
Key Takeaways
- Channel-level execution breaks at scale because separate SEO, PPC, content, and reputation vendors produce inconsistent provider data and conflicting messaging that erode the trust signals patients use to choose care 1.
- A five-layer operating system—discovery, demand capture, authority, reputation, and engagement—runs against one patient journey under a shared compliance envelope and a single cost-per-acquired-patient target 2.
- Compliance works as a design constraint, not a final checkpoint: HIPAA, AMA ethics, FDA misinformation posture, and HHS telehealth guidance shape targeting, content, and intake decisions before launch 5, 4, 6.
- Multi-location operators should start with discovery infrastructure, since a single source of truth for provider, location, and service-line data is what lets paid spend, authority content, and reviews compound 9.
Why Channel-Level Tactics Stopped Working for Multi-Location Healthcare
Most medical marketing playbooks still read like a checklist: rank the service pages, run the branded search campaign, post to social, harvest a few reviews. That sequencing worked when a practice operated from one address and competed against a handful of local peers. It breaks down the moment a healthcare operator is running fifteen, fifty, or two hundred locations across multiple states and service lines.
The patient journey has consolidated into something closer to a single connected path. Patients now move between search results, narrative reviews, social content, telehealth intake forms, and patient portals before and after they book, and they cross-check what they see against authoritative sources 7. Mayo Clinic Proceedings Digital Health frames this as an omnichannel reality where engagement, access, and cost outcomes depend on coordinating marketing, communication, and care delivery across organizational silos 2.
Channel-level execution cannot coordinate that path. Separate SEO, PPC, content, and reputation vendors—often duplicated per location—produce inconsistent provider data, conflicting messaging, and review responses that contradict the brand voice three locations away. Internet-based promotion is now indispensable to acquisition 1, yet fragmented delivery actively undermines the trust signals patients use to choose a provider.
The operators pulling ahead treat medical internet marketing as one account-level operating system. Five interlocking layers—discovery, demand capture, authority, reputation, and engagement—run against the same patient journey, governed by the same compliance envelope, measured against the same cost-per-acquired-patient targets. The rest of this framework lays out how those layers connect.
The Five-Layer Operating Framework
Discovery: Local and Service-Line SEO as Account-Wide Infrastructure
Discovery is the layer where most multi-location operators bleed efficiency first. Each location ships its own Google Business Profile, its own NAP variations, its own provider pages copy-pasted from a template that nobody owns. Search engines pick up the inconsistency. Patients pick up the inconsistency. Service-line authority dilutes across dozens of orphaned URLs that compete with each other instead of with regional rivals.
Evidence-based healthcare SEO has moved past keyword density and link counts. The peer-reviewed overview of healthcare SEO argues that optimization must prioritize accuracy, transparency, and alignment with medical guidelines, because higher-ranked pages disproportionately shape public understanding of health topics 9. That requirement collides directly with how most multi-location stacks are built: marketing owns the page, a contracted writer owns the copy, the clinical team never reviews it, and the per-location agency optimizes for ranking signals without regard to medical accuracy.
An account-level discovery layer treats local and service-line SEO as one infrastructure problem, not two. Provider data, location data, and service-line content live in a single source of truth that propagates to every site, GBP listing, and schema markup block. Service-line pages are templated at the account level with clinical review built into the publication path, then localized with the specific provider roster, insurance acceptance, and facility detail for each location. Internal linking maps service lines to location pages and back, so authority compounds across the footprint rather than fragmenting.
This approach also makes optimization auditable. When a service-line page updates to reflect a new clinical guideline, the change ships to every location simultaneously, with the same citation trail. That is the version of SEO that meets the accuracy and transparency bar healthcare ranking now requires 9—and it only works when discovery is run as account-wide infrastructure, not as a per-location task.
Demand Capture: Paid Acquisition and DTC Telehealth Funnels
Paid acquisition in healthcare carries operating constraints that consumer marketers never see. Targeting parameters that look routine on a retail account—health condition interests, lookalike audiences seeded from patient lists, retargeting pixels firing on symptom pages—run into HIPAA boundaries and the privacy expectations patients bring to digital health services. Research on privacy and digital health trust shows that perceived commercialization of personal health data measurably reduces willingness to engage 11. Sloppy ad targeting does not just risk a violation; it depresses the conversion rate of the campaign that triggered it.
Direct-to-consumer telehealth funnels add a second constraint layer. The HHS DTC telehealth guidance is explicit that providers must address privacy, licensure, prescribing rules, and technology standards across every jurisdiction served, and that digital entry points should clearly explain services and their limits 5. For an operator running telehealth across state lines, that means campaign geography is bounded by where providers are licensed, ad creative must match what is actually offered in that state, and the intake flow must route the patient to a provider who can lawfully see them.
Telehealth is worth the operational investment because it works as an access channel. Patient satisfaction studies from the pandemic-era surge documented generally high satisfaction with virtual visits, particularly when platforms were easy to use and integrated with existing care relationships 12. That makes telehealth a durable conversion endpoint for paid campaigns, not a temporary substitute.
The operating discipline at this layer is matching bid strategy and creative to capacity. Paid campaigns that drive demand into service lines or geographies without provider availability inflate cost-per-acquired-patient and erode trust at intake. Demand capture only pays back when the system behind the click can actually see the patient.
Authority: Content, E-E-A-T, and the Credibility Cross-Check
Patients do not read healthcare content the way they read a retail blog. They cross-check it. Research on patient use of social and online health information finds that patients routinely compare what they see on social platforms against more authoritative sources, and that perceived expertise and transparency drive trust while sensational or misleading content erodes it 7. Content that cannot survive that cross-check does not convert—it actively damages the brand running it.
Authority content for a multi-location operator is built around three signals search engines and patients both reward: clinical authorship, evidence citation, and structural transparency about who reviewed the content and when. Provider bios connect to the articles those providers wrote or reviewed. Service-line content carries the clinical guideline references it draws from. Update dates reflect actual review, not a CMS timestamp from a cosmetic edit.
The same approach addresses the AI-generated content problem most marketing teams are now wrestling with. The bar is not whether a piece was drafted by a human or a model. The bar is whether the published version reflects accurate medical information that a qualified clinician has endorsed and that a patient can verify against the sources cited. The evidence-based SEO literature reinforces this: accuracy and alignment with medical guidelines are ranking-adjacent requirements, not aesthetic ones 9.
Authority content also feeds the other framework layers. Reputation responses cite back to it. Paid landing pages link to it for substantiation. Telehealth intake flows surface it as pre-visit education. Treating content as a standalone SEO asset misses the compounding role it plays once it is built to clinical standard. The operators getting return on content investment are the ones treating every article as a multi-channel asset under one editorial governance model.
Reputation: Narrative Reviews as an Acquisition Lever
Reputation has been undersold to healthcare marketing leaders as a soft signal. The evidence says otherwise.
A 2023 study of patient e-doctor choice on digital platforms found that narrative reviews significantly increase the likelihood of selection by enhancing perceived functional and emotional value, and that the richness and credibility of qualitative reviews mattered more for decisions than numerical scores alone 3. Separately, empirical work on physician choice in competitive markets shows that higher ratings and more favorable comments correlate with increased patient volumes—and that negative reviews disproportionately influence perception when overall review counts are low 8. Read together, those findings reframe reputation as a measurable acquisition lever with two operating variables: narrative quality and review velocity per location.
For a multi-location operator, the velocity variable is where most programs underperform. A location with eighteen lifetime reviews is one bad weekend from a star-rating drop that the empirical evidence says will measurably depress patient volume 8. A location with four hundred reviews absorbs the same incident without a market signal. Closing that gap requires a review-request workflow built into post-visit communication at every location, not a quarterly campaign run by corporate marketing.
Narrative quality is the second variable, and it is harder to systematize. The qualitative content patients write—what the provider explained, how the front desk handled a billing question, whether the telehealth visit actually felt like care—is what shifts the next patient's choice 3. Operators get more useful narrative when the review request happens close to the experience and asks specific prompts rather than a generic five-star ask.
Response strategy completes the layer. Public responses to negative reviews are read by prospective patients more than the original review in many cases. The FDA's draft guidance on correcting third-party misinformation about prescription drugs and devices is a useful reference point for the posture: corrections should be truthful, non-misleading, and limited to the issue at hand 6. The same discipline applies to review responses generally—correct factual errors without disclosing protected information, and never let a single response create a HIPAA exposure.
Engagement: Portals, Messaging, and the Post-Click Experience That Protects CAC
Every dollar spent in the first four layers is wagered against the engagement layer. A patient who clicks through a paid ad, books an appointment, and then hits a portal they cannot log into, a messaging thread that goes unanswered for four days, or a telehealth platform that fails to load is a patient whose acquisition cost was paid but whose lifetime value was not earned.
The patient engagement research is direct about what drives perceived value in digital tools: ease of use, responsiveness, and clear integration with the care team 10. Fragmented or hard-to-use tools actively reduce engagement and trust, which means the post-click experience is not a separate operations problem—it is an acquisition problem that shows up downstream in retention, referrals, and review sentiment.
For multi-location operators, the engagement layer is where channel coordination either pays back or collapses. A patient acquired through a knee-pain campaign in one market should land in the same portal experience, with the same messaging response SLA and the same telehealth follow-up option, as a patient acquired in any other market. When the portal is inconsistent across locations—different login flows, different appointment types exposed, different response cadences—the acquisition campaign's measured CAC understates the real cost, because the patient who churns at the portal has to be replaced.
The omnichannel framing from the Mayo Clinic Proceedings Digital Health synthesis applies precisely here: improving engagement and access depends on integrating data and processes across organizational silos 2. Marketing cannot fix the portal alone. But marketing leaders accountable for CAC have to make the post-click experience a measured variable, because it determines whether the spend at the top of the funnel ever returns.
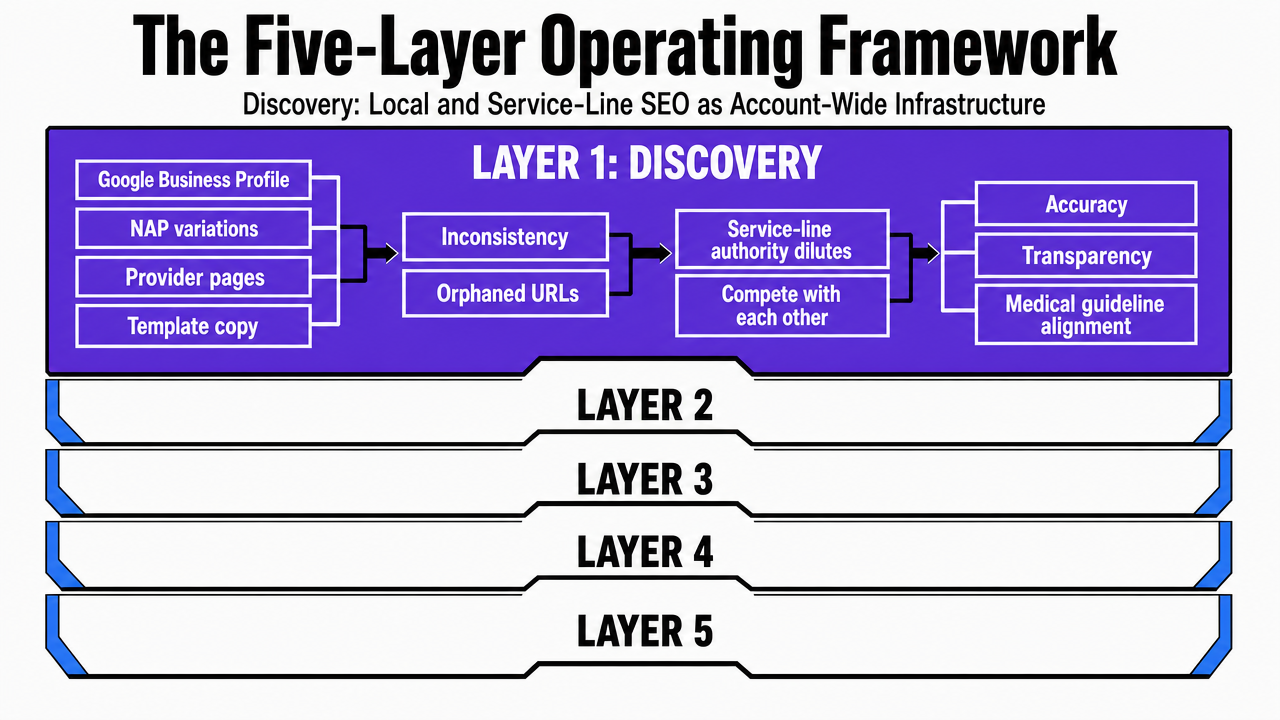 Visualize the five interlocking layers of the operating framework as a stacked process diagram tied directly to the section structure
Visualize the five interlocking layers of the operating framework as a stacked process diagram tied directly to the section structure
Test unified multi-location campaigns before committing
Run real-time, location-wide medical marketing initiatives risk-free for one week and measure results directly.
Compliance as Design Constraint, Not Afterthought
Compliance fails healthcare marketing programs when it shows up as a legal review checkpoint at the end of a campaign. By that stage, the targeting decisions, the social copy, the review response template, and the telehealth landing page have already been built around assumptions that may not survive scrutiny. The cost of unwinding that work is what produces the familiar pattern of slow launches and risk-averse creative that underperforms.
The framework treats four regulatory inputs as design constraints baked into each layer. HIPAA boundaries shape what data can seed ad audiences and retargeting pixels, which is why privacy-by-design ad targeting is a discovery and demand-capture decision, not a post-launch audit. Patients withdraw from digital health services when they perceive personal data is being commercialized 11, so the constraint is also a conversion variable.
The AMA's social media ethics opinion governs the authority and reputation layers. It draws clear lines around confidentiality, separation of personal and professional content, and avoidance of misleading information, warning that misuse can undermine the patient-physician relationship and the profession's integrity 4. Provider-authored content, social posts featuring clinicians, and review responses involving named providers all sit inside that envelope.
The FDA's draft guidance on correcting third-party misinformation defines the posture for engaging with user-generated content about products and services. Corrections should be truthful, non-misleading, and limited to the misinformation at issue, and firms are generally not responsible for independent third-party content they do not control 6. That posture transfers cleanly to review responses and social comment moderation.
The HHS direct-to-consumer telehealth guidance governs demand capture and engagement for virtual care, requiring alignment with privacy, licensure, prescribing, and technology standards across every jurisdiction served 5. Run as a design constraint, compliance narrows the creative space early and removes the late-stage rework that quietly inflates campaign cost.
Coordinating the Layers Against a Single Patient Journey
The five layers only produce account-level economics when they share a patient journey, not just a dashboard. A prospective knee-replacement patient does not experience SEO, then PPC, then content, then reviews, then portal access as discrete events. They move through a sequence—organic search to service-line page to narrative reviews to insurance verification to telehealth consult to in-person visit—and every layer either reinforces the next handoff or breaks it.
Coordination starts with a shared definition of the journey by service line. Orthopedic intake looks different from dermatology intake, which looks different from behavioral health intake. The discovery layer surfaces the right service-line page, the demand-capture layer routes paid traffic to a landing experience matched to that intake, the authority layer supplies the clinical substantiation a researching patient looks for, the reputation layer carries the narrative reviews specific to that service and location, and the engagement layer delivers a portal and messaging experience configured for that care pathway. The omnichannel synthesis in Mayo Clinic Proceedings Digital Health is clear that this kind of cross-silo integration is what separates engagement gains from fragmented spend 2.
Three coordination signals show whether the layers are actually connected:
- Provider data matches across GBP, service-line pages, authority content bylines, and intake confirmations.
- Response cadence—paid lead follow-up, review response, portal message reply—is measured against a single SLA at the account level.
- Compliance review runs once per asset and propagates, instead of repeating per location.
Centralize Medical Internet Marketing With a Unified Multi-Location Strategy
See how leading healthcare groups eliminate workflow silos and manage content, SEO, and PPC at scale—all from a single, data-driven operating system built for complex, multi-site operations.
If You Manage Multiple Locations: Consolidation Economics
For operators running more than a handful of sites, the framework's economics turn on a single question: is each layer executed once at the account level, or repeated per location through a stack of vendors?
The traditional model multiplies cost and coordination drag with every new site. A per-location SEO retainer becomes a per-location retainer times N. A separate PPC vendor runs campaigns that do not know what the content team published last week. Backlink work happens in isolation from the service-line pages it should be supporting. Compliance review repeats for every market because no asset is treated as account-level canon. The omnichannel integration that drives engagement and access outcomes 2is precisely what this structure prevents.
The account-level operating-system model inverts those line items. The table below contrasts the two on the dimensions that show up in a healthcare marketing P&L.
| Dimension | Per-Location Agency Stack | Account-Level Operating System |
|---|---|---|
| Scope of coverage | Per-location retainer × N locations, often duplicated per channel (SEO, PPC, content, backlinks) | Single account-wide program covering all sites and service lines |
| Coordination overhead | Multiple account managers, manual handoffs, cross-vendor status meetings | One strategy approval path; execution coordinated against a shared journey |
| Execution cadence | Retainer-bound deliverables, monthly reporting cycles, queue-based response | Continuous execution against prioritized actions |
| Compliance review path | Repeated per location and per vendor; late-stage rework common | Reviewed once per asset at the account level, then propagated |
| Reporting unification | Channel- and location-siloed dashboards; manual roll-up | Account-wide reporting across channels and sites |
| Anchored cost reference | Variable per location, per channel | Vectoron post-trial: $599/mo |
The point of the comparison is not the dollar figure on any single line. It is what the cost structure incentivizes. Per-location retainers reward vendors for protecting scope, not for coordinating across the patient journey. An account-level program is paid to make the layers reinforce each other, which is the only structure that produces the omnichannel coordination the evidence base rewards 2.
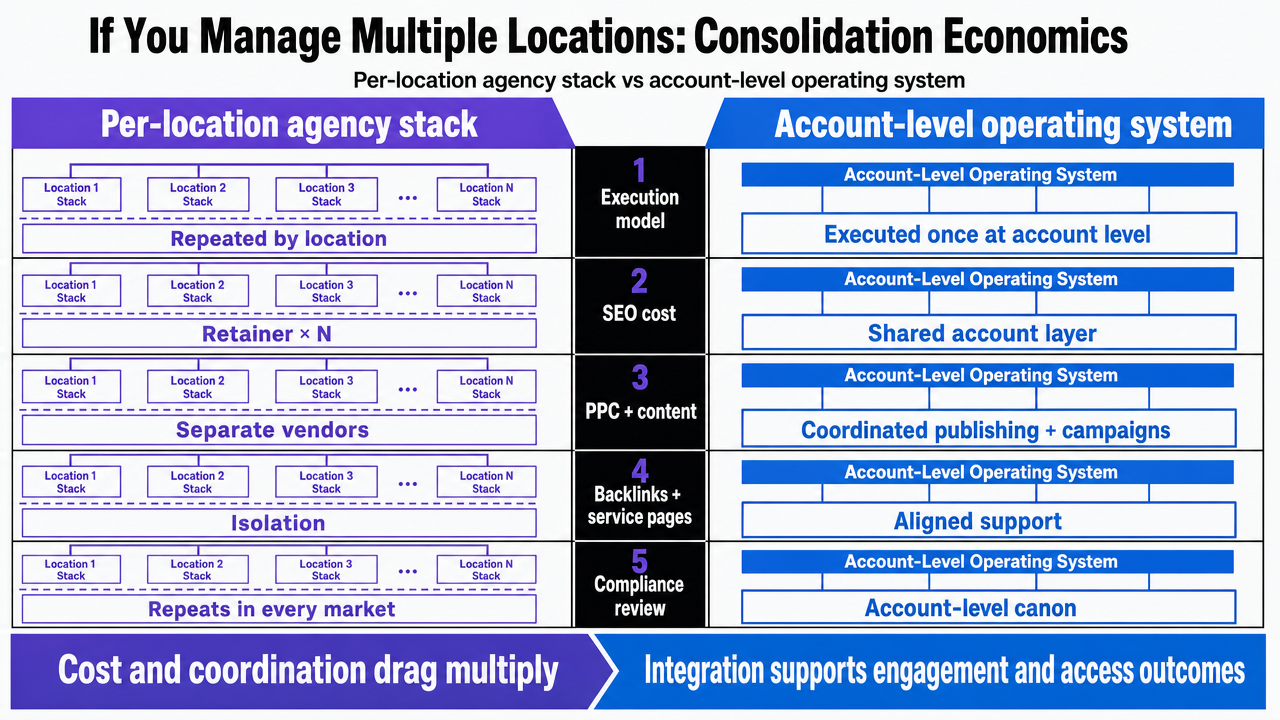 Side-by-side comparison infographic mirroring the article's comparison table between per-location agency stack and account-level operating system
Side-by-side comparison infographic mirroring the article's comparison table between per-location agency stack and account-level operating system
What a Working Account-Level System Looks Like
A working account-level system shows up in three observable artifacts, not in a strategy deck.
- The first is a single source of truth for provider, location, and service-line data that propagates to every GBP listing, schema block, intake form, and authority byline without manual reconciliation.
- The second is a coordination layer where the next prioritized action across discovery, demand capture, authority, reputation, and engagement is visible against the same patient journey and the same compliance envelope—so a service-line content update, a paid creative refresh, and a review response template are sequenced rather than queued by separate vendors.
- The third is a unified reporting view that ties cost-per-acquired-patient back to the post-click experience the patient actually received 2.
Healthcare marketing leaders evaluating this shift can start the Vectoron trial to see the layers running against an account, then operate the program at $599/mo. The framework is the deliverable; the platform is how it runs continuously without per-location vendors stitching it together after the fact.
Frequently Asked Questions
References
- 1.The adaptation of health care marketing to the digital era.
- 2.An Overview of Omnichannel Interaction in Health Care Services.
- 3.The Impact of Narrative Reviews on Patient E-doctor Choice from the Perspective of Patient-perceived Value.
- 4.2.3.2 Professionalism in the Use of Social Media.
- 5.Developing a direct-to-consumer telehealth strategy.
- 6.Draft Guidance for Industry: Internet/Social Media Platforms – Correcting Independent Third-Party Misinformation About Prescription Drugs and Medical Devices.
- 7.Social media and online health information: the patient perspective.
- 8.Online reviews and their impact on patient choice of physicians.
- 9.Search engine optimization for healthcare websites: an evidence-based overview.
- 10.Digital health and patient engagement: what matters to patients?.
- 11.Privacy concerns and trust in digital health services.
- 12.Telehealth and patient satisfaction during the COVID-19 pandemic.