Key Takeaways
- Local SEO works at scale when run as one templated production system with location variables, not fifty parallel page projects competing for the same content team.
- Review volume drives booking behavior more than average star rating, so event-triggered solicitation at every site outperforms passive monitoring of ratings 8.
- Star ratings track clinical quality signals, so review patterns should route to both marketing response workflows and clinical leadership review 6.
- Service line landing pages should be built once as a master asset and localized through structured data fields, not rebuilt market by market 10.
- Targeted digital advertising reaches older patient populations faster and often more cost-effectively than direct mail and traditional outreach methods 7.
- Online scheduling integrated across every site converts discovery into booked visits, since practices offering digital access attract more new patients 8.
- Omnichannel coordination requires unified patient identity, shared data, and one content library feeding every channel, not more platforms layered on silos 2.
- Patient experience data drives retention since satisfied patients are 28% less likely to switch providers, making it a high-leverage marketing asset 3.
- Account-level execution replaces per-location agency stacks by eliminating duplicated content, fragmented PPC accounts, and reconciliation overhead that grows with each new site 1.
The Coordination Problem Behind Every Multi-Site Marketing Plan
A dermatology group running 47 clinics does not have 47 marketing problems. It has one marketing problem expressed 47 different ways: inconsistent location pages, uneven Google Business Profile data, three different agencies producing service line content in three different voices, and a paid media account where bid strategy varies by whichever vendor inherited each market. The tactics are not the issue. The coordination is.
Research on group practices documents this directly. A systematic review of multi-site care delivery found that group structures can improve access and operational efficiency, but introduce complexity and potential depersonalization when execution drifts across sites 11. Marketing inherits the same risk. Patient-facing signals fragment faster than headquarters can correct them.
The consumer environment makes that drift expensive. Patients now shop for care across multiple digital sources before booking, compare options the way they compare retail, and switch providers more readily than in prior decades 9. A clinic with stale hours, two reviews, and a generic service page loses to a competitor with disciplined local execution, regardless of clinical quality.
The nine ideas in this piece are not standalone tactics. Each one is presented as an account-level system: one plan at the top, consistent execution at every site, and a measurable patient acquisition or retention outcome at the bottom.
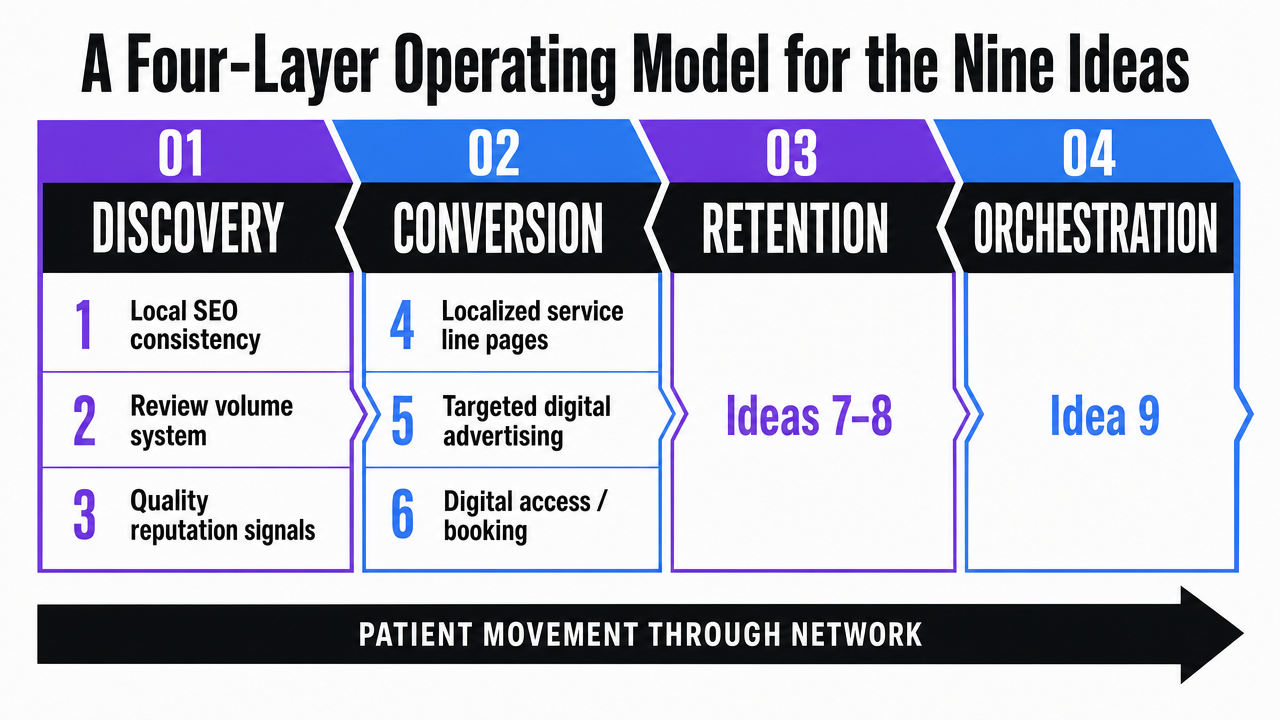
A Four-Layer Operating Model for the Nine Ideas
The nine ideas that follow are organized into four layers that match how patients actually move through a healthcare network: discovery, conversion, retention, and orchestration. McKinsey's analysis of consumer-led healthcare strategy documents that patients now research care across multiple digital sources and switch providers more readily than in prior decades, which means each layer carries real revenue exposure if it drifts 9.
Discovery covers how a clinic gets found: local SEO consistency, review volume as a production system, and reputation signals tied to clinical quality. These are ideas one through three. Conversion covers what happens after discovery: service line landing pages built once and localized at the edge, targeted digital advertising in place of mass outreach, and digital access as the booking layer. Those are ideas four through six.
Retention covers the work that keeps a patient inside the network: coordinated omnichannel journeys across sites and patient experience data used as a retention engine. Those are ideas seven and eight. Orchestration is the ninth idea on its own: the account-level execution model that makes the other eight repeatable across every location without per-site rebuilds.
 Visualize the four-layer operating model (Discovery, Conversion, Retention, Orchestration) and map each of the nine ideas to its layer, giving readers a structural map of the article
Visualize the four-layer operating model (Discovery, Conversion, Retention, Orchestration) and map each of the nine ideas to its layer, giving readers a structural map of the article
Idea 1: Treat Local SEO as One Template, Not Fifty Projects
The fastest way to spot a multi-location group with no central marketing operating model is to audit ten of its location pages. NAP fields drift. Service line lists vary by whichever office manager last edited the GBP profile. Schema markup exists on some pages and not others. Three locations have FAQ sections, the rest have none. None of this is a strategy problem. It is a templating problem.
The foundational components of healthcare local SEO are well understood: a search-optimized website, consistent location data, structured content, and review integration 10. What changes at scale is that those components stop being a checklist and become a production specification. A urology group with 60 sites cannot afford 60 versions of a vasectomy page. It needs one page architecture, one schema template, one set of trust signals, and a localization layer that swaps clinician bios, addresses, insurance accepted, and catchment-area language at the edge.
The operational test is simple. When a new clinic opens, the location should inherit the full template—page structure, schema, GBP categories, internal linking, review widget—on day one, not after a 90-day backlog. Multi-location groups that get this right run local SEO as a single account-level system with location variables, not as fifty parallel projects competing for the same content team.
Idea 2: Manage Review Volume as a Production System
Most multi-location groups treat reviews as a passive metric. The marketing team watches the average star rating, flags outliers, and assumes the work is done. The evidence says they are measuring the wrong variable. A JMIR Medical Informatics analysis of online physician reviews and outpatient visit volume found that the number of reviews was more effective in influencing patient decisions than the overall review rating 8. Volume, not valence, moved booking behavior.
That finding reframes reputation as a production problem. A 4.7-star clinic with 12 reviews loses to a 4.4-star clinic with 380 reviews in the same zip code. The first clinic is not underperforming on quality. It is underperforming on solicitation volume. Independent research on how online physician reviews shape decision making reinforces the pattern: both review count and content drive perceived quality and selection intent 5. Patients read reviews as a signal that other patients exist.
The operational fix is to make review requests an event-triggered system at every site, not a per-clinic project. Every completed visit fires a request through the same channel mix, on the same cadence, with the same fallback logic if the first message goes unread. A 60-location physical therapy network running this as a central workflow can produce thousands of new reviews per quarter. The same network running it as a site-level discretionary task produces a long tail of underperforming GBP profiles and a few overperforming ones, which is exactly the inconsistency patients notice when they shop across providers 9.
The metric to watch is monthly review velocity per location, segmented by service line. Average rating is a lagging indicator. Volume is the production line.
Idea 3: Tie Reputation Signals to Clinical Quality, Not Vanity Scores
Star ratings get treated as a marketing scoreboard. The research suggests they are closer to a clinical signal. A Journal of Marketing study summarized by the American Marketing Association found that online physician ratings are robustly and positively associated with conventional measurements of physician credentials, adherence to clinical guidelines, and patient outcomes 6. Reputation is not decoupled from quality. It tracks it.
That changes how a multi-location group should govern reviews. Negative review patterns concentrated at one site are not just a marketing problem to suppress. They are an operational signal worth routing to clinical leadership before the marketing team drafts a response template. Review content analysis at the network level can surface which sites have rising complaint themes around wait times, billing surprises, or specific clinicians, and the underlying study of review valence and content shows those themes shape selection intent at the next patient's search 5.
The operational shift is to wire reputation data into two workflows at once: a marketing response system and a clinical quality review. A 30-site behavioral health network running this loop catches a billing-process complaint cluster in one market within weeks instead of quarters. The marketing payoff is durable. Sites that fix the underlying issue stop generating the reviews that depress conversion in the first place, and the ones that earn praise produce content that other prospective patients use as a quality proxy 6.
Test Unified Campaign Execution for All Locations
Experience coordinated multi-location marketing results using real campaigns during your free trial.
Idea 4: Build Service Line Landing Pages Once, Localize at the Edge
A 40-site orthopedic group launching a new sports medicine service line should not be commissioning 40 landing pages. It should be commissioning one. The page architecture, the clinical content, the trust signals, the schema, the conversion components, and the SEO depth all belong in a single master asset. What varies by site is narrow: clinician roster, address, parking notes, insurance accepted, intake hours, and the few sentences that reflect local catchment language.
The peer-reviewed literature on healthcare digital marketing treats the search-optimized service page as foundational, but the guidance assumes a single practice 10. At fifty sites that same advice becomes an operations problem. Groups that build pages site by site end up with a backlog measured in quarters and a content quality curve that drops with every new market. Groups that build once and localize at the edge ship a new service line across the entire network in days.
The localization layer is where most multi-site operators get this wrong. Treating it as copywriting work fragments the program; treating it as structured data populates a unified template from a location database. Clinician name, NPI, languages spoken, and accepted plans flow in as fields. Body copy stays consistent. Patients comparing options across digital sources see the same depth of information at every site, which is what consumer-led healthcare research describes as table stakes for retaining shoppers across the discovery process 9.
Idea 5: Run Targeted Digital Ads in Place of Mass Outreach
The assumption that older patient populations are unreachable through digital channels keeps a lot of multi-location marketing budgets stuck in direct mail, local print, and broadcast spend. A randomized study comparing targeted web-based advertising with traditional recruitment methods for enrolling older adults into clinical trials found the opposite. Targeted digital ads recruited participants faster, and in several conditions more cost-effectively, than mailings and conventional outreach 7. The audience that operators most often assume requires paper actually responded better to precision digital targeting.
For a multi-location group, the implication is operational, not philosophical. Mass outreach scales by spending more money in more zip codes. Targeted digital media scales by tightening match criteria—catchment radius, service line intent, insurance match, demographic profile—and letting the platform allocate impressions where conversion probability is highest. A 22-site primary care network running geo-fenced search and audience campaigns against Medicare-eligible patients can shift budget across markets weekly based on cost per booked visit, which no direct mail program can match.
The coordination problem at scale is account structure, not creative. Groups that let each market run its own ad account end up with duplicate keywords bidding against each other, inconsistent landing page destinations, and conversion tracking that breaks at the network level. Centralizing the account, the audience definitions, and the creative library—then localizing offer, clinician, and location—turns paid media into one workstream with 22 dials instead of 22 separate programs. Cost per acquisition becomes a number the VP of marketing can actually compare across sites.
Idea 6: Make Digital Access the Conversion Layer
Discovery without booking is a leak. A patient who finds a clinic page, reads the reviews, and then has to call a phone tree to schedule has been handed back to the competition. The JMIR Medical Informatics study on outpatient visit volume found that practices offering online services attracted more new patients, alongside the review-volume effect 8. Digital access is not a convenience feature. It is where the conversion happens.
At one site, online scheduling is a vendor decision. At fifty sites it is an integration problem. The booking widget has to read each location's provider availability, service line eligibility, insurance accepted, and intake protocol in real time, then write back to whatever EHR or practice management system each market uses. Multi-location groups that solve this once at the account level shrink time-to-appointment from days to minutes across the entire network. Groups that let each site bolt on its own scheduler end up with broken handoffs and conversion rates that vary by zip code for reasons no one can explain.
The consumer expectation makes the investment unavoidable. Patients researching care across multiple digital sources now expect retail-grade booking, transparent pricing where available, and same-session confirmation, and they switch providers when those expectations are not met 9. Digital access turns the discovery layer into revenue.
Idea 7: Coordinate Omnichannel Journeys Across Sites
Omnichannel in healthcare is not a content calendar that runs across more channels. A peer-reviewed review of omnichannel interaction in care services defines it as the integrated use of digital and physical channels with shared data and analytics, designed to deliver a consistent service experience across every touchpoint a patient uses 2. Channel integration, data sharing, and personalization are the operational components, not the marketing department's choice of platforms.
For a multi-location operator, that definition cuts in a specific direction. A patient who searches in one market, books at a second site, receives intake reminders by SMS, switches to a portal message for a clinical question, and shows up at a third location for a referral should encounter the same brand, the same record, and the same access logic at every step. Most networks fail this test because each channel reports to a different vendor and each site treats the patient as a new contact. The review notes that organizational silos and uneven data sharing are the most common implementation barriers 2.
The coordination work is in the middle layer: a unified patient identity that travels across sites, a content library that feeds email, SMS, portal, and call-center scripts from one source, and journey logic that knows what was sent yesterday before sending the next message today. A 90-site dermatology platform running this centrally retires the duplicate-outreach problem that erodes trust at the site level.
See How Enterprise Healthcare Operators Orchestrate Multi-Location Marketing at Scale
Connect with experts to review unified strategies that automate content, PPC, and SEO execution for all your locations from a single platform—eliminating manual coordination and accelerating measurable outcomes.
Idea 8: Use Patient Experience Data as a Retention Engine
A McKinsey survey of more than 3,000 US healthcare consumers found that satisfied patients were 28% less likely to switch providers than unsatisfied ones, which makes experience data one of the highest-leverage retention assets a multi-location group owns 3. Most networks treat it as a quality-department artifact. The marketing team sees the dashboard once a quarter and moves on.
That pattern leaves money on the table. A peer-reviewed review of the business case for patient experience consolidates evidence that higher patient-reported experience tracks with better adherence, lower readmissions, and stronger financial performance, which means the same data that drives clinical improvement also drives lifetime value 4. For a 75-site multispecialty group, the question is not whether to collect experience data. It is whether the marketing operating model can act on it before the next patient decides to leave.
The operational shift is to route experience signals into three workstreams at once. Site-level scores feed clinical quality review. Service-line themes feed content production, so the next patient searching that specialty encounters answers to the friction points the last cohort flagged. Promoter-level patients feed review-solicitation and referral workflows, turning the satisfied 28% into the volume that the JMIR study identified as the dominant booking signal earlier in this piece 3. Detractor-level patients trigger recovery outreach before they post publicly.
The metric a VP of marketing can actually defend is retention rate by site and service line, paired with experience score deltas quarter over quarter. Sites where both move together are compounding. Sites where they diverge expose either a measurement problem or an execution gap that no amount of acquisition spend will fix.
 Reduction in provider switching for satisfied patients
Reduction in provider switching for satisfied patients
Reduction in provider switching for satisfied patients
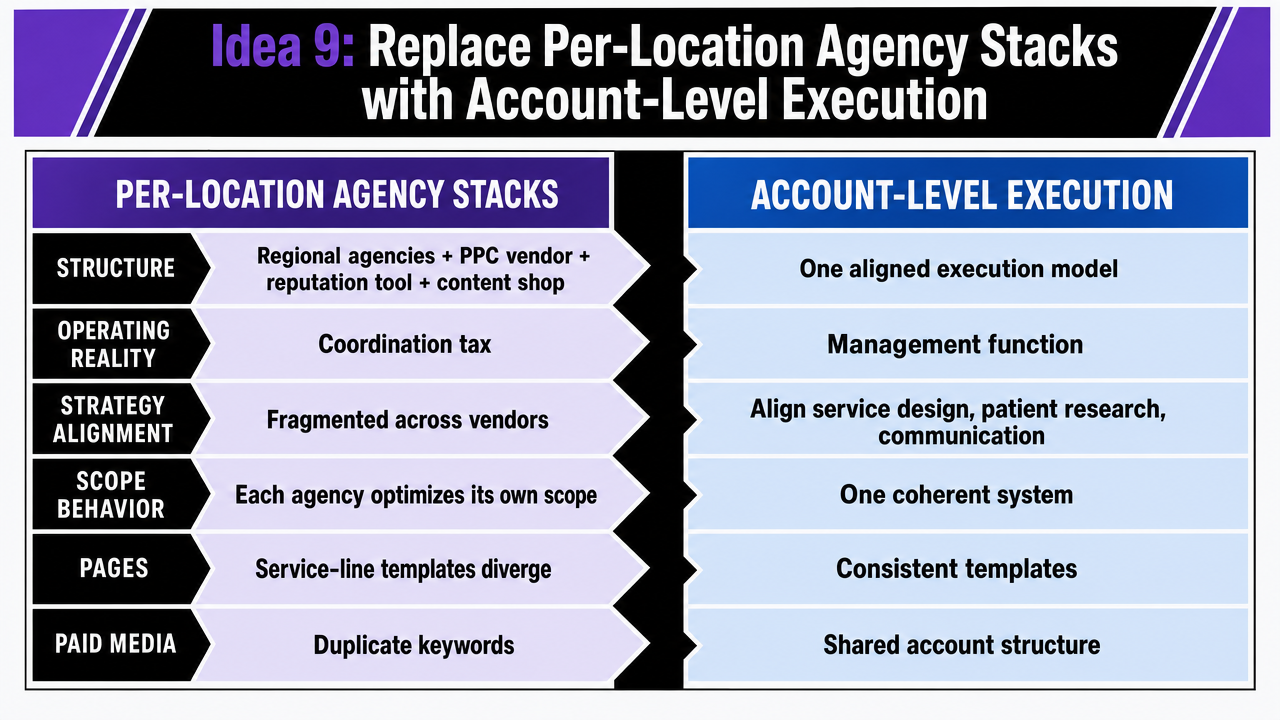
Idea 9: Replace Per-Location Agency Stacks with Account-Level Execution
The eighth idea ended at the site level. This one moves up the org chart, because the operating model under the first eight ideas is the variable that decides whether they ship at scale. A 50-site multispecialty group running three regional agencies, a national PPC vendor, a separate reputation tool, and a content shop billing per location is not running a marketing program. It is running a coordination tax.
The peer-reviewed framing of marketing in healthcare treats strategy as a management function that must align service design, patient research, and communication into one coherent system 1. That alignment is structurally impossible when execution is fragmented across vendors charging per site. Each agency optimizes its own scope. Service-line page templates diverge. Paid media accounts duplicate keywords. Review responses arrive in three voices. The VP of marketing spends the quarter reconciling reports instead of moving acquisition cost.
The economics make the case before the quality argument does. The cost driver in a per-location agency stack is not the work itself. It is the duplication.
| Cost driver | Per-location agency stack | Account-level execution |
|---|---|---|
| Content production | Billed per site, per service line | One master asset, localized at the edge |
| GBP and local SEO management | Per-site retainer line | One template, one workflow, N location variables |
| Landing page builds | Rebuilt for each new market | One architecture, location data populates fields |
| PPC account management | Per-market fees, fragmented accounts | One account, geo-targeted, centralized creative |
| Reporting and analytics | Reconciled across vendors monthly | One dashboard across sites and channels |
| Pricing structure | Per-location retainer (X) × locations (N) | Account-level fee independent of site count |
The patient-side argument is the same one that runs through the previous eight ideas. Consumers research across multiple digital sources, compare options, and switch when discovery feels uneven 9. A unified account-level operating model is the only structure that keeps signals consistent at every site as the network adds clinics, retires service lines, or enters new markets. Vectoron is one example of this category—a single growth program covering content, SEO, PPC, and backlinks across every location, with a two-week trial at $599/mo afterward—built so the marketing org scales by adding sites, not headcount.
 Render the comparison table between per-location agency stacks and account-level execution as a clean visual side-by-side, reinforcing the operational and cost argument made in the section
Render the comparison table between per-location agency stacks and account-level execution as a clean visual side-by-side, reinforcing the operational and cost argument made in the section
Failure Modes That Quietly Erode Multi-Site Marketing Programs
The programs that look healthy at the network level often hide three specific failure modes at the site level.
- Silent template drift. A location page changes once because a regional manager wanted a different headline, and the rest of the network keeps shipping the old version. Six months later, ten sites have diverged and no one owns the reconciliation.
- Duplicate outreach. Each channel vendor pulls its own patient list, so a single patient gets three SMS reminders, two emails, and a postcard for the same appointment. The omnichannel literature names this directly: shared data and unified patient identity are the prerequisites for a consistent experience, and most multi-site groups fail the prerequisite 2.
- Acquisition spend covering retention leaks. Sites with weak experience scores get more paid media instead of clinical or operational repair, even though the evidence ties experience to adherence, lower readmissions, and financial performance 4. The budget grows. The leak does not close.
Where to Start Without Stalling the Network
The trap in adopting all nine ideas at once is the same trap that creates the coordination problem in the first place: too many parallel projects, no single owner, no measurable sequence. Multi-location operators move faster by running three plays in order.
- Audit ten location pages and ten GBP profiles against one template and fix the drift before adding new work.
- Wire review solicitation into the visit workflow at every site so volume becomes a daily output, not a quarterly campaign 8.
- Consolidate the vendor stack into one account-level plan so service line pages, paid media, and reporting share a spine 1.
Acquisition spend, content production, and experience data align after that foundation, not before it.
Frequently Asked Questions
References
- 1.The impact of marketing strategies in healthcare systems.
- 2.An Overview of Omnichannel Interaction in Health Care Services.
- 3.Marketing in healthcare: Improving the consumer experience.
- 4.Examining the Business Case for Patient Experience.
- 5.Insights Into the Impact of Online Physician Reviews on Patients’ Decision Making Process.
- 6.How Online Reviews Influence Doctor Selection [Quality Insights].
- 7.Comparison of Targeted Web-based Advertising vs Traditional Recruitment Methods for Clinical Trials.
- 8.How Online Reviews and Services Affect Physician Outpatient Visits.
- 9.Consumers rule: Driving healthcare growth with a consumer-led strategy.
- 10.Digital Marketing for Private Practice: How to Attract New Patients.
- 11.Group practice impacts on patients, physicians and healthcare systems.