives algorithmic skepticism of thin healthcare content far better than templated service copy.
Operationally, the unlock is governance. One owner maintains the provider data layer. Location pages, provider pages, and authored articles read from it. When a clinician moves between sites, the change propagates everywhere in one update rather than triggering forty manual edits.
Prioritize Content Using Patient Experience Data, Not Keyword Volume Alone
Keyword volume tells a healthcare marketing team what people search. Patient experience data tells the team what those searchers actually struggle with once they arrive. The second input is usually the better content prioritization signal for a multi-location portfolio, and most SEO leads under-use it.
HCAHPS, the standardized national survey of hospital patient perspectives, exists precisely because patient experience contains structured, comparable signal about what care feels like across sites 3. AHRQ's guidance on the CAHPS family of surveys recommends using results to identify the specific experience gaps a given location should address and to direct improvement resources accordingly 4. That same logic transfers cleanly to content prioritization. The questions patients raise in experience surveys — wait times, communication clarity, appointment access, billing transparency, post-visit instructions — map directly to the FAQ blocks, service-page sections, and provider-page modules that win informational queries in local search.
The operational pattern is straightforward. A regional orthopedic group with 24 clinics pulls its experience data by location, identifies the two or three friction points each site scores worst on, and routes those topics into the location-page content backlog for that specific clinic. A site flagged for poor communication around post-surgical recovery gets a clinician-authored recovery timeline module. A site flagged for scheduling friction gets a structured access and intake section.
A systematic review of patient satisfaction measurement found that determinants vary by setting and population, which is why portfolio-wide content templates miss 1. Experience data localizes the priority list. Keyword tools cannot do that.
Test Multi-Location Healthcare SEO Execution Live
Experience real-time SEO optimization and publish actual content for your healthcare locations during your free trial.
Reviews Measure Experience, Not Clinical Quality — Plan Accordingly
Reputation strategy in healthcare runs on a contradiction most marketing teams never name out loud. Reviews matter enormously for patient acquisition, and reviews are a poor measure of the thing patients think they are measuring.
Both claims have evidence. A peer-reviewed analysis of provider choice found that review valence and trust signals significantly affect which clinician a patient selects, with the effect most pronounced for higher-risk conditions where the decision carries real consequence 2. At the same time, a Brookings analysis of medical provider reviews concluded that what patients actually rate is bedside manner, office decor, staff demeanor, and the texture of the visit — not the clinical quality of the care delivered 8. A separate university research summary reached the same conclusion: online physician reviews do not reliably indicate the quality of care a clinician provides 5.
For a multi-location operator, that tension changes how the reputation program gets built. The goal is not to chase clinical-quality signaling through star ratings, because the channel cannot carry that load. The goal is to engineer the experience signals reviews actually capture — front-desk responsiveness, wait-time communication, staff warmth, facility condition, post-visit follow-up — and let the reviews reflect what the locations genuinely deliver.
That reframing also clarifies what content claims a location page can defensibly make. Pages can showcase verified credentials, procedure volumes, and accepted insurance with confidence. Claims that lean on aggregate star averages to imply clinical superiority overpromise on what the underlying signal supports. A 40-clinic dental group with 4.8 stars across the portfolio is telling search engines and patients that its locations are pleasant places to receive care. That is a real and valuable claim. It is not the same claim as superior clinical outcomes, and the content should not blur the line.
The operational consequence is straightforward: reputation programs at scale should be staffed and measured against experience inputs the locations control, with content claims calibrated to what reviews actually measure.
Engineer Review Velocity Across Owned and Third-Party Channels
Review volume is a distribution problem before it is a content problem. A 60-clinic primary care group does not need a clever ask script. It needs every site collecting at a steady weekly rate across the channels patients actually consult, with the flagship locations not absorbing all the volume.
The channel mix matters because the channels disagree. A hospital-based study comparing provider-initiated surveys with independent review sites found a higher number of reviews and more favorable ratings on hospital-owned channels than on third-party platforms 7. Patients researching a clinician check both, and Google's local pack rewards third-party signal that the brand cannot directly stage. A program that only pumps reviews into the owned site builds a lopsided portfolio that search engines and prospective patients discount.
The operating pattern at scale is per-location velocity targets across at least two channels — the Google Business Profile for each site and a relevant third-party platform — with a centralized request system that hands off to local staff at the moment of care. Post-visit SMS triggers from the EHR, kiosk prompts at checkout, and discharge-instruction emails are the workhorses. Centralization owns the trigger logic, deliverability, and reporting. Locations own the patient interaction that earns the review.
Two governance rules keep the program defensible: no gating reviews by predicted sentiment, and no incentives. The growth happens at the site level, on real experiences, distributed across the channels patients trust.
Mine Review Text as a Content and Quality-Improvement Input
Star ratings are the wrong layer of review data to mine. The narrative text underneath holds the actual signal. A peer-reviewed analysis of online hospital reviews trained machine-learning models on review text and reported 99% accuracy predicting overall HCAHPS scores and 93% to 99% accuracy predicting relevance to seven domains of patient experience 11. Reviews carry structured information about communication, responsiveness, environment, and post-visit experience — the same dimensions that drive informational search behavior in healthcare.
That makes review text a dual-purpose input. For content, the recurring phrases patients use at a specific site reveal the exact wording, concerns, and comparisons that should appear in that location's FAQ, service-page modules, and provider-page Q&A. A pediatric urgent care chain whose reviews in three suburban markets cluster around weekend wait times and insurance verification has its content roadmap for those sites written for it.
For quality improvement, the same text routes back to operations. A site where reviews repeatedly flag billing communication gives the local team a defined experience problem to fix, which then changes the inputs the next batch of reviews captures. Mining the text closes a loop that star averages alone cannot.
Hold NAP and Google Business Profile Consistency at the Data Layer
Name, address, and phone consistency stops being a checklist item somewhere around the fifteenth location. Past that point, no spreadsheet survives the weekly drift of suite number changes, after-hours line swaps, holiday closures, and clinicians rotating between sites. A 120-clinic dialysis network that manages NAP at the listing level is already losing the battle. The only durable fix is moving the source of truth one layer up — into a structured data system that publishes outward to every listing, location page, schema block, and directory feed.
The pattern mirrors how healthcare organizations sustain other multi-site standards. An overview of clinical implementation research found that reminders, audit and feedback, and care pathways were among the strategies that produced reliable execution across organizational settings 9. Marketing operations needs the analog: a canonical record per location, automated audits that flag mismatches between the record and what is live on Google Business Profile, Healthgrades, Yelp, and the location page itself, and a publishing pipeline that pushes corrections rather than relying on a coordinator to chase them.
One owner holds the data. Every downstream surface reads from it. NAP consistency then becomes a system property, not a quarterly cleanup project.
Coordinate SEO Across Locations With Data-Driven Precision
Connect with specialists to see how enterprise-grade automation and cross-location SEO orchestration can streamline execution for complex healthcare organizations.
Use Structured Service Comparisons to Match How Patients Decide
Patients shopping for care behave like patients shopping for coverage. Federal guidance on plan selection frames the decision as one that gets easier once a few concrete factors are lined up side by side 10. Healthcare search pages should mirror that behavior. The location and service pages that win informational queries present structured comparisons — accepted insurance, in-network status, same-day availability, telehealth versus in-person, procedure scope, language support — rather than paragraphs of undifferentiated prose.
The multi-location wrinkle is that each comparison field has to vary by site and stay accurate. A 30-clinic women's health group cannot publish one insurance list and call it done. Site A accepts a payer that Site B does not. Site C offers a procedure Site D refers out. Templated comparison blocks fed from a per-location data source solve this; hand-edited tables do not survive past the first credentialing change.
Structured comparisons also feed schema. Service offerings, accepted insurance, and procedure availability map cleanly to markup that local search rewards. The patient sees a clear decision aid. The crawler sees machine-readable inputs that distinguish one location from the next.
Deploy Schema and Internal Linking as a Portfolio System
Schema markup and internal linking are usually treated as one-off page tasks. At portfolio scale, both should function as systems that generate themselves from the same structured data that powers location pages, provider records, and service comparisons.
The schema side starts with MedicalOrganization or MedicalClinic markup per location, with nested Physician entities, MedicalProcedure offerings, accepted insurance via healthPlanNetwork, and explicit geo coordinates. Each field reads from the canonical record described earlier — provider data, NAP, service availability — so the markup updates automatically when the underlying data changes. A 50-clinic cardiology group should not be hand-editing JSON-LD blocks. The same governance pattern that produces reliable execution across healthcare sites — reminders, audit and feedback, structured pathways 9— applies to markup integrity audits running against the live pages.
Internal linking follows the same logic. Provider pages link to every location where the clinician practices. Location pages link to the providers who see patients there, the services offered at that site, and the city-level service hub. Service pages link to the specific locations where the service is available. The link graph encodes which providers, services, and sites belong together as a machine-readable map of the portfolio — not a coincidence of which writer happened to remember to add a link.
Pick a Production System: In-House, Agency, or AI Platform
The first nine tactics describe the work. This one decides who does it. Multi-location healthcare SEO at 30 or 300 sites is bottlenecked by execution capacity, not strategy, and the production model a team picks determines whether the playbook survives contact with the location count.
Three models dominate. An in-house team holds institutional knowledge and moves fast on brand-specific judgment calls, but FTE cost varies by market, and headcount has to grow roughly in step with portfolio complexity. A traditional agency on retainer brings outside specialist capacity, but most agency commercial models scale with site count — per-location retainers, per-page content fees, and per-listing management charges — so the cost line tracks the footprint and the coordination overhead grows with every handoff between the brand, the account manager, and the production staff. An AI marketing platform shifts the unit economics by operating at the account level rather than per location, with the same plan covering every site, service line, and provider record under one program. The Vectoron platform, as one example in this category, runs at $599/month following a two-week trial, with strategy, content, technical SEO, and reporting handled across the full footprint rather than billed per site.
The comparison below uses transparent variables for the inputs no public benchmark reliably captures.
| Dimension | In-House Team | Traditional Agency (Retainer) | AI Marketing Platform |
|---|---|---|---|
| Cost structure | Fixed FTE cost; varies by market and seniority | Monthly retainer, often with per-location or per-page fees | Flat account-level subscription (Vectoron: $599/month post-trial) |
| Scaling behavior with location count | Headcount grows with portfolio complexity | Cost typically scales linearly with site count | Cost holds flat as locations are added under one account |
| Coordination overhead | Low internally; high cross-functional load on marketing lead | Brand–agency handoffs, account-manager layer, approval cycles | Centralized approval workflow; production runs from one data layer |
| Time-to-publish per location page | Constrained by team capacity and queue depth | Constrained by agency SLA and revision rounds | Constrained by approval throughput rather than writer availability |
No model is universally right. A 6-clinic specialty group with a tenured marketing lead may run leanest in-house. A 200-site primary care network with thin internal capacity will find per-location agency math punishing. The decision rule that matters: pick the model whose cost and coordination curves stay flat as the next 20 locations come online, because they will.
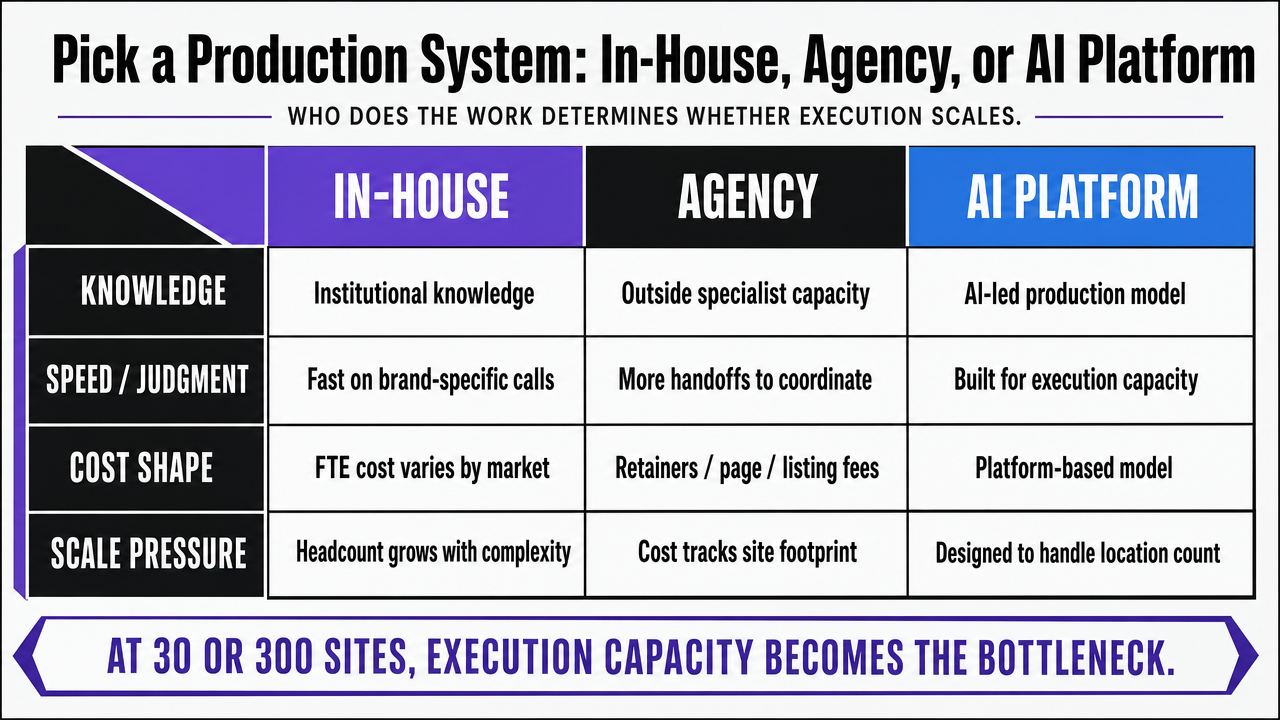 Render the in-text comparison table as a clean side-by-side comparison infographic so readers can scan the three production models against the four dimensions discussed in the section
Render the in-text comparison table as a clean side-by-side comparison infographic so readers can scan the three production models against the four dimensions discussed in the section
Measure What Actually Moves Patient Acquisition
Most multi-location healthcare SEO dashboards report on the wrong layer. Keyword rankings, domain authority, and aggregate organic sessions describe activity, not outcomes. The metrics that correlate with patient acquisition operate at the location and service-line level, and a portfolio program that does not report on them is flying on proxies.
Three measurement tiers earn their place. The first is location-level booked appointment volume from organic and local search, segmented by new versus returning patients and tied back to landing page and Google Business Profile entry points. The second is service-line conversion rate by site, which surfaces which locations convert search traffic into scheduled visits and which leak qualified intent at the form or call step. The third is the patient-experience signal already discussed — review velocity, sentiment by topic, and the experience domains review text predicts with high accuracy 11— read as a leading indicator of what the next quarter of acquisition will look like.
AHRQ's guidance on prioritizing patient-experience improvement applies directly: results should drive where the next resources go 4. A 50-site portfolio that reports acquisition by location, isolates the bottom-quartile sites, and routes content, listings, and experience fixes to those specific clinics will outperform one that optimizes the brand average. The portfolio average hides the locations that are actually losing patients.
Frequently Asked Questions
References
- 1.Patient Satisfaction with Healthcare Services and the Techniques to Measure It: A Systematic Review.
- 2.Choosing a Provider: What Factors Matter Most to Consumers and Do Preferences Align With Those of Providers?.
- 3.HCAHPS: Patients' Perspectives of Care Survey - CMS.
- 4.Section 5: Determining Where To Focus Efforts To Improve Patient Experience.
- 5.Researchers Examine if Online Physician Reviews Indicate Clinical Quality.
- 6.Can online doctor reviews be trusted?.
- 7.Study Finds Discrepancy in Reporting of Doctor Reviews.
- 8.Online reviews of medical providers: Take them with a grain of salt.
- 9.Strategies for the implementation of clinical practice guidelines in healthcare organizations: an overview of systematic reviews.
- 10.3 things to know before you pick a health insurance plan.
- 11.Using Online Reviews to Drive Person-Centered Care: An HCAHPS ....