
Key Takeaways
 Respondents who considered hospital ownership relevant to their care decisions
Respondents who considered hospital ownership relevant to their care decisions
Respondents who considered hospital ownership relevant to their care decisions
- Patient hospital choice consistently hinges on five factors: quality of care, distance, waiting times, staff attitude, and reputation, yet most keyword inventories overweight procedure terms and miss the other four 11.
- Ownership labels like nonprofit or academic deserve minimal real estate since only 29.0% of U.S. adults say ownership status has ever influenced their care decisions 5.
- Keyword clusters should follow journey stages, with symptom and recovery pillars at the system level, procedure content at the service-line level, and only location-specific answers on site pages 9.
- Multi-location systems running per-site retainers cannibalize their own rankings; an account-level execution model assigns intent to one canonical page and resolves the duplicate-content drag 3.
Why most hospital keyword lists miss the patient
Most hospital keyword strategies start with the wrong question. Teams ask which terms have search volume, then they sort those terms by service line and assign them to location pages. The resulting spreadsheet looks comprehensive. It rarely reflects how patients actually search, decide, or convert.
A systematic review of survey studies on hospital choice found that patients consistently cite five factors when picking a facility: quality of care, distance, waiting times, staff attitude, and reputation 11. None of those map cleanly to the institutional vocabulary that fills most hospital sitemaps. A separate systematic review on publicly available quality information reached an even sharper conclusion: patients rarely use the technical quality data hospitals publish as a primary decision input, despite years of transparency policy aimed at making that data accessible 2.
Search engines remain the dominant starting point for health information seeking, a pattern that has held across more than a decade of survey data 8. That means the gap between what hospital teams optimize for and what patients query is not a small leak. It is the entire funnel.
This article reframes hospital keyword strategy around documented patient decision behavior, journey-stage intent, and the multi-location execution problem that makes per-site keyword planning break down at scale.
What patients actually weigh when choosing a hospital
The five recurring decision factors
A systematic review of survey studies on hospital choice consolidated decades of patient-reported data and surfaced a consistent hierarchy. Five factors recur across studies: quality of care, distance from home, waiting times, staff attitude, and hospital reputation 11. The ranking shifts by population and procedure type, but the five themes appear with enough regularity to function as a keyword prioritization map.
Quality of care is the loudest stated preference, yet patients translate it into lay terms. They search for phrases like "best hospital for heart surgery near me" rather than risk-adjusted mortality indices. Distance shows up as "near me," ZIP code modifiers, and neighborhood names. Waiting times surface as "ER wait time," "same-day appointment," and "urgent care vs ER" comparisons. Staff attitude generates queries about specific physicians, nurse reviews, and bedside manner. Reputation overlaps with brand searches, ranked-list queries, and "top-rated" modifiers.
Keyword inventories built from service-line taxonomies miss most of this surface area. A cardiology page targeting "coronary artery bypass graft" captures clinical intent but leaves the four other documented decision factors uncovered. A more accurate architecture assigns keyword themes to each of the five factors and tracks coverage gaps the way ops teams track open beds.
The review authors caution that survey responses can diverge from actual behavior 11. Stated preferences still set the floor for content themes because they describe what patients say out loud when typing into a search box.
The ownership keyword trap
Hospital marketing teams spend disproportionate effort on institutional-identity keywords: "nonprofit hospital," "academic medical center," "faith-based hospital," "teaching hospital." The patient-side data does not support that allocation.
A 2023 survey of U.S. adults found that only 29.0% indicated hospital ownership status had ever been relevant to their decision about where to seek care 5. The remaining 71% treated ownership as background information at most. Relevance was higher among respondents with lower health literacy, which is a meaningful subgroup signal but not a mandate to lead the sitemap with ownership language.
The strategic read is straightforward. Ownership-type keywords belong on About pages and trust-building content where they reinforce credibility for patients who care. They do not belong on landing pages competing for procedure or symptom intent, where they crowd out the patient-language terms that actually drive clicks. A page titled "Nonprofit Academic Cardiac Surgery Program" is solving for a board narrative. A page titled "Heart Bypass Surgery: Recovery Time, Risks, and What to Expect" is solving for a patient at 11 p.m. trying to understand what their cardiologist just said.
Reallocating that real estate to journey-stage themes is the single highest-leverage move most hospital keyword inventories have available.
Quality-data keywords: high stated value, low actual use
Quality-outcome keywords sit in a more complicated position. A national evaluation of patient preferences for elective surgery selection found that 82% of respondents said they would use at least one type of quality information when picking a hospital, with mortality rates, complication rates, hospital-acquired infection rates, and surgeon volume ranking as the most frequently selected measures 10. That is a strong stated-intent signal, especially for high-stakes elective procedures like joint replacement, cardiac surgery, and oncology.
The complication is that a separate systematic review of how patients actually use publicly available quality information reached the opposite finding in practice. Patients rarely use such data as a primary decision factor despite years of transparency policy and public reporting efforts 2. The same study on directing patients to high-volume hospitals reinforced that simply publishing performance metrics online is insufficient to change hospital choice 1.
The keyword-strategy implication is a tiered priority. Quality-outcome terms deserve dedicated content for elective surgery service lines, where stated intent is highest and the search funnel includes longer comparison phases. They warrant lighter investment for emergency and acute care service lines, where distance and wait-time terms dominate actual behavior. Treating all service lines as equally quality-data-driven misreads the evidence in both directions: it underweights elective surgery and overweights everything else.
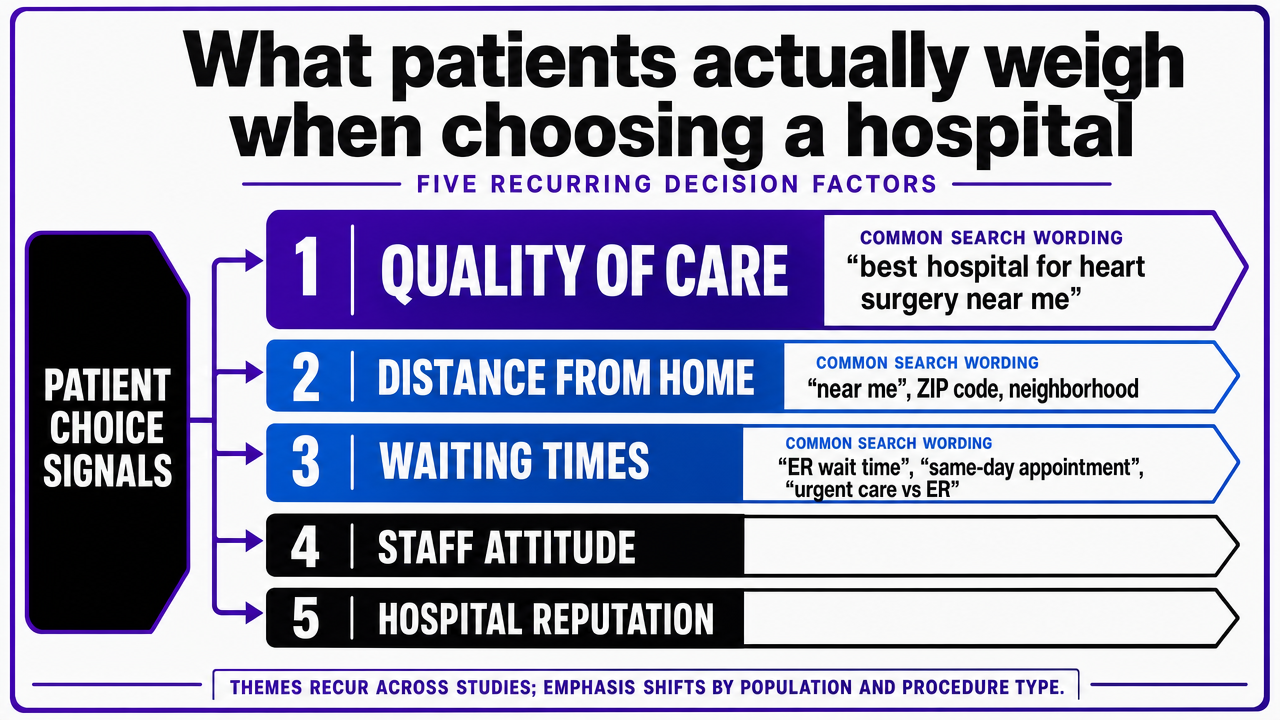 Visualize the five recurring patient hospital-choice factors cited from the systematic review, giving readers a scannable framework for keyword prioritization
Visualize the five recurring patient hospital-choice factors cited from the systematic review, giving readers a scannable framework for keyword prioritization
A journey-stage architecture for keyword clusters
Symptom and condition queries at the front of the journey
Patient search activity rarely begins with a hospital name. It begins with a body. A systematic review of online information-seeking behavior among patients with chronic conditions found that the most common search topics include symptoms, treatment options, side effects, and prognosis, almost always phrased in lay language rather than clinical terminology 12. Someone with new chest tightness types "chest pressure when walking" before they ever type "stable angina," and they type either of those before they type the name of a cardiology program.
This front-of-funnel layer is where most hospital sites underperform. Service-line pages skip past symptom intent and land directly on treatment descriptions, which leaves the highest-volume queries to WebMD, Healthline, and Mayo Clinic's consumer content. Patient journey mapping research identifies pre-visit information needs as a distinct decision point with its own questions, anxieties, and triggers 9. Hospitals that treat symptom content as below their clinical altitude forfeit that decision point.
A workable cluster at this stage pairs symptom phrases with the conditions they commonly indicate and the specialty that treats them. "Sharp pain in lower right abdomen" connects to appendicitis, which connects to emergency surgery. "Numbness in fingers at night" connects to carpal tunnel, which connects to orthopedic hand specialists. The keyword inventory should treat the symptom-to-specialty bridge as an explicit content asset, not an SEO accident.
Procedure and treatment comparison queries
Once a condition has a name, the search behavior shifts from diagnostic to comparative. Patients researching chronic conditions consistently look for treatment options, side effects, and provider details before committing to a path 12. The queries at this stage carry modifiers like "vs," "recovery time," "success rate," "alternatives to," and "is it worth it."
This is also where quality-outcome keywords earn their priority. The national evaluation of elective surgery preferences found that mortality rates, complication rates, hospital-acquired infection rates, and surgeon volume topped the list of measures patients said they would consult 10. A page on "robotic prostatectomy vs open prostatectomy" that integrates outcome data alongside recovery and side-effect discussion does double duty: it captures comparison intent and surfaces the quality signals that elective-surgery patients ask for, even if they often default to other factors at the moment of choice 2.
The cluster shape matters here. A single pillar page per major procedure, supported by satellite pages on alternatives, risks, recovery, and cost questions, outperforms a flat list of procedure names. The pillar absorbs broad terms. The satellites catch the long-tail comparison queries that signal a patient actively narrowing options.
Provider, location, and booking queries
The intent collapses sharply once a patient has chosen a procedure or specialty. Queries shorten and pick up geographic, scheduling, and provider modifiers: "orthopedic surgeon near me," "same-day mammogram [city]," "book pediatric appointment," "[physician name] reviews." Patient journey research positions this as the conversion-adjacent stage where the information need flips from learning to acting 9.
The systematic review of hospital website evaluation models identified find-a-doctor, find-a-location, and appointment-booking as core user tasks that determine whether a site converts the traffic it earns 3. Keyword work at this stage should map directly onto those tasks. Provider pages need physician names, sub-specialties, languages spoken, insurance accepted, and location attached. Location pages need driving directions, parking, ER wait times, and the specific services available at that site, not a copy-paste of the system's full service catalog.
Two patterns sabotage this stage. The first is the generic provider directory that ranks for a doctor's name but answers none of the questions that prompted the search. The second is the location page that recites a mission statement before listing services. Both treat high-intent traffic as if it were still browsing. The architecture should compress steps between query and booking action, not pad them.
Post-visit recovery and follow-up queries
The journey does not end at discharge, and neither does the keyword opportunity. Patient journey mapping identifies post-visit information needs as a distinct phase with questions about recovery timelines, medication side effects, warning signs, and follow-up logistics 9. Chronic-condition research confirms that side-effect and prognosis queries continue well after the initial diagnosis or procedure 12.
Hospitals that own this content layer earn two compounding returns. The first is loyalty: a patient who finds their own hospital's recovery guide ranks the institution higher on the next decision. The second is acquisition from outside the patient base. "What to expect after gallbladder surgery" pulls in searchers who had their procedure elsewhere and are now evaluating where to take their next concern.
Cluster examples include recovery timelines by procedure, when-to-call-your-doctor checklists, medication interaction guides, and rehabilitation expectations. These pages also feed the symptom layer at the top of the funnel, closing the loop in the keyword architecture.
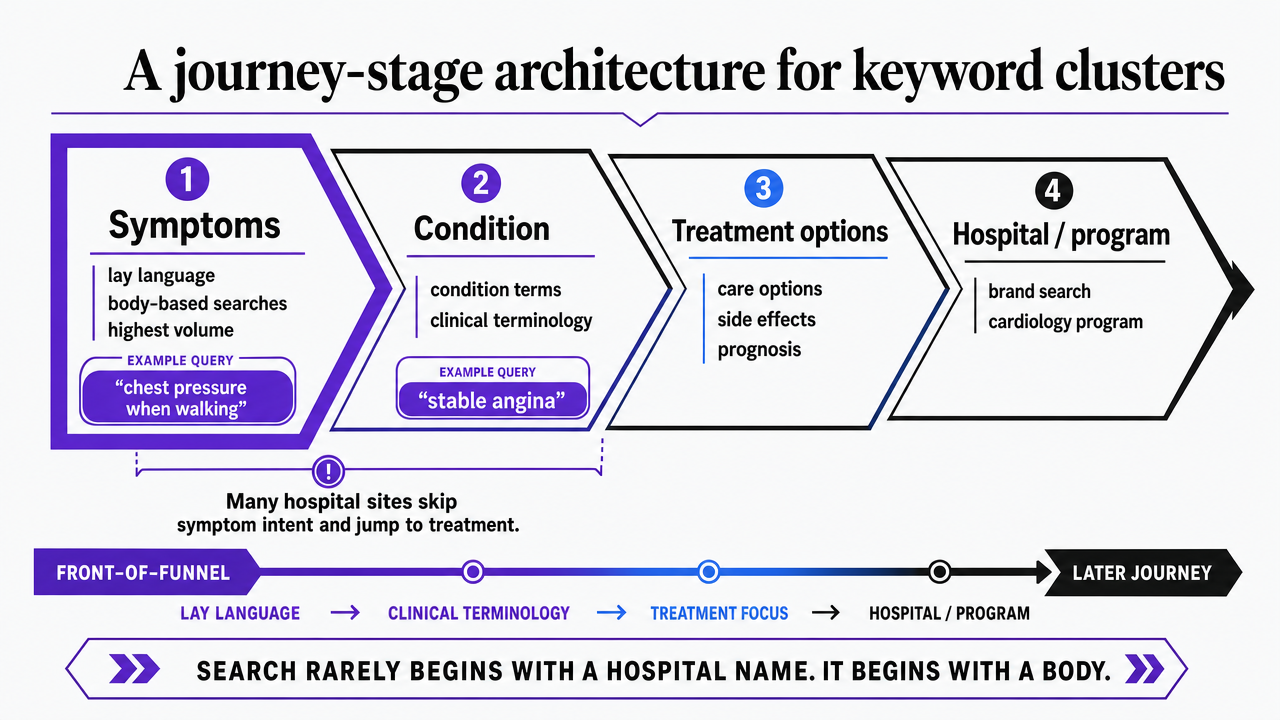 Map keyword cluster types to the four patient journey stages described in the section, reinforcing the architecture readers should adopt
Map keyword cluster types to the four patient journey stages described in the section, reinforcing the architecture readers should adopt
Test hospital SEO keywords in live campaigns today
Launch hospital keyword-driven campaigns and measure real patient acquisition results in your first week.
Patient language, not clinical language
The gap between how clinicians label conditions and how patients describe them is one of the most expensive translation problems in hospital SEO. A systematic review of chronic-condition information-seeking found that patients overwhelmingly search in lay vocabulary, looking up symptoms, treatment options, side effects, and prognosis using the words they use at the kitchen table, not the ICD-10 codes their chart will eventually carry 12. Someone types "why does my knee click when I bend it," not "patellofemoral crepitus." They type "can't sleep flat" before "orthopnea."
Hospital content that leads with clinical nomenclature surrenders the top of the funnel. Service-line pages titled with procedure codes or formal diagnostic terms rank against other clinical content, mostly other hospitals and journal abstracts, instead of against the consumer-health sites that actually capture patient queries. The fix is not to dumb down the medicine. It is to lead each page with the patient phrasing, then introduce the clinical term as a synonym a paragraph in.
This is also where HCAHPS-aligned experience language earns its place. Patient-experience domains like communication with nurses, responsiveness of staff, and a quiet environment map to queries patients actually type when comparing facilities 13. "Hospital with private rooms" and "doctors who explain things clearly" are keyword themes, not soft marketing copy.
The readability tax on keyword-rich content
Optimizing for search and optimizing for patient comprehension pull in opposite directions more often than most content teams admit. A 2024 study of diabetic retinopathy web pages found that many sites ranking well in search results were written above recommended reading levels for patient materials, even as they hit standard SEO targets 6. The pages got found. The patients who landed on them could not parse what they said.
The cost shows up downstream. A reader who bounces off a procedure page because the prose reads like a discharge summary does not book an appointment. They click back to the results and pick the next listing, which is often a consumer-health publisher with cleaner sentences and weaker clinical authority. The hospital traded a ranking signal for a conversion loss.
A workable rule is to write the first 200 words of any condition or procedure page at a 9th-grade reading level, introduce clinical terms as glosses rather than headers, and reserve dense technical content for collapsible sections or linked deeper pages. Keyword density follows the language patients use, not the language the chart uses. The page can still satisfy crawler signals through structured data, internal linking, and headers that mirror question-format queries.
See Hospital SEO Keyword Data That Informs Patient Acquisition Strategy
Request a custom report of high-conversion hospital SEO keywords, volume metrics, and competitive benchmarks designed for multi-location healthcare brands and agency teams managing complex footprints.
If you manage multiple locations: account-level keyword execution
Where per-location SEO retainers break down
For systems running three or more sites under one brand, the keyword problem changes shape. It stops being about which terms to target and starts being about how to keep twelve location pages from competing with each other for the same query.
Per-location SEO retainers were built for a different operating reality. Each site gets its own keyword list, its own content calendar, and its own agency contact. The cardiology page in Site A and the cardiology page in Site B end up optimized for nearly identical procedure terms, with geographic modifiers as the only meaningful differentiator. Google sees two pages from the same domain chasing the same intent and splits authority between them, which is the textbook definition of cannibalization. Research on hospital website evaluation has long flagged duplicate and overlapping content as a structural weakness in multi-site systems, since it degrades the usability and content-quality dimensions that determine whether searchers complete core tasks like finding a provider or booking care 3.
The coordination tax is the second drag. Every service-line launch, every physician hire, every facility expansion has to be re-briefed to each location's content team. Production cycles stretch. Symptom and recovery content, which the journey research identifies as the highest-leverage front-of-funnel layer 9, gets deferred because no single location owns it.
A consolidation comparison for multi-site systems
An account-level keyword model treats the entire footprint as one inventory and assigns intent to the right page rather than duplicating it across every page. Symptom and condition pillars live once at the system level, where they pull traffic from the full geographic catchment. Location pages carry only the queries that actually require a location answer: wait times, parking, accepted insurance, on-site services, and provider rosters. Procedure pillars sit at the service-line level and route to the nearest qualified site through structured location modules. The architecture matches how search engines already weight authority and how patients already search 8.
The economics are easier to compare when framed as variables rather than invented dollar figures.
| Cost and output driver | Per-location retainer model | Account-level execution model |
|---|---|---|
| Monthly spend | L locations × per-site retainer | Single account-level program covering L locations |
| Content production cycles | L parallel queues, separately briefed | One queue, one brief, routed assets |
| Cannibalization risk | High: duplicate procedure pages across sites | Low: intent assigned to one canonical page |
| Coordination handoffs per asset | One per location agency contact | One per approval cycle |
| Symptom and recovery coverage | Often deferred, no single owner | Owned at the system level |
Platforms like Vectoron are built around that account-level execution model, which lets a system run one keyword inventory across every site and service line instead of paying L times for L versions of the same plan.
Operator implications for the next planning cycle
The work for the next planning cycle is not another keyword refresh. It is a re-architecture of the inventory against documented patient behavior. Three moves carry most of the weight.
- First, audit the existing keyword map against the five recurring patient-choice factors: quality of care, distance, waiting times, staff attitude, and reputation 11. Most inventories overweight procedure terms and underweight wait-time, staff, and experience themes that HCAHPS domains describe in patient language 13. Coverage gaps in those four themes are usually larger than gaps in the procedure catalog.
- Second, reassign content ownership by journey stage rather than by service line. Symptom and recovery pillars belong at the system level, where they pull from the full catchment and feed the procedure pages that sit beneath them 9. Procedure and provider content belongs at the service-line level. Only wait times, parking, on-site services, and provider rosters belong at the location level.
- Third, run the inventory through one execution queue instead of L parallel ones. Account-level marketing operating systems, including platforms like Vectoron, were built for this shape of work: one keyword plan, one production cycle, one approval surface across every site and service line. The savings are not theoretical. They are the duplicate pages that stop competing with each other and the symptom content that finally gets written.
Frequently Asked Questions
References
- 1.How to direct patients to high-volume hospitals.
- 2.The use of publicly available quality information when choosing a hospital for elective hospitalisation: Systematic review.
- 3.Evaluation models and criteria of the quality of hospital websites: A systematic review.
- 4.Applying Website Rankings to Digital Health Centers in the United States.
- 5.Public perceptions of US for-profit, nonprofit, and public hospitals.
- 6.Search engine optimization and its association with readability and quality of online information on diabetic retinopathy.
- 7.Online Health Information Seeking Behavior: A Systematic Review.
- 8.Evolving Health Information–Seeking Behavior in the Context of Digital Platforms.
- 9.Understanding Patient Journey Mapping in Healthcare: An Exploratory Study.
- 10.National Evaluation of Patient Preferences in Selecting Hospitals for Elective Surgery in the United States.
- 11.What factors do patients consider important when choosing a hospital? A systematic review of survey studies.
- 12.Information needs and online information-seeking behaviour of patients with chronic conditions: a systematic review.
- 13.Hospital CAHPS (HCAHPS) Survey.