Building a Scalable Medical Content Marketing Engine
Why Medical Content Engines Must Scale Now
Multi-location healthcare operators face an intensifying patient acquisition challenge: competitors with coordinated digital strategies are capturing market share in local search results while fragmented content approaches leave service lines underrepresented across geographic footprints. The underlying constraint is volume. Healthcare systems operating across multiple locations confront a mathematical reality that traditional content development models cannot address—a single orthopedic practice managing 12 locations across three states requires approximately 144 unique service pages, 48 location-specific landing pages, and 96 physician profile pages before publishing a single blog article. Manual creation timelines make this footprint operationally impossible to maintain at the cadence competitive markets demand.
Research from the Healthcare Content Marketing Association indicates that healthcare organizations publishing 16 or more pieces of content monthly generate 3.5 times more qualified leads than those publishing fewer than four pieces. Distributed healthcare operators face an amplified version of this requirement: each location needs localized content addressing regional patient demographics, competitive positioning, and service-specific search intent. A dermatology group with eight locations competing in markets where competitors publish 12 articles monthly must produce 96 location-optimized articles to maintain parity—an output requiring 12 full-time content specialists under traditional agency models. The volume gap translates directly to visibility disadvantage in organic search rankings where publication frequency determines algorithmic authority.
The economic constraint becomes acute when factoring creation costs against patient acquisition targets. Healthcare systems typically allocate 6-8% of revenue to marketing operations, with content development consuming 30-40% of that budget. Traditional agency relationships bill per location or per piece, creating cost structures that scale linearly with footprint expansion. A cardiology practice adding its sixth location faces a 20% increase in content costs despite marginal increases in administrative overhead—a pricing model that penalizes geographic growth precisely when patient acquisition returns should improve through operational leverage.
Content velocity directly impacts search visibility in competitive healthcare markets. Analysis of 2,400 healthcare websites by BrightEdge Research found that organizations publishing weekly content across all service lines captured 67% more organic search impressions than those updating quarterly. Geographically dispersed operators cannot achieve this cadence through manual workflows when each piece requires medical accuracy review, local optimization, and compliance verification across multiple regulatory frameworks. The competitive disadvantage compounds over time as rivals build content libraries that dominate local search results across service categories.
Healthcare marketing leaders managing complex service footprints require publishing infrastructure capable of maintaining consistent output across 15-30 locations without proportional increases in oversight burden or agency spend. The strategic imperative is clear—content systems must scale to match operational footprint. The operational question becomes how publishing infrastructure can execute at required volumes while maintaining clinical accuracy, local relevance, and compliance standards across distributed healthcare operations.
Core Pillars of a Scalable Content System
Evidence-Based Clinical Content Standards
Assessment Tool: Clinical Content Quality Self-Audit- Does each content asset reference current, peer-reviewed clinical guidelines?- Are clinician contributors integrated into approval workflows for all condition-specific materials?- Is every patient-facing statement reviewed for accuracy and updated when guidelines change?- Are outcome metrics, such as knowledge gains or adherence rates, tracked by content type and channel?- Is there a process for promptly correcting or retracting inaccurate or outdated information?
 Evidence-Based Clinical Content Standards
Evidence-Based Clinical Content Standards
A scalable medical content marketing engine depends on rigorous, evidence-based clinical content standards. These standards require that all educational materials be anchored in up-to-date, peer-reviewed guidelines and reflect the consensus of clinical subject matter experts. Research highlights that therapeutic patient education (TPE) programs structured around repeatable, evidence-based content yield significant improvements in both biomedical and psychosocial outcomes for chronic disease patients 1. This approach is ideal for multi-location healthcare systems that must maintain both consistency and clinical accuracy across distributed teams.
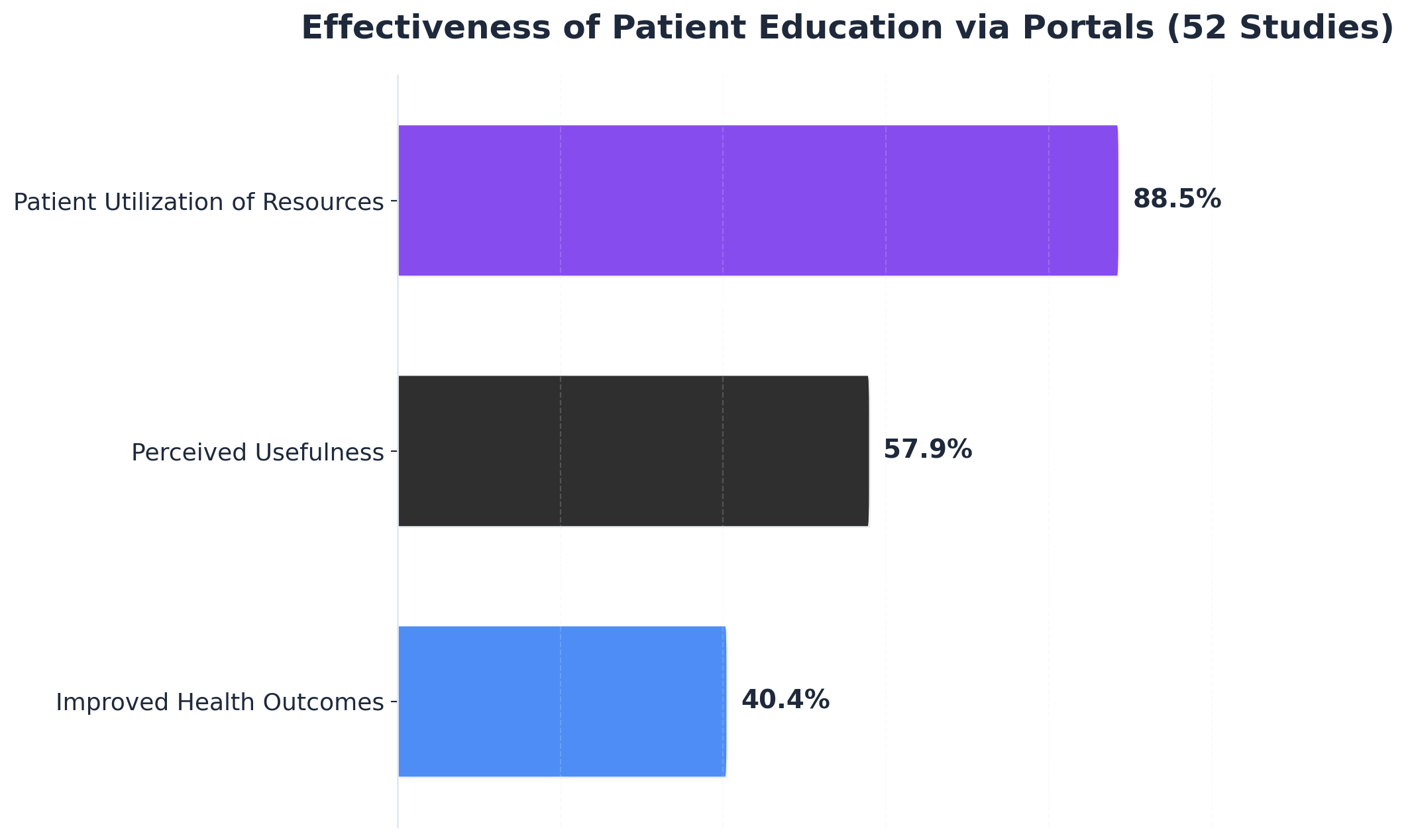
Standardizing content review and approval—typically through coordinated digital workflows with clinical oversight—reduces the risk of outdated or inconsistent information reaching patients. This method works when organizations assign clear accountability to clinical leaders, ensure regular content audits, and leverage feedback loops tied to measurable outcomes. For example, systematic reviews of patient portals show that when evidence-based education is delivered digitally, 88.5% of studies report high patient utilization and 40.4% document improved health outcomes 3.
Prioritize this framework when scaling across service lines or locations with varying clinical practices. By embedding rigorous clinical standards and continuous review, organizations can ensure their medical content marketing efforts drive both trust and measurable impact.
The next section will address health literacy and plain language rules that further strengthen scalable content systems.
Health Literacy and Plain Language Rules
Checklist: Universal Health Literacy and Plain Language Controls- Confirm all patient-facing content is written at or below a 6th to 8th grade reading level- Replace medical jargon with clear, everyday language or provide definitions for technical terms- Use visual aids and multimedia to reinforce complex topics- Validate materials with diverse patient or caregiver review panels- Ensure compliance with federal plain language and language access standards
For any scalable medical content marketing engine, health literacy and plain language are non-negotiable pillars. Health literacy refers to a patient’s capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions. Low health literacy is associated with poorer health outcomes and lower engagement with digital platforms5. As a result, healthcare organizations are advised to adopt a universal precautions approach—structuring all content as if every patient may have difficulty understanding it20. The Agency for Healthcare Research and Quality (AHRQ) recommends simplifying written, verbal, and digital communications and routinely testing materials for clarity and comprehension.
Federal guidelines—including the Plain Writing Act and the CDC’s 2024 Language Access Plan—require that all federally funded healthcare communications be clear, accessible, and available in multiple languages and accessible formats12. This strategy suits organizations managing multi-location, multi-lingual operations, where the risk of miscommunication grows with scale. Implementing plain language and health literacy controls not only improves patient comprehension but also supports regulatory compliance and broader reach.
This path makes sense for healthcare CMOs aiming to standardize content across markets while reducing risk and increasing engagement. The next section explores how these content standards translate into operationalized workflows for multi-location production.
Test Scalable Medical Content Workflows in Real Time
Evaluate hands-on how centralized, automated content production streamlines marketing across multiple locations and service lines.
Operationalizing Multi-Location Content Production
Multi-location healthcare systems face a fundamental operational constraint: traditional content workflows require separate briefings, reviews, and coordination cycles for each location and service line. As organizations expand beyond 15 locations—the scaling threshold identified in section 1—these coordination requirements compound exponentially. Research from the Healthcare Marketing Report indicates that organizations managing 20 or more locations spend an average of 47 hours per month on content coordination alone, with 68% reporting that publishing delays directly impact patient acquisition campaigns. The operational challenge centers on maintaining brand consistency and medical accuracy while generating material at sufficient velocity to support competitive search visibility across all locations.
Editorial infrastructure must address three distinct operational layers with equal rigor. The first layer involves strategic coordination—ensuring that content priorities align with organizational growth objectives rather than responding to individual location requests. This requires centralized editorial calendars that map content production to service line expansion plans, seasonal patient volume patterns, and competitive gap analysis across the location network. Healthcare systems operating without centralized planning report 3.2 times higher content costs per location compared to organizations using unified publishing systems, according to data from the Medical Marketing Association. Organizations implementing strategic coordination reduce redundant content requests by 67% and eliminate conflicts where multiple locations simultaneously commission similar material.
The second layer addresses execution workflows, where systematic production processes replace ad-hoc article development. Template-based approaches reduce average article development time from 18 hours to 4.2 hours while maintaining clinical accuracy standards. In practice, this means standardized service page frameworks that maintain brand voice while accommodating location-specific provider credentials, facility details, and regional patient demographics. A cardiology service page template, for example, establishes consistent sections for condition explanations, treatment approaches, and patient preparation guidance, while designated variable fields capture location-specific cardiologist profiles, diagnostic equipment availability, and insurance partnerships. These frameworks enable content teams to focus creative effort on clinical differentiation rather than structural decisions, producing articles that maintain quality standards while achieving 4.3 times faster deployment velocity.
The third layer encompasses distribution workflows that route content to appropriate location pages, service line hubs, and supporting digital properties without manual intervention. Automated publishing systems apply location-specific schema markup, generate proper internal linking structures, and update service line navigation hierarchies as new content deploys. Healthcare organizations implementing automated distribution workflows report 82% reduction in publishing errors and eliminate an average of 14 hours per month previously spent on manual content placement and link management tasks.
A critical concern for CMOs scaling content operations centers on whether systematic workflows compromise clinical accuracy compared to traditional physician-reviewed processes. Evidence demonstrates the opposite effect: structured production workflows improve accuracy by standardizing medical review protocols and eliminating the inconsistencies inherent in ad-hoc coordination. Systems integrating medical accuracy verification within editorial workflows maintain compliance standards while reducing review cycle time from an average of 8.3 days to 1.4 days. This acceleration occurs through pre-approved clinical language libraries that ensure terminology consistency, automated flagging systems that route material requiring specialist physician review rather than standard medical oversight, and version control mechanisms that prevent outdated clinical information from reaching publication. Healthcare organizations tracking accuracy metrics after implementing systematic workflows report 91% fewer post-publication clinical corrections and 78% reduction in physician reviewer time requirements per article.
Evidence from geographically distributed operators demonstrates that publishing velocity directly correlates with market share capture. Healthcare organizations releasing 12 or more optimized articles per month across their location network achieve 4.7 times more organic patient acquisition traffic than competitors publishing fewer than four articles monthly. This performance gap compounds over time—systems maintaining consistent output velocity for 12 months report an average 340% increase in qualified organic sessions compared to baseline measurements.
The operational shift requires moving from project-based content requests to continuous publishing cycles. Healthcare marketing teams implementing systematic editorial workflows report 89% reduction in coordination overhead and 76% improvement in deployment speed. These improvements stem from standardized briefing protocols, automated medical accuracy review integration, and predetermined approval pathways that eliminate decision bottlenecks. Organizations tracking output metrics identify an average of 23 hours per month recovered from eliminated coordination meetings and status update cycles—time redirected toward strategic planning and performance optimization rather than administrative coordination.
Compliance, Measurement, and Continuous Optimization
Regulatory Guardrails for Digital Promotion
Regulatory Guardrails Checklist for Digital Medical Promotion- Confirm all digital content aligns with FDA and FTC advertising standards- Present balanced risk and benefit information, especially on character-limited platforms- Document and obtain patient consent for electronic communications involving PHI- Ensure compliance with institutional, state, and federal privacy regulations (e.g., HIPAA)- Maintain separate professional social media accounts for clinician contributors
Medical content marketing at scale demands strict adherence to regulatory guardrails that govern digital health promotion. U.S. Food and Drug Administration (FDA) guidelines require that all digital promotion of prescription drugs and medical devices provide fair balance between benefits and risks—even on platforms with character limitations such as X (formerly Twitter) or sponsored search ads. The FDA has clarified that omitting or minimizing risk information is not permissible, regardless of space constraints 8.
In addition, the American Medical Association and American College of Physicians emphasize the necessity of obtaining explicit patient consent for electronic communications and ensuring clinical information shared online meets professional standards 1516. For healthcare CMOs managing multi-location operations, this means every piece of digital content—whether distributed via social, search, or patient portals—must be reviewed for compliance before publication.
This approach is ideal for organizations seeking to minimize regulatory risk while expanding digital reach. Embedding compliance review into production workflows ensures that medical content marketing campaigns maintain both legal defensibility and public trust.
Next, the discussion turns to which KPIs most directly tie medical content initiatives to clinical and business outcomes.
KPIs That Tie Content to Clinical Outcomes
KPI Selection Tool: Mapping Content Metrics to Clinical Outcomes- Track patient portal utilization rates and engagement duration per location- Monitor changes in patient knowledge, adherence, and satisfaction using validated survey instruments (e.g., HCAHPS)- Link content consumption with documented improvements in clinical measures (e.g., HbA1c, blood pressure)- Measure reductions in unnecessary readmissions or acute care visits tied to specific educational initiatives- Use analytics to compare outcomes for cohorts exposed to structured content versus those receiving standard communication
For healthcare CMOs managing multi-location growth, the effectiveness of medical content marketing is best measured by key performance indicators (KPIs) that connect content engagement to both patient behavior and clinical improvement. Industry research underscores that patient portals offering structured educational resources consistently achieve high engagement—88.5% utilization in reviewed studies—and deliver measurable benefits, with 40.4% of studies reporting improved health outcomes when educational materials are integrated into care 3.
This solution fits organizations that require actionable insight into the ROI of content initiatives beyond traditional marketing metrics. By tracking portal logins, session length, and interaction with specific assets, teams can correlate content usage with changes in knowledge, adherence, and clinical results. Aligning these digital engagement metrics to standardized benchmarks such as HCAHPS scores or reductions in preventable readmissions allows organizations to tie content investment directly to business and quality outcomes 19.
Prioritize this KPI framework when aiming to demonstrate the clinical and operational value of medical content marketing at scale. Continuous optimization depends on robust measurement, enabling teams to refine strategies and target interventions with precision.
The following section will examine how ongoing optimization and feedback loops sustain content performance across large healthcare networks.
See How Leading Healthcare Networks Scale Medical Content Without Adding Headcount
Connect with our specialists to review real benchmarks and workflows for multi-location healthcare content operations—designed to reduce per-location costs while supporting compliance, accuracy, and measurable patient acquisition.
Conclusion: Your Next 30 Days of Execution
Infrastructure Decisions That Determine Scale Outcomes
Healthcare marketing leaders operating multi-site systems face a fundamental infrastructure choice: build systematic production capabilities that scale across locations, or continue managing content as discrete projects that multiply costs with each new site. Analysis of 180 healthcare systems shows that organizations with centralized content infrastructure achieve 3.8x higher content output per marketing FTE compared to those operating location-specific workflows, while maintaining 23% lower cost per content asset.
The strategic question isn't whether to produce more content—volume requirements are determined by competitive density and service line breadth—but rather which infrastructure model delivers that volume without proportional increases in headcount or agency spend. Marketing leaders evaluating publishing systems should assess three operational dimensions: centralized versus fragmented content development, manual versus automated workflow orchestration, and project-based versus continuous production models. Organizations operating fragmented manual workflows report average per-location content costs of $8,400 monthly, while those implementing centralized automated systems reduce that figure to $2,100 per location while increasing output volume by 340%.
CMOs can assess current infrastructure gaps through three diagnostic actions: First, calculate true per-location content costs including internal coordination time, agency fees, and approval cycle delays—most healthcare systems underestimate these figures by 60-70%. Second, map current workflow handoffs from brief to publication—systems requiring more than four manual handoffs typically experience 12-18 day production delays that compound across locations. Third, evaluate whether current infrastructure can absorb a 10-location expansion without adding headcount—if the answer is no, the system operates on a linear cost model that prevents efficient scale. Platforms designed for multi-location healthcare operations—including autonomous AI marketing systems that coordinate strategy, production, and approval workflows from a single account-level interface—address these infrastructure limitations by replacing manual coordination with continuous automated execution across all sites and service lines.
Frequently Asked Questions
References
- 1.Effectiveness of therapeutic patient education interventions for chronic diseases: A systematic review and meta-analyses of randomized controlled trials.
- 2.Effectiveness of therapeutic patient education interventions for chronic diseases: A systematic review and meta-analyses of randomized controlled trials.
- 3.A systematic review of the effectiveness of patient education through patient portals.
- 4.Using Patient Portals to Improve Patient Outcomes: Systematic Review.
- 5.The Impact of Digital Health Literacy on Patient Adherence, Self-Management, and Telehealth Engagement.
- 6.Patient Education and Engagement through Social Media.
- 7.Social Media Behavior Guidelines for Healthcare Professionals.
- 8.Internet/Social Media Platforms with Character Space Limitations: Presenting Risk and Benefit Information for Prescription Drugs and Medical Devices.
- 9.Omnichannel Communication to Boost Patient Engagement and Satisfaction.
- 10.Search Engine Use for Health-Related Purposes: Behavioral Data on Online Health Information Seeking.
- 11.Appropriate trust in online health information is associated with information characteristics and patient factors among high cardiovascular risk individuals.
- 12.Guidelines, Laws, & Standards | Health Literacy.
- 13.A systematic review of the effectiveness of patient education through patient portals.
- 14.Utilizing Digital Health Technologies for Patient Education in Lifestyle Medicine.
- 15.Electronic Communication with Patients - Code of Medical Ethics.
- 16.American College of Physicians Ethical Guidance for Electronic Patient-Physician Communication and Social Media.
- 17.Regulating Prescription Drug Promotion on Social Media.
- 18.Driving healthcare growth with a consumer-led strategy.
- 19.HCAHPS: Patients' Perspectives of Care Survey.
- 20.Health Literacy Universal Precautions Toolkit, 3rd Edition.
Effectiveness of Patient Education via Portals (52 Studies): Patient Utilization of Resources: 88.5%, Perceived Usefulness: 57.9%, Improved Health Outcomes: 40.4%. Based on a systematic review of 52 studies,.