Key Takeaways
- Patient acquisition has become a coordination problem, not a per-location creative problem, because system competitors run one keyword plan, one bid logic, and one compliance pipeline across every site 10.
- Per-site retainers quietly fail through duplicated keyword maps, sister locations bidding against each other in shared geos, and inconsistent FTC substantiation review at the publish stage 5.
- An account-level model runs one plan feeding content, technical SEO, paid media, and backlinks from shared inputs, with substantiation decided in the brief rather than debated per asset.
- Report blended patient acquisition cost, service-line lifetime value, and LTV-to-CAC by location instead of channel CPL, since patient relationships compound over multiple periods 9.
Why Patient Acquisition Stopped Being a Per-Location Problem
A 40-site dermatology group running paid search through three different agencies will, on any given Tuesday, have two of those agencies bidding against each other on the same Phoenix ZIP code. The third will have paused its campaigns for compliance review on a before-and-after photo that the other two are still serving. None of them share a keyword map. None of them know what the central content team published last week. The CFO sees a single line item called "marketing" and asks why patient acquisition cost is climbing.
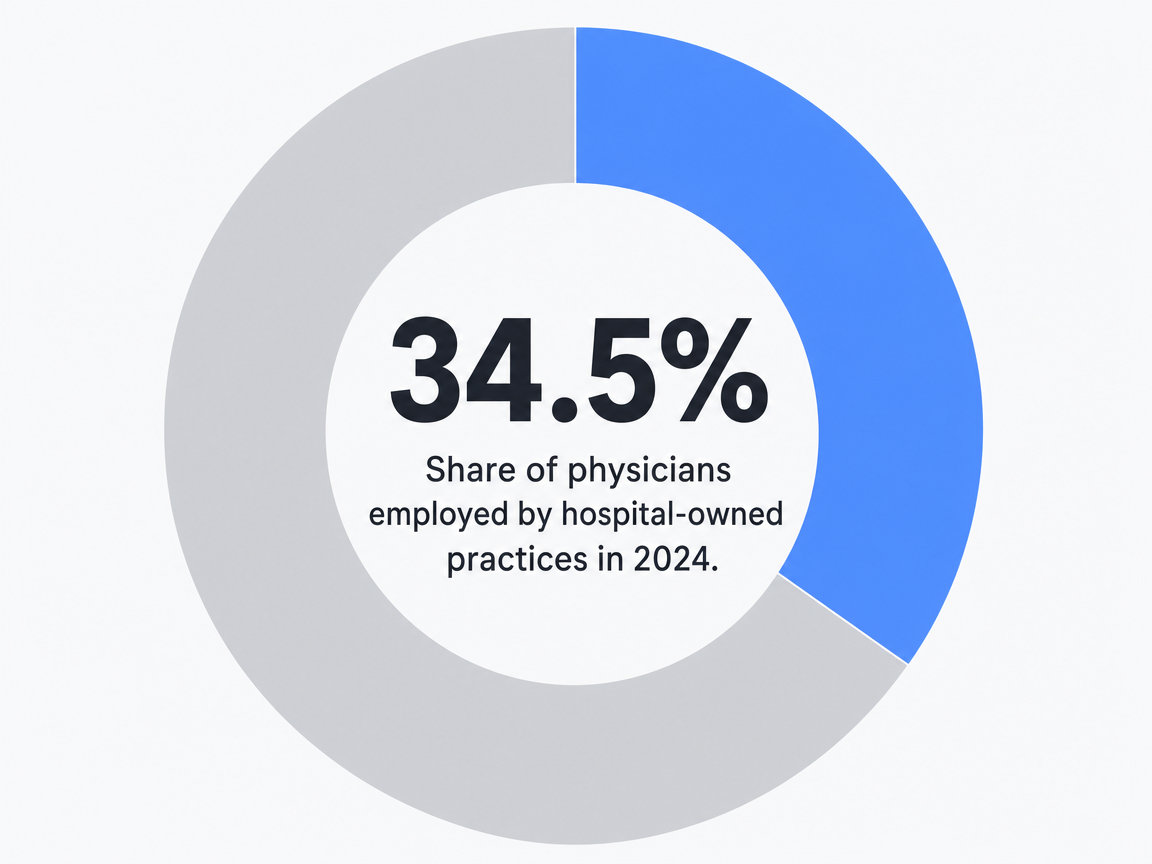 Share of physicians employed by hospital-owned practices in 2024: 34.5%
Share of physicians employed by hospital-owned practices in 2024: 34.5%
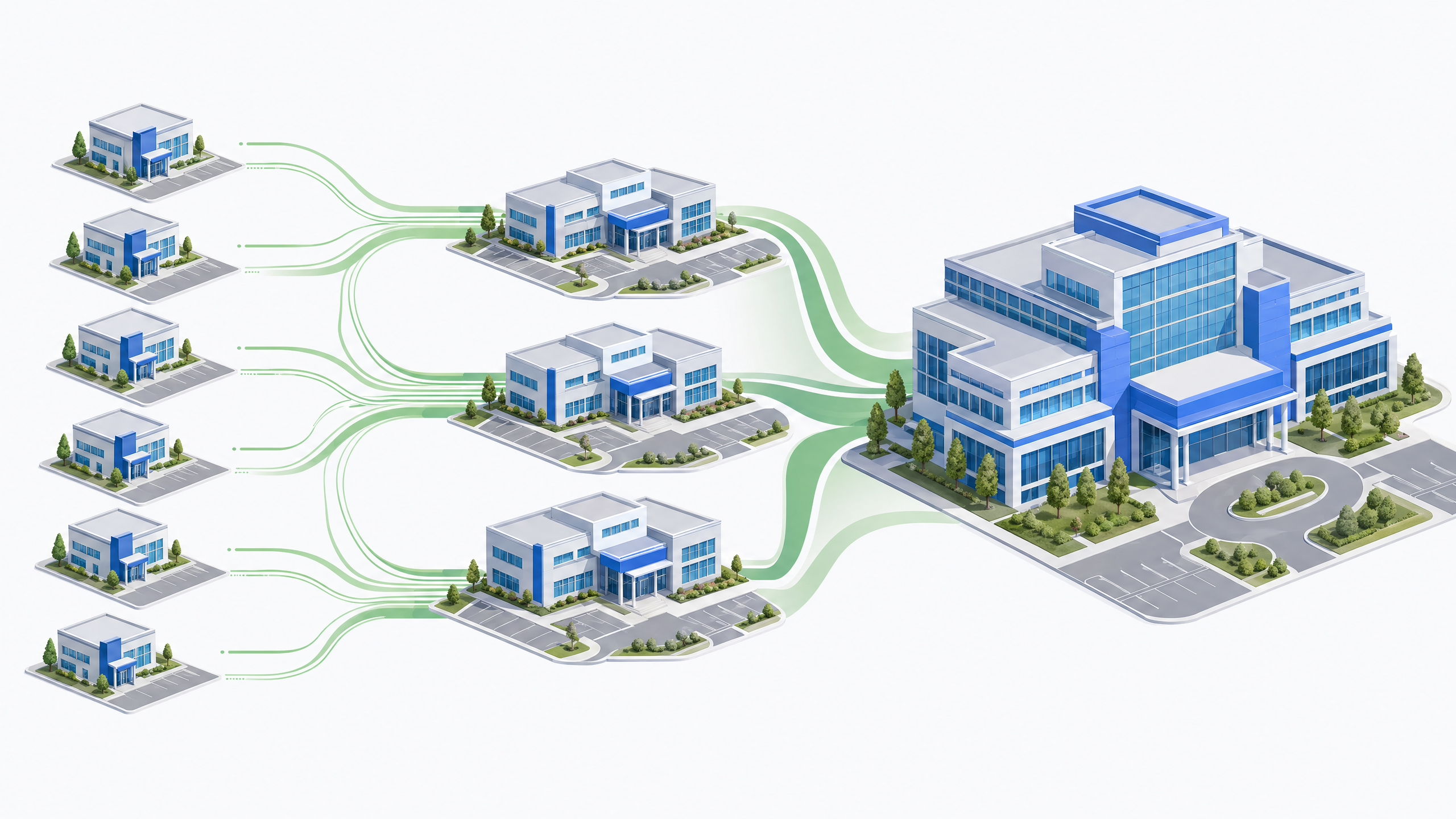
That scenario is now the default, not the exception. Hospital systems and large groups have absorbed enough of the physician workforce that independent and mid-market operators are no longer competing site-by-site against the urgent care across the street. They are competing against centralized marketing functions with one keyword strategy, one bid logic, and one compliance review pipeline running across dozens of locations 10.
The structural change matters because it inverts what scaling means. Per-location creative work, the model most groups inherited from a decade of agency retainers, generates duplicated research, conflicting bid strategies, and inconsistent claim substantiation under FTC rules 5. The work that wins patients now, educational content tied to search demand, paid media coordinated at the account level, and backlink acquisition pointed at the right service-line pages, has to be planned once and executed across the whole footprint 11.
This article treats medical marketing for doctors and practices as an operating-model question for VPs of Marketing managing five sites or 150. The tactics are settled. The coordination is not.
The Consolidation Pressure Reshaping Operator Economics
What Hospital-Owned Growth Means for Mid-Market Groups
The share of physicians working in hospital-owned practices climbed from 23.4% in 2012 to 34.5% in 2024, with 15.1% of practices acquired after 2019 alone 6. That is a twelve-point shift in who owns the supply side of care, concentrated heavily in the last five years. The acquisition wave is partly a response to fiscal stress on independent practices, including reimbursement pressure and rising operating costs that make a sale to a system the cleaner option 8.
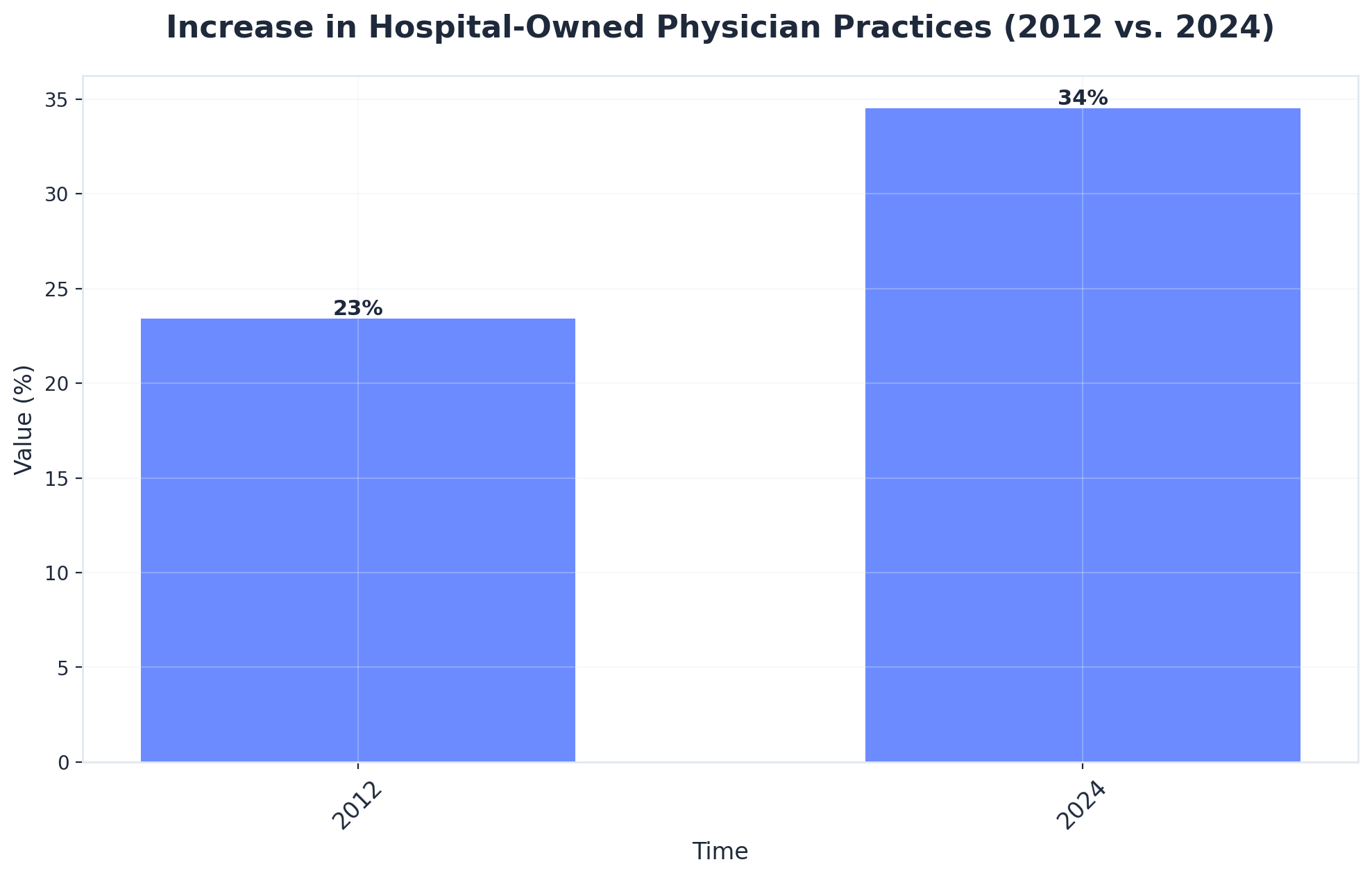 Increase in Hospital-Owned Physician Practices (2012 vs. 2024)
Increase in Hospital-Owned Physician Practices (2012 vs. 2024)
Increase in Hospital-Owned Physician Practices (2012 vs. 2024): 2012: 23.4%, 2024: 34.5%. Percentage of physicians working in practices owned by hospitals or health systems in 2012 versus 2024, highlighting the trend of practice consolidation.
For a VP of Marketing at a 25-site multispecialty group or a 60-clinic dental support organization, the consolidation number changes what the competitive map looks like at the ZIP-code level. Two things happen at once. First, more of the local search results, paid placements, and physician directory listings are occupied by hospital-system brands operating with central budgets. Second, the pool of independent practices available to acquire, partner with, or recruit from shrinks, which raises the pressure on organic patient acquisition through search and content rather than referral relationships built over years.
Competitive Asymmetry Against Centralized Health System Marketing
More than half of U.S. physicians are now employed by larger healthcare entities rather than maintaining independent practices 10. That workforce share is the practical ceiling on what mid-market and independent groups are competing against in any local market: not a peer practice, but a system-owned brand with shared capital, shared analytics, and a single marketing plan covering every service line.
The asymmetry shows up in concrete places. A health system marketing team running cardiology content does it once, optimizes it for the system's domain authority, and points internal links at every cardiology service location. An independent five-site cardiology group running the same playbook through three retainer agencies produces three keyword maps, three sets of landing pages, and three competitor analyses, none of which compound on each other. The system also has a centralized compliance review function that clears claims under FTC substantiation rules in one pass, while the independent group routes the same review through three different account managers with different interpretations 5.
The asymmetry is not a quality gap. It is a coordination gap. The AMA's digital strategy guidance for private practices explicitly recommends selecting firms with healthcare expertise and treating search, display, and paid social as a coordinated mix rather than separate channel buys 1. That recommendation reads differently in 2024 than it did a decade ago, because the alternative competitor is no longer the practice down the street. The operating-model question for VPs of Marketing is whether their current vendor stack can produce the kind of single-plan execution that system competitors already run as a default.
Coordination Drag: Where Per-Site Retainers Quietly Fail
Duplicated Keyword Maps and Conflicting Bid Strategies
The failure mode of a per-site retainer model is rarely dramatic. It is duplicative. A 12-site orthopedic group with three regional agencies will often have each agency build its own keyword map for "knee replacement," "rotator cuff repair," and the dozen long-tail variants that actually convert. Three teams pay for three SEMrush seats, run three competitor analyses on the same hospital-system competitor, and produce three sets of landing-page briefs that diverge on H1 structure, schema markup, and call-to-action language.
The paid side is worse because the conflicts are auction-visible. When two agencies manage Google Ads accounts for sister locations 14 miles apart, both bidding on "sports medicine near me" with overlapping geo-radii, the group is bidding against itself. CPCs rise. Quality Scores stay flat because no single account holds enough conversion volume to train the bidding algorithm at the keyword level. A single Google Ads MCC with shared negative-keyword lists, geo-fenced campaign structures, and consolidated conversion data fixes that, but only if one team owns the account architecture across every location.
The AMA's digital strategy guidance frames search, display, and paid social as a coordinated mix and recommends working with firms that understand healthcare-specific buying patterns 1. That recommendation assumes one firm running the mix, not three running parallel versions of it. For a VP of Marketing, the audit question is concrete: how many keyword research deliverables, how many competitor reports, and how many bid-strategy documents exist across the current vendor stack? The number is almost always larger than one, and almost never compounds into anything.
Compliance Review as a Production-Line Input
FTC Health Products Compliance Guidance requires that claims about treatment outcomes, safety, and product benefits be truthful, non-misleading, and supported by competent and reliable evidence at the time the claim is made 5. For medical practices, that standard applies to every before-and-after photo, every "95% patient satisfaction" badge, every "minimally invasive" descriptor, and every paid ad headline that promises a clinical result. The standard does not change based on which agency produced the asset.
The coordination problem is that per-location retainers route compliance review through whoever the account manager happens to be that month. One agency's reviewer flags a testimonial without a typicality disclaimer. Another approves the same testimonial because their interpretation of the substantiation requirement is looser. A third pauses the campaign for two weeks while waiting for the practice's outside counsel to weigh in. The asset itself is identical. The review outcome is not.
Treating compliance as a production-line input means the substantiation check happens once, inside the content workflow, before an asset reaches any channel. A claim like "reduces recovery time by 40%" either has a citable clinical study attached at the brief stage or it gets rewritten before a copywriter touches it. A photo asset either has a signed release with typicality language or it does not enter the asset library. The review is a gate in the production pipeline, not a debate at the publish stage.
That model also closes the gap between content and paid media. The same substantiated claim that clears for a service-line page clears for the Google Ads headline and the Meta carousel without three separate review cycles. For groups operating across state lines, where state medical board advertising rules layer on top of FTC requirements, centralized review is the only way to keep state-specific disclaimers consistent without slowing time-to-publish to a crawl. The operating question is whether compliance lives in the brief or lives in the inbox. The first scales. The second is the reason a 40-site group ships eight pieces of content a quarter when it should be shipping eighty.
Test Unified Medical Marketing Execution Now
Experience coordinated multi-location campaigns with measurable results before making any commitment.
An Account-Level Operating Model for Content, PPC, and Backlinks
One Plan Feeding Four Workstreams
The alternative to per-site retainers is not a bigger retainer. It is a single growth plan that produces the inputs every channel needs and a single execution layer that consumes them. Four workstreams hang off that plan: content, technical SEO, paid media, and backlink acquisition. Each one draws from the same keyword map, the same competitor analysis, the same compliance-cleared claim library, and the same conversion data.
The shared inputs matter because they are where coordination either compounds or breaks. A keyword map built once for a 30-clinic dermatology group identifies the priority service lines (Mohs surgery, pediatric eczema, cosmetic injectables), the geographic modifiers that actually have search volume, and the competitor pages currently ranking. That single artifact then drives the content brief for the Mohs service-line page, the negative-keyword list for the cosmetic Google Ads campaign, the anchor-text strategy for backlink outreach to dermatology associations, and the schema markup priority for technical SEO. Built three times across three agencies, those four downstream decisions diverge. Built once at the account level, they reinforce each other.
Paid media sits inside the same plan rather than running as a parallel function. A unified Google Ads MCC structure, with conversion tracking standardized across every location's appointment scheduler, lets the bidding algorithms see enough volume to optimize at the keyword and audience level instead of starving in 12 separate single-location accounts. The AMA's digital strategy guidance treats search, display, and paid social as a coordinated mix for exactly this reason 1. Coordination is the prerequisite for the algorithms to do their job.
Backlink acquisition is the workstream most often left out of the plan and the one where account-level execution produces the steepest gains. A single outreach program targeting state medical society publications, condition-specific patient advocacy organizations, and local health journalism builds authority for the root domain that every service-line page inherits. Run as twelve separate per-location campaigns, the same effort produces twelve thin link profiles that compete with each other for the same prospect lists.
Content as the Acquisition Spine, Not a Blog Calendar
Content is the workstream that holds the operating model together because every other channel depends on its outputs. McKinsey research on online health information found that practices using educational health media to engage consumers achieve measurably better patient acquisition, stronger brand perception, and more durable competitive differentiation than those that do not 11. The mechanism is straightforward: a substantiated service-line page ranks organically, supplies the landing destination for paid traffic, earns links from condition-specific publishers, and feeds the structured data that powers physician directory placements.
The mistake most groups make is treating content as a blog calendar measured in posts per month. A blog calendar produces volume without ranking intent. An acquisition spine produces a finite, prioritized library of pages mapped to specific search demand and specific service-line revenue. For a 50-site women's health group, that library might be 240 pages: a core service-line page per condition, location-modified variants for the top 30 metros, Spanish-language variants where census data justifies them, and a long-tail layer covering pre-visit questions that drive scheduling intent.
Each page enters production with its substantiation requirements specified in the brief, its target keyword cluster locked, and its internal link destinations mapped before a writer opens a document. Digital content reaches its measurable engagement and return ceiling only when it is produced this way, with the structure decided once and the execution centralized 7. The blog calendar question stops being how many posts shipped this month. It becomes how much of the prioritized library is live, indexed, and converting.
If You Manage Multiple Locations: The Coordination Cost Math
This section is for operators running five sites or more. Single-location practices can skip ahead; the math below only matters when N gets large enough that duplication compounds. The consolidation pressure that makes this math urgent is the same pressure already named: 34.5% of physicians now work in hospital-owned practices, with 15.1% of those acquisitions landing after 2019 6. System competitors are running one plan against your N plans.
 Percentage of physician practices acquired since 2019 showing consolidation: 15.1%
Percentage of physician practices acquired since 2019 showing consolidation: 15.1%
The table below uses variables, not invented dollars, because retainer pricing and CPL benchmarks vary too widely across specialties and metros to fix in print. Plug the group's actual numbers into the variables. The pattern that emerges is the point.
| Cost or effort category | Per-location retainer model | Account-level execution |
|---|---|---|
| Keyword research | N agencies × one keyword map each, with overlapping service-line and metro terms | One keyword map covering every service line and metro, refreshed quarterly |
| Google Ads management | N separate accounts, fragmented conversion data, sister locations bidding against each other in shared geos | Single MCC, shared negative-keyword lists, geo-fenced campaigns, consolidated conversion training |
| Compliance review | N reviewer interpretations of FTC substantiation, asset-by-asset, at the publish stage | One substantiation gate inside the brief, cleared once, applied to every channel |
| Backlink prospecting | N parallel outreach lists targeting the same medical societies and condition publishers | One outreach program building root-domain authority that every service-line page inherits |
| Reporting | N dashboards, N attribution models, manual roll-up to portfolio view | One reporting layer with location, service-line, and account-level cuts from the same data |
| Time-to-publish | Weeks per asset, gated by the slowest reviewer in the chain | Days per asset when substantiation is decided in the brief |
The coordination tax is not the retainer line item. It is the duplicated research, the auction self-competition, and the review cycles that stretch a 240-page content library across two years instead of two quarters. For a 30-site group, the difference between shipping eighty assets a quarter and shipping eight is the difference between organic visibility that compounds and organic visibility that flatlines while system competitors keep publishing 10. The CFO question to expect: what is the unit economics of one more location under the current model versus a centralized one? If the answer is that adding a location adds a proportional retainer line and a proportional reviewer queue, the model is already losing to the systems acquiring the practice next door.
See How Leading Health Systems Scale Medical Marketing Across Every Location
Get a data-driven walkthrough of unified marketing systems proven to coordinate content, PPC, and SEO for multi-site medical practices—without increasing team headcount.
Measuring Return Against Patient Lifetime Value, Not Channel CPL
Cost per lead is the metric every channel reports because every channel can measure it cleanly. It is also the metric most likely to mislead a CFO. A $42 CPL on a paid search campaign for cosmetic injectables and a $38 CPL on a paid search campaign for Mohs surgery look comparable on a dashboard. They are not. The Mohs patient enters a long-term dermatology relationship with annual skin checks, repeat procedures, and family-member referrals. The injectables patient may convert once and never return. Pricing the two channels against the same CPL benchmark misallocates budget at the account level.
Healthcare ROI work has long argued that investment decisions in clinical operations should be measured against multi-period value capture rather than single-event cost, because the unit economics of patient relationships compound over years rather than transactions 9. The same logic applies to marketing spend. The question for a 30-site multispecialty group is not what each location's CPL was last quarter. It is what the lifetime value of an acquired patient looks like by service line, by payer mix, and by acquisition channel, and which combinations the budget should weight toward.
That reframe changes what gets reported to the CFO. Three numbers matter at the account level: blended patient acquisition cost across all channels feeding a given service line, projected lifetime value of that service line's patient cohort, and the ratio between them by location. Channel-level CPL becomes a diagnostic for the marketing team, not a headline for the board deck. Educational content compounds in this model because the organic patients it acquires carry no recurring acquisition cost on the second visit, the third, or the referral, which is the mechanism behind the patient-acquisition gains observed in content-led healthcare programs 11. The operational takeaway is concrete: rebuild the reporting layer so location and service-line cuts roll up to LTV-to-CAC, not to channel CPL, before the next budget cycle closes.
What Predicts Scaling Success in Patient-Facing Programs
A 2025 peer-reviewed study of patient-facing digital health programs identified 18 distinct success factors that predict whether a program scales across categories ranging from wellness tools to regulated therapeutics, with the relative weight of each factor shifting by category 2. For wellness-adjacent service lines, business flexibility and partnership velocity dominate. For regulated clinical programs, validation of health impact and regulatory fit dominate. The cross-category constant is that programs which cannot demonstrate substantiated outcomes do not scale, regardless of channel sophistication.
Three of those factors map directly to the operating model VPs of Marketing are designing right now. Validation comes first: every service-line claim that drives a paid headline, an organic page, or a backlink anchor needs an evidence file behind it before publication, not after a complaint 5. Partnership infrastructure comes second: link acquisition, condition-publisher relationships, and patient advocacy placements compound only when one team owns the prospect list across the whole footprint, not when twelve locations chase the same medical society. Reporting discipline comes third: programs that measure return as multi-period patient value, not single-event lead cost, allocate budget toward the service lines that actually compound 9.
Groups that get those three right ship the prioritized content library, win the auctions they should be winning, and inherit the link equity that paid placements cannot buy. Groups that do not stay stuck publishing eight assets a quarter while the system across town publishes eighty.
Frequently Asked Questions
References
- 1.A Guide to Basic Digital Strategies | AMA.
- 2.Success factors and measures for scaling patient-facing digital ....
- 3.Physician Practice Characteristics in 2024.
- 4.Primary Healthcare Marketing: A Bibliometric Study and Research ....
- 5.Health Products Compliance Guidance - Federal Trade Commission.
- 6.Charted: The rise of hospital-owned physician practices.
- 7.The impact of marketing strategies in healthcare systems - PMC - NIH.
- 8.AMA examines decade of change in physician practice ownership ....
- 9.The development of the concept of return-on-investment from large ....
- 10.Physician Practice Consolidation Driven By Hospitals, Not Private Equity.
- 11.Capturing the world of online health information.