Key Takeaways
- Patient acquisition stalls beyond ten locations because the limiting factor shifts from channel performance to integration across data, content, scheduling, and compliance operating as one system.
- A scalable program rests on four components: a unified data layer with one patient record, a compounding content engine, self-scheduling conversion infrastructure, and compliance embedded into templates.
- Per-location agency retainers fail because coordination costs grow linearly with sites while output does not, whereas account-level production decouples capacity from headcount 4.
- Operators should next quarter audit three signals: consistent cost-per-booked-appointment by service line, the share of digital leads booking without callbacks, and whether the content library grows between contracts.
Why Channel Optimization Stops Working at the Tenth Location
Most multi-location healthcare operators encounter a ceiling around the tenth site. While individual channel efforts like paid search, SEO, and social media continue, patient acquisition cost rises, and marketing teams expand disproportionately to booked appointments.
The common response is to intensify channel-specific optimization. However, this approach yields diminishing returns because the core issue shifts from individual channel performance to integration. For a single site, channel effectiveness is paramount. Across ten, twenty-five, or seventy-five locations, the critical factor becomes whether data, content, scheduling, and compliance function as a unified system or as disparate, loosely connected operations.
Research on omnichannel healthcare engagement highlights this: inadequate integration of processes, technologies, and personnel leads to fragmented patient experiences and increased operational complexity, not merely duplicated effort 1. This fragmentation is a critical failure mode that flattens conversion rates and inflates cost-per-booked-appointment as the operational footprint expands.
This article examines online lead generation as a production system comprising four essential components: a unified data layer, a compounding content and SEO engine, conversion infrastructure centered on self-scheduling, and compliance integrated into the workflow. Each component has a distinct failure mode at scale, can be measured, and cannot be optimized by simply adding more channel specialists or per-location retainers.
The following sections detail this architecture, the economic factors that render the agency-retainer model unsustainable beyond ten sites, and the strategic decisions operators must make to ensure their marketing programs scale effectively rather than stall.
The Four Load-Bearing Components of a Patient Acquisition System
From Channel Mix to Production System
A channel mix identifies sources of impressions, whereas a production system defines how those impressions consistently convert into booked appointments at a predictable unit cost across all locations. This distinction is crucial because channel optimization faces diminishing returns when the underlying production capacity is fixed. For instance, adding another PPC vendor won't boost output if content creation, scheduling, and compliance review processes are already at their limit.
McKinsey's research on hybrid B2B sales coverage provides a relevant parallel: organizations that integrated digital demand generation, inside sales, and field interactions achieved up to 50% more revenue than those treating each channel as a separate function 4. While this finding pertains to B2B, the structural lesson applies: integration surpasses isolated channel tuning when the objective is repeatable scale.
For multi-location healthcare operators, this integration spans four critical components:
- a unified data layer connecting traffic, leads, and bookings from every site into a single patient record;
- a content and SEO engine that continuously generates service-line and location pages;
- conversion infrastructure that directs intent to confirmed appointments, primarily through self-scheduling; and
- a compliance layer that governs claims, endorsements, and patient data without impeding campaign approvals.
Each component is vital, and isolating any one from the others is a common reason why scaling programs fail.
Where Per-Location Agency Retainers Break
The per-location agency model assumes that a successful strategy at one site can be replicated by purchasing the same service multiple times. However, the cost of coordinating numerous agencies often outpaces the output they collectively generate.
Consider a thirty-site operator managing three regional agencies and two specialist vendors. Each site typically has its own monthly reporting call, and each agency uses distinct analytics setups, tagging conventions, and creative brief formats. Approvals for a single service-line landing page might involve four to six individuals, delaying campaign changes significantly. This inefficiency isn't a fault of individual agencies but rather a structural cost of managing a footprint as a collection of independent accounts.
Under this model, patient acquisition costs escalate. Each additional site increases account-management overhead, slows production cycles, and dilutes data needed for accurate attribution. While centralized in-house teams can mitigate coordination issues, they face a different limitation: specialist headcount must grow proportionally with service lines, geographies, and channel complexity.
The alternative is a system that decouples production capacity from headcount by managing strategy, content, technical SEO, paid media, and compliance review at the account level, rather than per location. This structural shift makes the subsequent components—data, conversion, and compliance—economically viable across a large operational footprint.
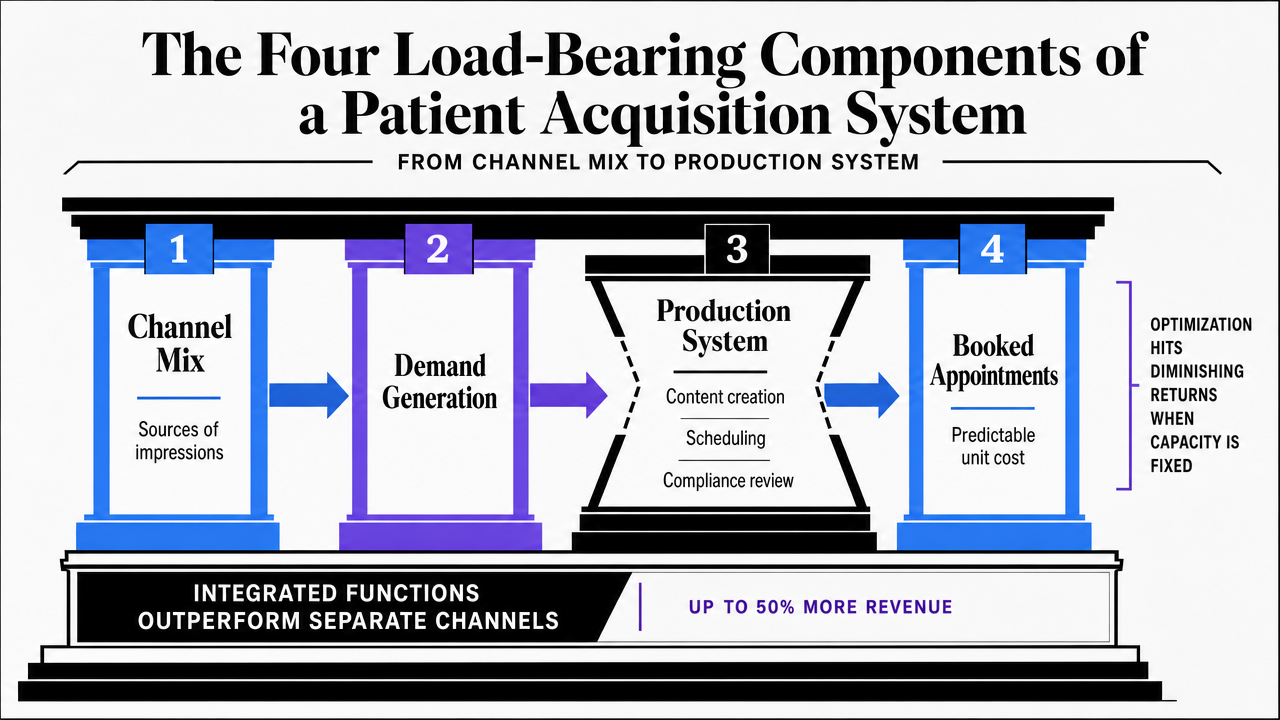 Visualize the four load-bearing components of the patient acquisition system as described in the section, giving readers a structural reference for the rest of the article
Visualize the four load-bearing components of the patient acquisition system as described in the section, giving readers a structural reference for the rest of the article
The Unified Data Layer: One Patient Record Across the Footprint
The data layer is the foundational element that determines whether other system components can truly compound. Without it, a forty-site operator manages forty separate analytics setups, attribution windows, and definitions of a qualified lead. With a unified data layer, this is streamlined to one.
The omnichannel healthcare review highlights the clinical necessity: inadequate integration of processes, technologies, and people results in fragmented patient experiences and operational complexity, not just redundant efforts 1. Data layer fragmentation manifests downstream as wasted media spend on existing leads, inconsistent service-line attribution across regions, and disparate CAC calculations across reports.
A unified data layer consolidates four key streams into a single patient record at the account level:
- Site-level traffic and engagement data from web analytics and Search Console are stored in one warehouse.
- Paid media spend, impressions, and conversions are reconciled against booked appointments, not just form fills.
- Scheduling and CRM events complete the loop, identifying which leads generate revenue.
- Compliance metadata—consent status, channel preferences, authorization—is integrated, ensuring downstream campaigns automatically adhere to necessary permissions.
The operational litmus test is straightforward: Can the head of marketing quickly retrieve cost-per-booked-appointment by service line across all sites, using a consistent definition of 'booked' that aligns with operations? If this requires multiple vendors and manual spreadsheets, the data layer is the bottleneck, regardless of channel performance reports.
Two common structural errors are treating the CRM as the data layer (it's a workflow tool, not a comprehensive data warehouse) and allowing each agency or vendor to define its own conversion events. Standardizing conversion definitions at the account level is essential; otherwise, aggregated performance reports are unreliable.
Test Autonomous Lead Generation Workflows Risk-Free
Experience measurable lead growth on real campaigns before making a commitment.
A Content and SEO Engine That Compounds Across Service Lines
Content investment can function either as infrastructure or as inventory. Infrastructure, like service-line pages, location pages, and clinical explainers, compounds over time, continuously generating organic traffic and bookings. Inventory, such as campaign-specific content for promotions, depreciates once the campaign concludes.
Most multi-location operators inadvertently manage content as inventory. An agency proposes a quarterly plan, delivers a set number of pieces, invoices, and the cycle restarts with little carryover. Each new quarter effectively begins from scratch because previous content was treated as a temporary campaign asset, not a permanent addition to a service-line library. The agency-retainer model often reinforces this by billing for activity rather than for the enduring value of the content footprint.
The system alternative views content production as a continuous engine scaled to the account's complete service-line and location matrix. For example, a twenty-five-site operator with six service lines has a potential need for 150 location-and-service pages, plus supporting clinical, comparison, and decision-stage content. This comprehensive library is built once and maintained, rather than being recreated each quarter.
The compounding effect of this approach is well-documented. Research on digital marketing in hospitals indicates that a sustained digital presence attracts new patients, expands business, fosters patient trust and loyalty, and enhances brand awareness—benefits that accumulate over time 5. McKinsey's analysis of high-performing commercial models similarly concludes that successful organizations at scale employ data-driven, repeatable engines for personalized outreach, rather than relying on one-off quarterly campaigns 10.
Two operational metrics distinguish a compounding engine from a campaign cadence:
- A consistent number of pages published per week over at least four quarters, with ongoing refreshes of existing content.
- A growing share of organic bookings attributed to pages older than twelve months.
If content output drops to zero between agency contracts, the program is operating on an inventory model.
Conversion Infrastructure: Self-Scheduling as the Choke Point
The Form-Fill Fallacy
In healthcare lead generation, the contact-form submission is often mistakenly considered the conversion event. In reality, a form fill is merely a request for contact. The true conversion—a booked appointment on a clinician's calendar—requires one or two additional manual steps.
This gap between form submission and booked appointment is where multi-location operators lose valuable prospects. A patient submits a form late in the evening, and the lead enters a queue, is assigned the next morning, and receives a callback hours later. By then, many prospects have already booked elsewhere, abandoned their search, or are no longer answering unknown numbers.
Managing to form fills also distorts channel performance reports. Paid search might appear successful due to high form volume, but the reports often fail to show that only a fraction of these forms convert to scheduled visits, or that conversion rates from form to appointment vary significantly across sites based on call-center staffing. This reliance on a proxy metric can lead to misinformed economic decisions for the entire program.
Why Online Self-Scheduling Is an Access Issue, Not a Convenience Feature
The academic literature on automated patient self-scheduling frames it as more than a convenience. A scoping review identifying barriers and facilitators across patient, provider, organizational, and technological levels positions delays in access as a contributor to poor outcomes, making scheduling a quality issue rather than a mere UX preference 2. A 2025 evaluation of online appointment scheduling in hospitals reached a similar conclusion: digital scheduling enhances patient satisfaction and improves care efficiency by removing the phone-call bottleneck between patient intent and appointment 3.
For multi-location operators, the implication is clear. Without patient-facing self-scheduling, every booked appointment necessitates a callback, introducing three significant drop-off points:
- the delay between submission and outbound call,
- the low answer rate for return calls, and
- the complex calendar negotiation that often requires multiple contacts.
These issues compound across multiple locations. A program with thirty sites and an average 24-hour callback window will have a structurally limited conversion rate, regardless of media spend efficiency.
The same research acknowledges an equity concern: automated self-scheduling can disadvantage older adults and those with low digital literacy if it's the sole option, and poor design can misdirect patients to inappropriate appointment types 2. The solution is parallel paths: self-scheduling as the default for digitally originated leads, with phone and assisted scheduling maintained as full-service alternatives. Operators who implement self-scheduling effectively often observe a reduction in phone channel usage, freeing call-center capacity for higher-intent or more complex cases.
The key metric for effective self-scheduling is the conversion ratio from web session to confirmed appointment, measured at the service-line level and aggregated across the account. If this ratio isn't a primary marketing dashboard metric, the program is likely still managing to form fills rather than actual appointments.
On-Site Behavior as a Conversion Lever
A website is more than a digital brochure with a scheduling button; it's the interface where patient intent is refined into specific service-line and location selections. The site's information architecture significantly influences conversion rates.
Behavioral analysis of hospital website visitors, using clickstream and Bayesian modeling, reveals that on-site search queries and navigation paths clearly indicate patient intent. This insight can guide structural changes to improve the visibility of relevant information 6. For multi-location operators, this means internal search logs and top navigation paths are diagnostic tools, not just vanity metrics. They show which service lines patients seek at which locations, identify content gaps leading to dead ends, and highlight pages receiving the most pre-scheduling traffic.
Two consistent changes improve the conversion ratio:
- Scheduling entry points should be present at the moment of decision—on service-line pages, location pages, and clinician profiles—rather than solely in the global header.
- On-site search results should link directly to bookable destinations, not just content indexes.
Both are information-architecture decisions, not full redesigns, and both can be measured against the web-session-to-appointment ratio.
Compliance by Design: One Decision Framework, Not Scattered Warnings
Compliance should be integrated as a routing rule within the production workflow, applied once and inherited universally, rather than existing as a warning sticker on every campaign. Three regulatory areas primarily govern online lead generation in healthcare, each addressing a different aspect of marketing activity.
The first concerns the use of protected health information (PHI) for marketing. HIPAA's Privacy Rule generally mandates patient authorization when a covered entity receives financial remuneration for promoting a third party's product or service, with specific exceptions for treatment and certain healthcare operations 7. Operationally, this means audience-building from clinical data, third-party sponsored content, and remarketing lists derived from PHI all require explicit authorization workflows linked to the patient record, not a checkbox added later at the campaign level.
The second addresses the substantiation of claims about services, outcomes, or products. The FTC's health products compliance guidance states that advertisers cannot make claims through testimonials or expert endorsements that they couldn't substantiate directly, and typical-versus-exceptional results must be presented honestly 8. For multi-location operators, this prohibits service-line pages from quoting outlier outcomes as typical and restricts how before-and-after content from one site can be syndicated to others.
The third involves disclosing material connections in endorsements. The FTC's Endorsement Guides require clear and conspicuous disclosure when a relationship between an endorser and a marketer could influence consumer perception and isn't otherwise obvious 9. Clinician-authored content, paid influencer placements, and employee reviews all trigger disclosure rules that are more effectively enforced at the template level than per campaign.
CMS Conditions of Participation provide an overarching framework, governing patient rights and governance standards that influence how aggressively Medicare-participating hospitals can pursue acquisition tactics 11. Practically, compliance is embedded into content production templates, patient record consent fields, and media stack audience-build logic. Once these three areas are correctly configured, compliance review shifts from a per-campaign approval queue to an inherent property of the system itself.
See How Leading Healthcare Operators Scale Lead Generation Without Added Overhead
Request a walkthrough of the latest AI-driven marketing operations platform designed for multi-location healthcare and agency growth teams seeking measurable, cost-efficient online lead generation at scale.
If Operators Run More Than Ten Sites: The Coordination Economics
Beyond ten sites, the primary question shifts from which marketing model performs best for a single P&L to which model can withstand the complexities of coordination.
Three common structures are observed: per-location agency retainers, centralized in-house teams, and an account-level production system that integrates strategy, content, media, and compliance across the entire footprint. Each scales differently. The table below uses variables to illustrate cost growth patterns rather than specific figures.
| Cost driver | Per-location agency retainers | Centralized in-house team | Account-level production system |
|---|---|---|---|
| Production cost | Retainer × locations | FTE × specialist roles (SEO, content, paid, analytics, compliance) | Flat platform fee + production volume |
| Coordination cost | Linear: account managers, reporting calls, approval cycles per site | Sub-linear up to a ceiling, then specialist hiring resumes | Flat: one strategy, one approval queue, one data definition |
| Time to ship a service-line page | 4–6 weeks per site | 1–3 weeks centrally, slower with cross-site review | Continuous queue, sized to account |
| Failure mode at scale | Approval drag, inconsistent attribution, content inventory resets | Headcount cap on service-line and geography expansion | Depends on quality of underlying data layer |
The per-location agency retainer model is typically the first to fail. Coordination costs increase linearly with the number of sites, not with output, meaning each additional site adds overhead faster than it generates booked appointments. The in-house model sustains longer but eventually encounters a specialist headcount ceiling, where each new service line or region necessitates another hire. The account-level system, by decoupling production capacity from headcount, offers the only cost curve that flattens at scale.
The structural lesson from hybrid B2B coverage research directly applies here: integrating digital, inside, and field operations outperforms parallel channel management because the gains stem from the system's synergy, not from individual functions 4. For healthcare operators managing more than ten sites, this logic determines whether expanding to twenty more locations becomes easier or more challenging.
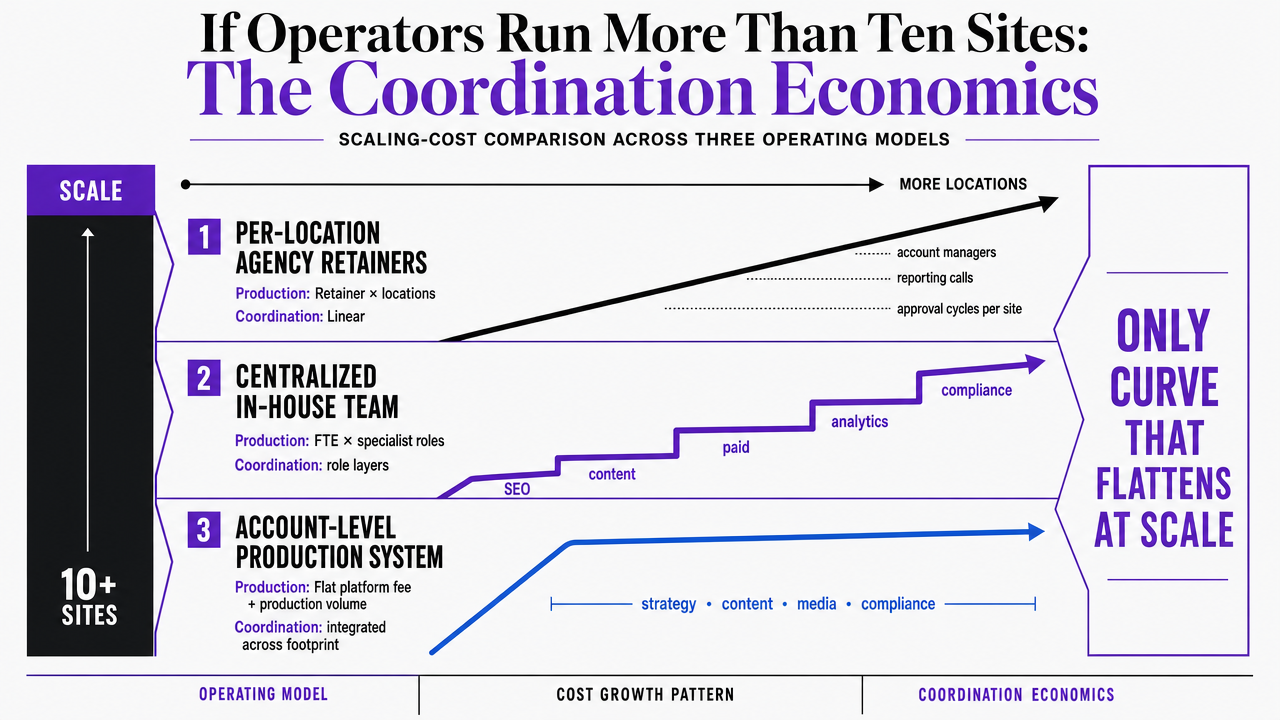 Translate the section's comparison table of three operating models into a visual scaling-cost comparison, reinforcing why account-level production is the only curve that flattens at scale
Translate the section's comparison table of three operating models into a visual scaling-cost comparison, reinforcing why account-level production is the only curve that flattens at scale
What Operators Should Decide Next Quarter
The critical decision for operators is not whether to increase lead generation spending next quarter, but whether that investment will enter a system that compounds value or a collection of accounts that reset periodically.
Three diagnostic checks can differentiate between these two scenarios:
- Can the cost-per-booked-appointment be accurately retrieved by service line across the entire footprint using a single, consistent definition of 'booked'? If not, prioritizing the data layer is essential before increasing media spend.
- What percentage of digitally originated leads result in a confirmed appointment without requiring a phone callback? If this share is below 50%, self-scheduling and its underlying information architecture are the key levers, not creative or bid strategy.
- Does the content library expand each quarter, or does it reset when an agency contract concludes? A library that shrinks between contracts indicates an inventory model that requires constant re-investment.
Operators who honestly assess these three questions will identify which component needs immediate funding. The more challenging decision is structural: whether to continue managing coordination through retainers and increased headcount, or to consolidate strategy, content, media, and compliance review into a single, account-level production program. Vectoron is designed to facilitate this consolidation for operators ready to make that strategic shift.
Frequently Asked Questions
References
- 1.An Overview of Omnichannel Interaction in Health Care Services.
- 2.Barriers to and Facilitators of Automated Patient Self-scheduling for Health Care Organizations: Scoping Review.
- 3.Efficient patient care in the digital age: impact of online appointment scheduling.
- 4.The future of B2B sales is hybrid.
- 5.The impact and challenges of digital marketing in the health care industry.
- 6.Behavioral Analysis of Visitors to a Medical Institution's Website for Improving the Visibility of Medical Information.
- 7.Uses and Disclosures for Marketing.
- 8.Health Products Compliance Guidance.
- 9.FTC's Endorsement Guides: What People Are Asking.
- 10.The future of B2B sales: The big reframe.
- 11.Guidance to Surveyors: Hospital Conditions of Participation.