Key Takeaways
- Patient acquisition is the coordinated visibility of credentials, insurance acceptance, reputation, publicly reported experience, consumer-usable price, and access at the moment a prospect compares providers 1, 4.
- The traditional marketing-funnel framing misrepresents how patients decide, because factors like medical license, certification, and insurance acceptance function as gating filters that outrank reviews and recommendations 4.
- Experience scores under HCAHPS and consumer-usable prices required by 2026 turn previously internal data into public comparison fields a prospect uses before any contact 2, 3.
- For multi-location operators, each input is a data series across sites and service lines, and the weakest instance defines the brand, making account-level coordination a structural requirement.
Why the Old Definition of Patient Acquisition No Longer Holds
Patient acquisition has been defined for years as the marketing process of moving a prospective patient from awareness to a booked appointment. That definition is now too narrow to be operationally useful. The behavior it tries to describe has changed, and the inputs that influence whether a person becomes a patient sit largely outside the traditional marketing function.
Three forces have rewritten the working definition. First, patients increasingly act as informed decision-makers who gather information from literature, the internet, and direct-to-consumer content before contacting a provider 7, 11. Second, the federal government has made experience and price into public, comparable data points through HCAHPS reporting and the 2026 hospital price transparency reforms, which require consumer-usable prices rather than estimates 2, 3. Third, peer-reviewed work on provider choice shows that the factors patients actually weigh, such as medical license, certification, and insurance acceptance, often outrank the channels marketers spend most heavily on 4.
Read together, these shifts move patient acquisition out of campaign vocabulary and into operations vocabulary. It is no longer a sequence of ads and landing pages. It is the coordinated visibility of credentials, insurance fit, pricing, reputation, and access at the moment a person is comparing providers. The sections that follow build a working definition grounded in that research, separate acquisition from adjacent concepts it is often confused with, and translate the definition into what it requires of growth leaders running more than one location.
A Working Definition Grounded in Healthcare Research
Acquisition, Experience, Retention, and Consumerism Are Not Synonyms
Patient acquisition is often used interchangeably with patient experience, retention, and consumerism, which flattens four distinct concepts into one fuzzy marketing term. Each has a specific definition in the research literature, and the differences matter for how growth leaders allocate budget and accountability.
Patient experience : As defined by the Agency for Healthcare Research and Quality, refers to the range of interactions patients have with the health system, including timely appointments, easy access to information, and good communication with clinicians and staff 1. It describes what happens during care, not the decision that led a person to that care.
Healthcare consumerism : Describes the decision posture patients bring into the system. The peer-reviewed literature defines it as patients acting as more active participants in their own healthcare decisions, gathering information from literature, the internet, and direct-to-consumer content before they ever contact a provider 5, 7. Consumerism is a behavior pattern, not an outcome.
Patient acquisition sits between those two ideas. It is the organizational result when consumer-style decision behavior meets a provider's visible experience signals and produces a new patient relationship. The business case literature is explicit on this point: patient experience may influence intermediate business outcomes including the acquisition of new patients, word-of-mouth, and loyalty 9. Retention, by contrast, measures whether that acquired patient returns. Treating these four as synonyms hides the fact that they are governed by different teams, different metrics, and different evidence bases. Separating them is the first step in defining acquisition usefully.
Why 'Funnel' Misrepresents How Patients Actually Decide
The funnel metaphor assumes a roughly linear sequence: awareness, consideration, conversion. Healthcare decision research describes something messier. Patients enter the comparison set already partly informed, often from online health communities and direct-to-consumer content, and they evaluate providers against fixed gating criteria before any marketing message reaches them 7, 11.
Two features of patient decision-making break the funnel model. First, the most important factors in the choice are filters, not persuaders. Peer-reviewed work on provider selection found that medical license, certification, and insurance acceptance ranked among the most important factors patients consider, with reviews and recommendations often weighted lower 4. A provider that fails the insurance filter does not move down a funnel; the prospect exits the comparison entirely.
Second, the inputs that matter are public and comparable. HCAHPS makes hospital experience scores publicly reported and standardized, which means a prospective patient can compare two providers on the same dimensions without ever engaging either organization's marketing 2. That comparison happens in parallel, not in stages.
A more accurate working definition treats patient acquisition as the coordinated visibility of the inputs patients use to filter and rank providers at the moment of comparison. Channels still matter, but they describe distribution, not decision logic. The next section examines which inputs the research identifies as decisive.
What Patients Actually Weigh When They Choose a Provider
Credentials and Insurance Acceptance Outrank Reviews
Marketing budgets often misallocate against what patients actually use to make a decision. The peer-reviewed provider-choice literature is direct on this: when patients were asked which factors mattered most in selecting a provider, medical license, board certification, and insurance acceptance ranked among the most important, while online reviews and recommendations from others were often less important 4. The hierarchy is closer to a gating sequence than a weighted score.
That distinction matters operationally. A provider who fails the insurance filter does not lose a few points on a comparison sheet; the prospect removes that provider from consideration before any review content, content marketing asset, or paid placement enters the evaluation. The same is true for credential visibility. If a patient cannot quickly confirm that a clinician holds the relevant license and certification, the listing functions as incomplete inventory rather than a competitive option.
The implication for growth teams is uncomfortable. Spend that funds review velocity, social proof creative, and brand storytelling assumes a comparison where the provider has already cleared the gating criteria. In many markets, that assumption fails silently. Insurance acceptance is misstated or outdated on directory pages. Credential data is buried below fold or absent on bios. Specialty designations are inconsistent across location pages.
Before optimizing the persuasive layer, the gating layer needs an audit: every location, every clinician, every directory surface where a patient checks insurance fit and credentials. The factors the research identifies as decisive 4should be the first data points a prospect encounters, not the last.
Digital Reputation and Narrative Reviews as a Secondary Filter
Reviews do not vanish from the decision once gating criteria are cleared. They become a secondary filter that helps patients rank the remaining options. Research on narrative online reviews and e-doctor choice found that patients interpret review text as a signal of clinical skill, attentiveness, and communication, and that those perceptions influence which qualified provider they ultimately select 10.
Two features of that finding shape how reputation work should be scoped. First, narrative content carries more decision weight than star averages alone. Patients read for specifics about how a clinician explained a diagnosis, handled a wait, or followed up after a visit 10. A four-star average without recent narrative detail offers less decision value than a 4.2-star page with current, descriptive reviews on the same dimensions.
Second, the same research raises a fairness concern that growth leaders should track. Review content can carry biases that affect which providers benefit from reputation signals and which do not, with downstream implications for access 10. That is not a reason to disengage from reputation management; it is a reason to treat review programs as a data quality discipline rather than a sentiment-farming exercise.
Operationally, reputation work earns its budget when it sits downstream of credential and insurance accuracy. Reviews rank the qualified set. They do not create one.
Experience as Both an Outcome and an Acquisition Input
Patient experience is usually framed as a quality and retention metric. The research record shows it also functions as an acquisition input, which is why it belongs inside any working definition of patient acquisition rather than parked in a separate column.
The Agency for Healthcare Research and Quality defines patient experience as the range of interactions patients have with the health system, including timely appointments, easy access to information, and good communication with clinicians and staff 1. Those same dimensions are measured at the hospital level through HCAHPS, the first national, standardized, publicly reported survey of patients' perspectives of hospital care 2. Public reporting converts experience from an internal quality metric into a comparable data point a prospective patient can use before contacting a provider.
The business case literature closes the loop. A peer-reviewed analysis of patient experience and business outcomes found that experience may affect intermediate business outcomes including the acquisition of new patients, word-of-mouth, and loyalty 9. Experience precedes acquisition through public scores, and follows it through the visit that produces the next round of reviews and recommendations.
That dual role has a practical consequence. Experience improvement work, often owned by clinical operations and quality teams, is also an acquisition lever, and the marketing function depends on its outputs. Growth leaders who treat experience data as someone else's report are working with a partial view of what drives new-patient volume across their footprint.
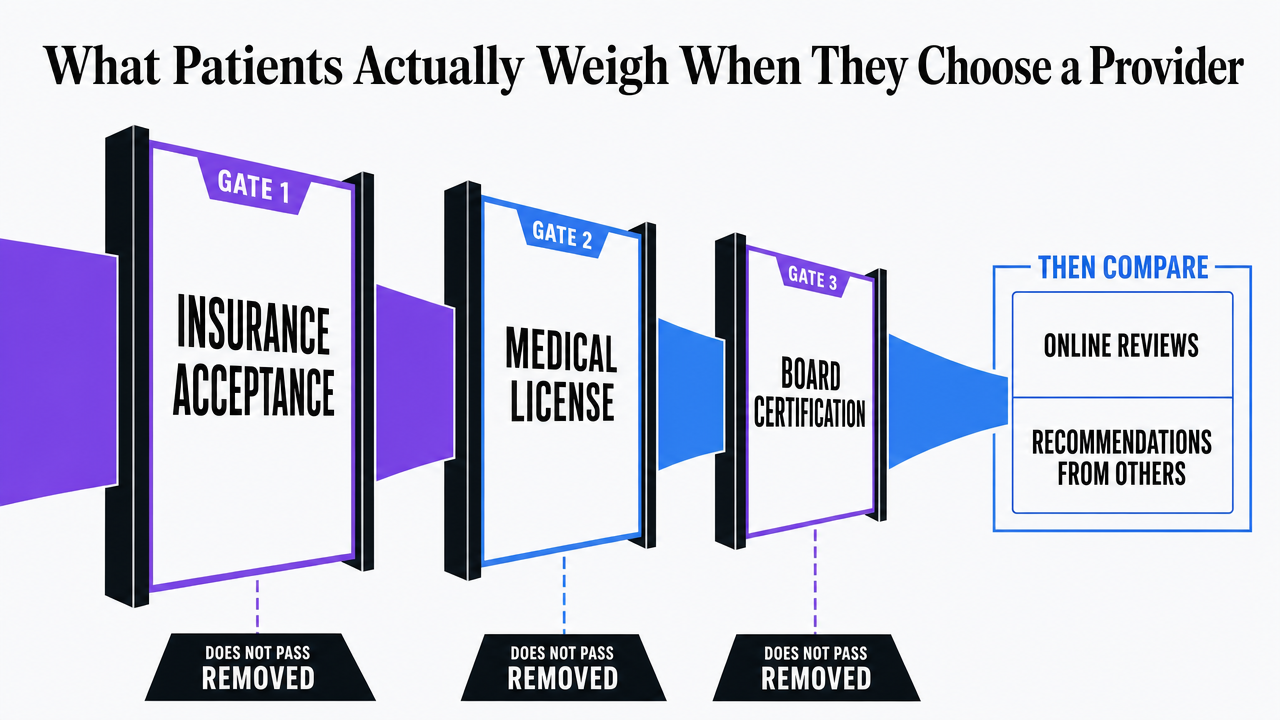 Visualize the gating-then-ranking hierarchy of decision factors patients use, grounded in the provider-choice research cited in this section
Visualize the gating-then-ranking hierarchy of decision factors patients use, grounded in the provider-choice research cited in this section
Experience Account-Level Patient Acquisition Execution Now
Test unified, multi-location patient acquisition workflows and publish live content during your 7-day trial.
The Regulatory Layer: Price Transparency Enters the Decision
Price has been a missing variable in most patient acquisition models because, for years, patients could not get a usable number before service. That gap is closing. CMS has stated that hospitals will need to post real, consumer-usable prices, not estimates, in standardized formats, with the new transparency requirements taking effect in 2026 and enforcement tied to compliance timelines 3. The shift moves price from a post-visit billing question into a pre-decision comparison input.
The acquisition implication is direct. Once standardized prices are published in formats a prospective patient can actually read, price joins credentials, insurance acceptance, and reputation as a filterable field in the comparison set. A patient weighing two in-network options for a planned procedure can compare line-item prices the way they currently compare star ratings. The 2026 effective date gives operators two budget cycles to decide whether their pricing surfaces will read as competitive, average, or off-market when a prospect lands on them 3.
Three operational consequences follow:
- Pricing data has to be accurate at the location and service-line level, not just the system level, because patients compare specific procedures at specific sites.
- The presentation layer matters as much as the data layer, since a compliant machine-readable file does little for acquisition if the consumer-facing display is unreadable.
- Pricing has to be reconciled against insurance acceptance and credential claims already on the site, because contradictions across those fields read as a quality signal to a comparing patient.
Hospital boards are already being pushed in the same direction by consumer expectation. Trustees are urged to monitor what affordability and value mean to the people they serve, which converts price visibility from a compliance task into a strategy question about whether the organization's value story holds up when its prices are exposed next to a competitor's 8. For acquisition leaders, the 2026 date is less a deadline than a publication event: the moment a previously private variable becomes a public one.
Consumerism Without the Cliché: Tension, Not Triumph
Consumerism is the word most often used to explain why patient acquisition has changed, and it is usually deployed as if the shift were settled and positive. The research record is less tidy. The peer-reviewed literature treats consumerism as a real behavior pattern with real frictions, not as a marketing victory lap.
The behavioral side is well-documented. Patients now make healthcare decisions based on knowledge acquired through literature, the internet, and direct-to-consumer content, often before any clinical encounter 7. That posture pressures organizations to compete on transparency, digital access, and visible experience rather than on referral relationships alone 11. For acquisition leaders, that is the part of the story that aligns neatly with budget arguments.
The tension sits in the other half of the literature. A consumerist model gives the patient what they want out of obligation, which can collide with clinical judgment and resource constraints 6. Other work frames consumerism as both a facilitator and a barrier to patient-centered relationships, capable of improving access while introducing market-driven friction that does not always produce better health outcomes 5, 7. There is also an equity concern: consumerist models may disadvantage vulnerable populations whose information access, digital fluency, or insurance status limits their ability to act as comparison shoppers 11.
Acquisition strategy reads more accurately when it holds both sides. Consumer-style behavior is the operating reality. Treating it as an unambiguous good produces marketing that overweights persuasion and underweights the patient-centered substance the same patients are checking for.
See How Top Healthcare Networks Streamline Patient Acquisition at Scale
Request a walkthrough of unified marketing systems that coordinate content, SEO, PPC, and backlinks across all locations—delivering measurable patient growth without fragmented workflows or added headcount.
If You Manage Multiple Locations: Acquisition as a Portfolio Discipline
Why Multi-Location Acquisition Breaks Per-Site Tactics
The working definition built so far applies to any provider, but its operational weight lands differently on operators running more than one location. For hospital systems, specialty groups, DSOs, MSOs, and ambulatory networks, the acquisition inputs identified in the research, credentials, insurance acceptance, reviews, experience scores, and the price fields coming online in 2026, are not single artifacts. They are data series repeated across every site and service line, and each instance is a separate point of failure in the comparison set a prospective patient is building 3, 4.
The per-site model treats each clinic as a standalone marketing project with its own directory listings, its own review program, its own pricing display, and often its own vendor stack. That model produces predictable drift:
- Insurance acceptance updates land at five sites and miss two.
- Credential refreshes appear on the main system page but not on satellite location pages.
- HCAHPS-style experience signals are reported at the system level while a prospective patient is comparing two specific facilities 2.
The patient sees the inconsistency the marketing organization cannot see from inside its own dashboards.
Acquisition at portfolio scale is less a campaign question than a data integrity and coordination question across the same five or six inputs, applied identically at every site.
How Single-Site and Multi-Site Operators Handle the Same Inputs
The inputs do not change between a single-site clinic and a forty-site specialty group. The operating posture toward each input does. The contrast below uses qualitative state descriptions rather than dollar figures, because the research record supports the variables but not the cost math.
| Acquisition input | Single-location operator | Multi-location operator |
|---|---|---|
| Credential visibility 4 | One bio page, manually maintained | Bios replicated across location pages, directories, and specialty pages; consistency depends on a system of record |
| Insurance acceptance display 4 | Single payer list, updated in one place | Payer lists vary by site and service line; per-location vendors often produce contradictions |
| Price transparency readiness 3 | One pricing surface to reconcile against the machine-readable file | Location-level and service-line-level pricing surfaces, each requiring its own consumer-facing display by 2026 |
| Review and narrative reputation 10 | One Google profile, one review feed | Dozens of profiles; narrative quality and recency vary by site, with downstream effects on the qualified set |
| Experience reporting 2, 9 | Internal scores, often informal | HCAHPS or equivalent scores compared publicly across facilities within the same system |
| Access and booking 1 | One scheduling path | Multiple scheduling systems, hours, and intake flows that a prospect compares across sites in the same search |
The pattern across rows is the same. Single-site operators manage one instance of each input. Multi-site operators manage a distribution, and the weakest instance in that distribution often defines how the brand reads to a comparing patient. Account-level planning, applied across every site under one growth program rather than per-location vendor relationships, is the structural answer to a problem the research describes as decision-level, not channel-level.
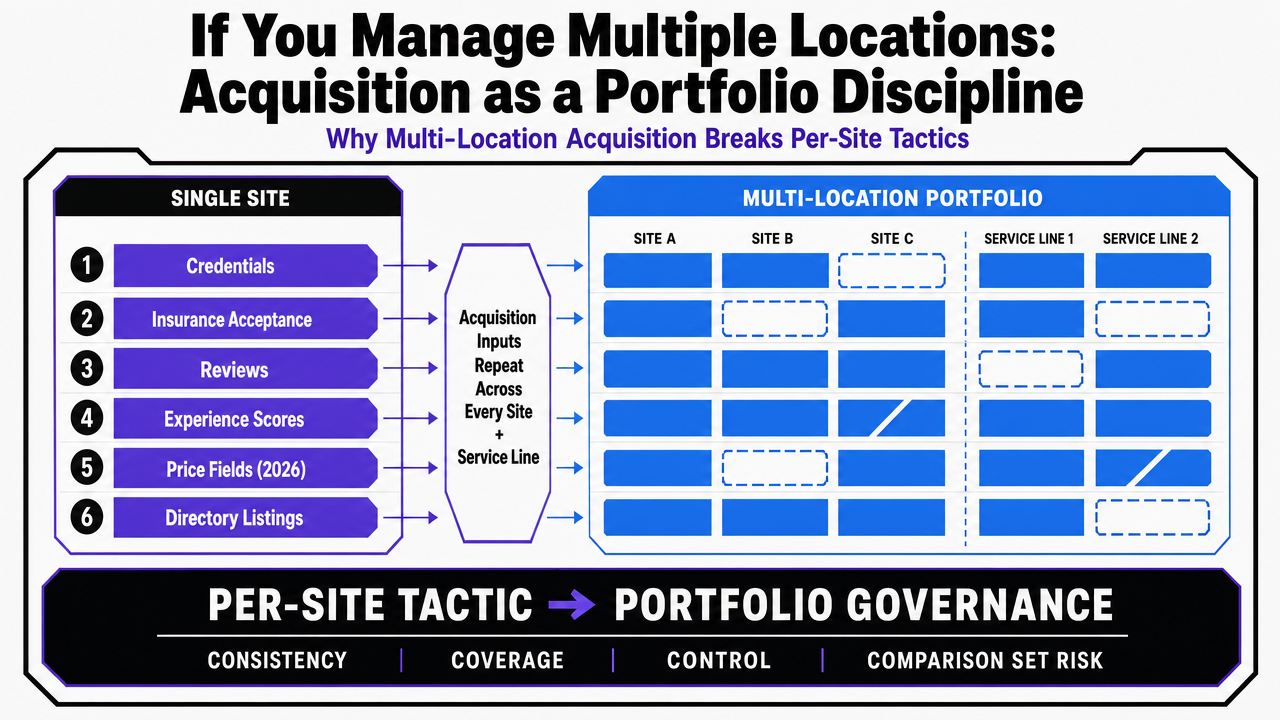 Translate the article's single-site vs multi-site comparison table into a clear visual reference for the six acquisition inputs
Translate the article's single-site vs multi-site comparison table into a clear visual reference for the six acquisition inputs
A Revised Definition for Marketing Leaders
Patient acquisition, defined operationally rather than rhetorically, is the coordinated visibility of the data points patients use to filter and rank providers at the moment of comparison: credential and certification clarity, accurate insurance acceptance, narrative reputation, publicly reported experience, consumer-usable price, and reliable access 1, 2, 3, 4, 10. Channels distribute those inputs. They do not substitute for them.
Three commitments follow from that definition. The gating layer comes first, because a provider that fails an insurance or credential check exits the comparison before any persuasion work has a chance to run 4. Experience is treated as both an outcome and an acquisition input, since HCAHPS-style public reporting turns it into a comparable field a prospect uses before contact 2, 9. And consumer-style decision behavior is met with patient-centered substance rather than marketing volume, because the same literature that documents consumerism also documents its frictions 5, 6.
For operators running more than one location, the definition is also a coordination mandate. Each input is a data series across sites and service lines, and the weakest instance often defines the brand. Platforms such as Vectoron exist to run that coordination at the account level, but the definition stands on its own: acquisition is what the comparison set sees, repeated everywhere a patient looks.
Frequently Asked Questions
References
- 1.What Is Patient Experience? | Agency for Healthcare Research and Quality.
- 2.HCAHPS: Patients' Perspectives of Care Survey.
- 3.CMS Empowers Patients and Boosts Transparency by Modernizing Hospital Payments.
- 4.Choosing a Provider: What Factors Matter Most to Consumers and Patients?.
- 5.Does healthcare consumerism serve as a barrier or facilitator to the patient-centered care relationship?.
- 6.Patient-centredness and consumerism in healthcare - PMC.
- 7.Patient-Centered Care and Healthcare Consumerism in Online Health Communities.
- 8.Focus on Consumerism to Drive Health Care Value.
- 9.Examining the Business Case for Patient Experience.
- 10.The Impact of Narrative Reviews on Patient E-doctor Choice.
- 11.Healthcare consumerism: implications for providers and patients.