
Key Takeaways
- Aesthetic patients decide on a surgeon using before/after galleries, testimonials, and reviews, so a top-ranked page without credible visual outcomes and peer voices loses consultations to lower-ranked competitors 4.
- Reorder the KPI hierarchy around booked consultations, consult-to-procedure rate, and revenue per consult, treating rankings and sessions as diagnostic inputs rather than program success metrics.
- Build procedure pages around candidacy, surgeon authority signals, and filterable before/after evidence, while treating reviews as content production and using selective price ranges to screen out unqualified inquiries.
- Focus next on closing the measurement loop from organic landing page to performed procedure, and on consolidating fragmented vendor stacks across multi-location groups into a single approval queue.
How Aesthetic Patients Actually Choose a Surgeon Online
The organic search problem facing aesthetic practices is not a ranking problem; it is a decision problem. Patients evaluating procedures like rhinoplasty, breast augmentation, or facial rejuvenation arrive at a procedure page already weighing factors that have little to do with search engine results. UNC Surgery researchers found that before-and-after photographs and patient testimonials were among the most influential factors in surgeon selection, often prioritized over practice-level signals typically emphasized by SEO teams 4. This means a page that ranks first but lacks credible visual outcomes and peer voices may lose a consultation to a lower-ranked competitor that provides them.
Surgeon-specific evidence further supports this. A 2026 cross-sectional survey of adult plastic surgery patients reported that online review websites are frequently consulted during surgeon selection and significantly shape perceptions of trustworthiness and bedside manner 2. Reviews act as a proxy for attributes prospective patients cannot verify before a consultation.
Channel behavior also narrows the audience. A 2023 systematic review of aesthetic marketing indicated that 81% of patients visiting a facial plastic surgery clinic were 25 to 34 years old, and 97% of surveyed cosmetic surgery patients found social media accounts helpful in decision-making 11. Search often confirms what a candidate has already discovered elsewhere.
Reframing the KPI Hierarchy: Booked Consults Over Rankings
Most aesthetic SEO programs are still measured by keyword positions and organic sessions, which are leading indicators at best. The ultimate metric for an elective practice is qualified consultation bookings, followed by the consult-to-procedure rate and revenue per booked consult. An SEO program that improves rankings without positively impacting these three metrics is not effectively utilizing its budget.
The reordering of the KPI hierarchy is justified by how patients evaluate a page upon arrival. A literature review on web-based patient decision-making concluded that information quality, system quality, service quality, and social influence collectively determine whether a digital health interaction leads to action 5. Rankings bring the visit; these four factors convert the visit into a phone call.
A robust scorecard for an aesthetic practice should track four layers. Booked consultations from organic search are at the top, segmented by procedure. The consult-to-procedure rate is next, as a high volume of unqualified bookings can inflate the top number while wasting surgeon time. Assisted conversions and form-to-call ratios follow, revealing whether the site is converting traffic or merely receiving it. Rankings, impressions, and sessions are diagnostic inputs at the bottom layer.
This prioritization shift means a procedure page ranking third but booking two consults a week is more valuable than a page ranking first and booking only one. Marketing leads who track rankings without considering booked consults are managing a vanity dashboard, and agencies reporting only on the bottom layer should be questioned about the disconnect.
The Qualified-Consultation SEO Stack
Procedure Pages Built Around Candidacy, Not Keywords
Procedure pages are crucial for aesthetic SEO, yet many are designed inefficiently. A page targeting "rhinoplasty [city]" is often optimized for the query itself rather than the visitor's decision-making process. Visitors are not questioning the existence of rhinoplasty; they are asking if they are a candidate, what recovery entails, if the surgeon has experience with their specific case, and if the outcome justifies the cost.
Candidacy should be the organizing principle. A high-performing rhinoplasty page should clearly state who is an appropriate candidate and who is not—addressing aspects like dorsal hump versus tip refinement, primary versus revision, ethnic considerations, and age/health thresholds. This structure aligns with how aesthetic patients weigh decisions; a literature review on web-based patient choice found that information quality and clarity, not just volume, drive action in digital health interactions 5. A patient who identifies as a candidate within the first scroll is a more qualified lead than one who fills out a generic contact form.
Beyond candidacy, the page should answer questions a qualified prospect asks before booking:
- technique options and the surgeon's selection process,
- recovery timelines with return-to-work specifics,
- anesthesia and facility details, and
- pricing context.
Search engines reward depth on these subtopics because they reflect real query clusters. Patients appreciate this depth as it addresses their concerns before a consultation fee is involved.
Keyword density is a diagnostic tool, not an end goal. A page that ranks without booking consults has solved the wrong problem. Marketing leads should evaluate each procedure page by asking: would a prospective patient reading this from top to bottom know if they should book a consultation, and if they should book it with this practice?
Surgeon Authority Signals That Search Engines and Patients Both Read
Authority signals serve both search engines and patients. Search engines analyze structured credentials, named entities, and consistent biographical data to assess expertise. Patients examine the same information for reasons to trust a significant decision. Signals that satisfy both audiences are concrete and verifiable: board certification by the American Board of Plastic Surgery, hospital privileges, fellowship training, society memberships, peer-reviewed publications, and procedure-specific case volume.
A 2026 cross-sectional survey of plastic surgery patients indicated that online review websites significantly influence perceptions of surgeon trustworthiness and bedside manner 2. Credentials alone are insufficient; they must be presented alongside patient-facing evidence. The surgeon bio page is where these elements converge. A bio detailing fellowship specifics, case counts for particular procedures, and a concise statement of surgical philosophy is more effective than one filled with awards and lifestyle photography.
Authority signals should also appear on procedure pages, not just the bio. A rhinoplasty page that names the surgeon, links to their full credentials, and displays case examples performed by that surgeon (not stock photos) addresses trust concerns directly. Research on online ratings as quality indicators found that physician ratings correlate with credentials, guideline adherence, and outcomes, validating their use as legitimate signals 9.
Practice managers should view the surgeon's name as a primary SEO asset. Branded searches for the surgeon often convert at higher rates than procedure queries, indicating a prospect is already comparing finalists. The site should rank for the surgeon's name with content that consolidates credentials, media mentions, publications, and procedure-specific evidence.
Before/After Galleries and Testimonials as Conversion Infrastructure
Before/after galleries and testimonials are not merely decorative; they are critical decision drivers. The UNC Surgery research on aesthetic surgery patients found them to be among the most influential factors 4. Treating them as conversion infrastructure, rather than simple gallery widgets, changes their optimal design, organization, and placement.
Depth is more important than sheer quantity. A rhinoplasty gallery with twelve cases organized by specific concerns (e.g., dorsal hump, bulbous tip, revision, ethnic rhinoplasty) is more effective than one with sixty unorganized cases. Patients self-select into the subset that matches their anatomy and goals. Filtering by concern, age range, and technique transforms browsing into qualification behavior. Each case should include the surgical plan, time elapsed between photos, and relevant context like concurrent procedures.
Testimonials gain weight when they are specific and verifiable. A generic two-line quote about a "great experience" is less impactful than a patient describing why they chose a particular surgeon, what the consultation clarified, and how recovery met expectations. This addresses specific objections a prospective patient might have. A literature review on web-based patient decision-making identified information quality, system quality, service quality, and social influence as key factors determining whether digital health interactions lead to action 5. Well-executed gallery design can positively impact all four.
Placement should follow function. Before/after evidence belongs above the consultation call-to-action on procedure pages, not hidden in a separate menu. The surgeon bio, candidacy criteria, FAQs, and gallery should be on the same page or one click away, reflecting the patient's journey from curiosity to commitment, rather than a CMS's content organization.
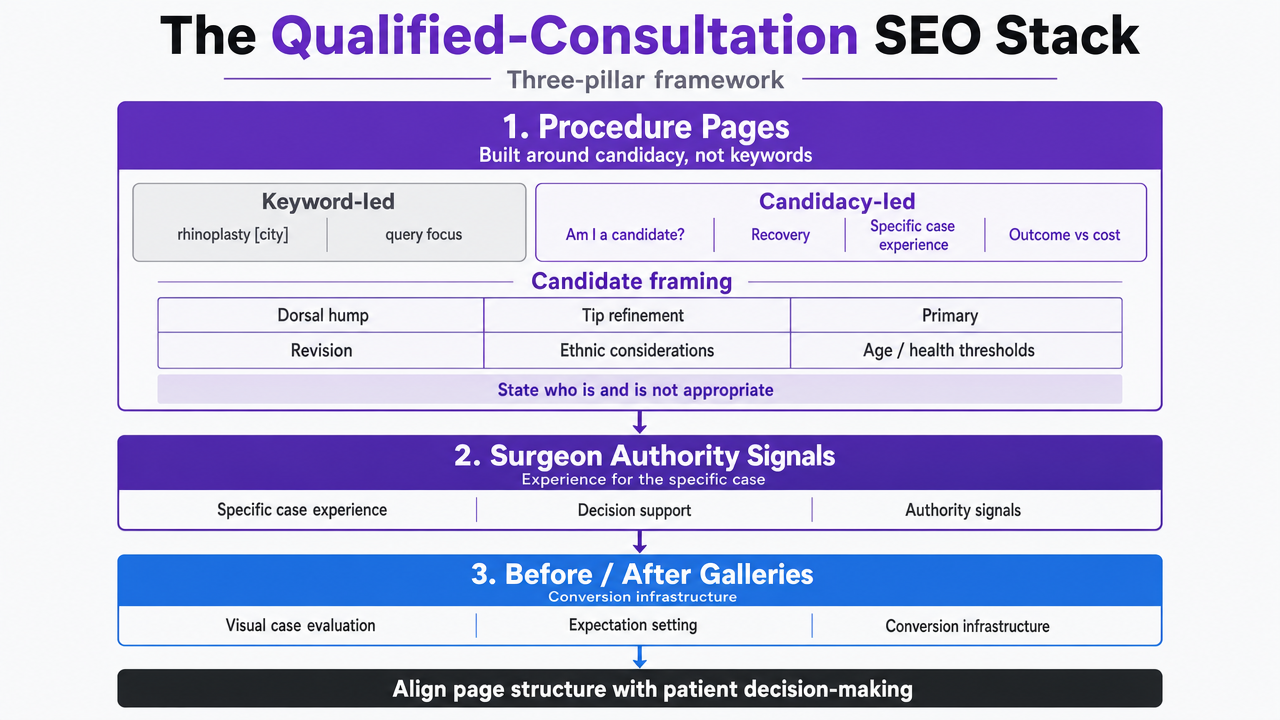 Visualize the three-pillar framework introduced in this section: procedure pages built on candidacy, surgeon authority signals, and before/after galleries as conversion infrastructure
Visualize the three-pillar framework introduced in this section: procedure pages built on candidacy, surgeon authority signals, and before/after galleries as conversion infrastructure
Test SEO content publishing for your practice
Evaluate real-world SEO results by publishing optimized content for your plastic surgery practice during the trial.
Reviews and Response Behavior as Core SEO Inputs
Why Reviews Function as a Quality Signal, Not Vanity
Reviews are often categorized under reputation management, separate from SEO, leading to suboptimal decisions. However, reviews influence local pack rankings, click-through rates from branded queries, and post-click dwell behavior—all signals search engines consider. They also hold independent evidentiary weight in a patient's decision, which ultimately determines if a session becomes a booked consult.
The critique that reviews are merely vanity metrics is disproven by evidence. A Journal of Marketing study, summarized by the American Marketing Association, found that online physician ratings are positively associated with credentials, adherence to clinical guidelines, and patient outcomes, suggesting they are a real proxy for clinical quality 9. Another study comparing online ratings against formal report cards found that positive assessments on physician rating platforms had a significantly positive effect on patient choice, sometimes exceeding the influence of formal quality data 6.
For an aesthetic practice, this means review velocity, distribution across platforms, and the substance of reviewer comments should be treated as content production, not a customer service afterthought. A practice averaging two generic five-star reviews per month will be outperformed by a competitor generating eight reviews monthly that name specific procedures, the surgeon, and the outcome.
Travel Distance and the Economic Value of Reputation
Reputation can expand a practice's effective service radius. A Department of Justice economics paper analyzing Yelp ratings and hospital choice for elective inpatient procedures found that patients were willing to travel 5% to 30% farther for care at a higher-rated hospital 1. While this finding doesn't directly transfer to outpatient rhinoplasty or breast augmentation, the underlying behavior—elective patients prioritizing perceived quality over distance—is the same mechanism aesthetic practices rely on.
The economic impact is clear. A practice with a stronger review profile than competitors within a 15-mile radius can attract qualified prospects from a 25- or 30-mile radius, expanding its addressable market without additional media spend. Conversely, a weaker review profile shrinks this radius, regardless of geographic search rankings.
Practice managers should compare their review profile against direct competitors in their metro area and use the differential for forecasting. If three nearby practices have superior review volume and average ratings, paid and organic spend will yield better returns for them. Closing this gap is essential for SEO investment to compound effectively rather than being diluted by better-reviewed competitors.
Response Language for Negative Reviews
Negative reviews are often misunderstood. The real issue is the absence of a response, or a defensive one. A 2024 experimental study on negative online reviews and physician responses found that both the review's features and the physician's reply significantly shaped causal attributions and willingness to choose the provider 10. Prospective patients infer character from these exchanges, not just clinical competence.
The response template is crucial. Replies that acknowledge the specific concern, avoid relitigating facts publicly, and direct the reviewer to a private channel for resolution are more effective than generic apologies or defensive corrections. Responses should never reference protected health information, even indirectly, nor name the procedure if the reviewer did not.
Response velocity is another key factor. A reply within 48 hours signals an attentive practice, while a six-week delay suggests the opposite to future readers. Practice managers should assign response authority to a specific staff member, with surgeon review for any clinically sensitive replies, and track median response time as a managed KPI.
Screening Out Price-Shoppers Before They Cost Staff Time
Unqualified inquiries are a hidden cost for aesthetic practices. A consult coordinator spending twenty minutes with a caller seeking the cheapest rhinoplasty within fifty miles generates no revenue and displaces a qualified prospect. SEO programs that optimize for raw form fills will exacerbate this issue. The goal is to design the site so unqualified visitors self-select out before entering the booking flow.
Selective pricing transparency is the most direct filter. A Duke Margolis analysis reported that only 17% of healthcare sites publish prices for common procedures, a gap largely due to insurance complexity not applicable to self-pay cosmetic surgery 7. Aesthetic practices can disclose realistic fee ranges by procedure—e.g., primary rhinoplasty within a stated low and high figure based on technique and facility—without committing to a final quote. Visitors unable to afford the lower end of the range will leave, while those who can and continue reading are pre-qualified.
Candidacy framing serves a similar purpose. A procedure page that specifies what the surgeon does not perform—such as non-surgical rhinoplasty for severe deviations or breast augmentation for patients below a certain BMI or age—filters out callers who would consume a consultation slot only to be declined. A literature review on web-based patient decision-making found that clarity and credibility of information influence whether digital interactions lead to action, and clear candidacy criteria contribute to both 8. The inquiry form itself can act as a filter by including fields for budget range, procedure of interest, and timeline, reframing the booking as a mutual evaluation rather than a price quote request.
Content Formats Matched to the 25–34 Aesthetic Buyer
Demographics significantly influence content format selection, often more than aesthetic SEO programs acknowledge. A 2023 systematic review of plastic surgery marketing reported that 81% of patients visiting a facial plastic surgery clinic were 25 to 34 years old, and 97% of surveyed cosmetic surgery patients found social media accounts helpful in decision-making 3. This cohort typically arrives at a procedure page having already consumed short-form video, browsed Instagram, and compared surgeons visually.
Content production should align with this sequence. Short procedure explainer videos embedded on the page—under two minutes, featuring the surgeon, and addressing a specific concern like a deviated septum or tuberous breast correction—are more effective for this audience than long text blocks. The same footage can be adapted for Instagram and TikTok, then linked back to the procedure page, connecting social discovery with search confirmation.
Written content remains important, but the most effective format is the structured FAQ: concise, specific questions answered in three to five sentences each. Topics like recovery timelines, anesthesia choices, scar management, and revision policies are questions search engines often reward with featured snippets, and prospective patients screenshot them for comparison across surgeons.
See How Top Plastic Surgery Practices Achieve Consistent, High-Intent Search Traffic
Request a workflow demo tailored for plastic surgery and discover data-backed frameworks for attracting more qualified consultations—without increasing acquisition costs or wasting resources on unqualified leads.
If You Manage Multiple Locations: Consolidating the Execution Layer
This section is written for marketing leads at aesthetic groups, multi-surgeon partnerships, and DSO-style platforms. Single-location readers can skip ahead.
Multi-location aesthetic groups often face a vendor stack that grows with each new office. This typically includes a content writer or agency, an SEO agency, a review management tool, a call tracking platform, and a web vendor—each billed per location or per seat, producing reports on different cadences that rarely reconcile against booked consults. The execution layer becomes fragmented faster than the brand expands.
The question of consolidation centers on whether a new location adds proportional overhead or if shared infrastructure can absorb it. Procedure pages, surgeon bios, candidacy criteria, and FAQ libraries are largely reusable across locations with surgeon-specific and geographic adjustments. Review response policies, gallery taxonomy, and measurement schemas should be standardized across the group. What cannot be consolidated is local content—neighborhood landing pages, location-specific surgeon bios, and the local review profile that determines each office's catchment radius.
A valid consolidation comparison uses known practice variables rather than invented market averages. The table below uses reader-supplied inputs and an anchor price: a coordinated AI execution platform reference point of $599 per month.
| Cost layer | Per-vendor stack | Consolidated execution layer |
|---|---|---|
| Content production | (L × Rcontent) | Included |
| SEO retainer | (L × Rseo) | Included |
| Review management tool | (L × Rreviews) | Included |
| Call intelligence | (L × Rcalls) | Included |
| Coordination overhead | Internal hours | Single approval queue |
| Reference price | Sum of above | $599/mo post-trial |
L represents the location count, and each R variable is the per-location retainer the group currently pays. A four-location group with four separate retainers at any significant monthly rate will see the per-vendor column scale linearly, while the coordinated layer remains flat. The savings claim is only as accurate as the inputs; practice managers should review twelve months of actual invoices before modeling.
The operational gain often outweighs the line-item savings. A single approval queue for content, SEO, reviews, and call intelligence streamlines the briefing and reconciliation cycles that typically consume marketing-lead time in multi-location groups, which often limits the pace at which a group can open new offices.
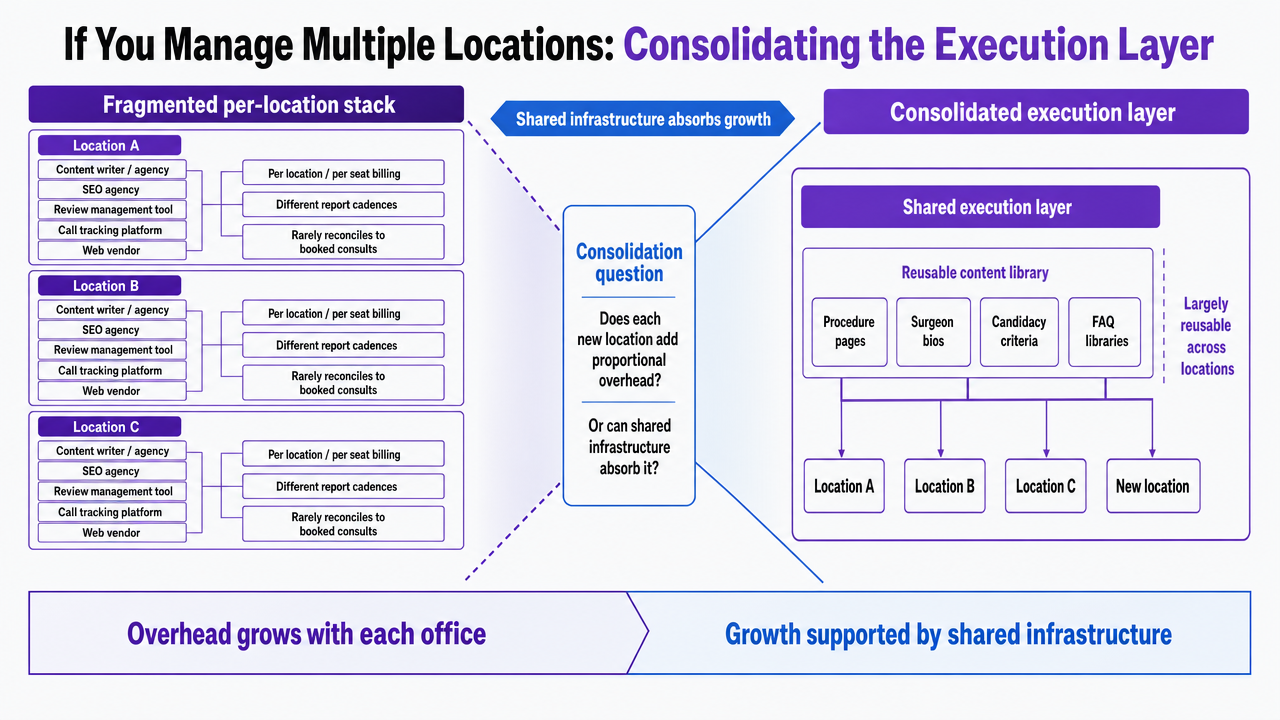 Visualize the comparison between fragmented per-vendor stack and consolidated execution layer described in this section's table
Visualize the comparison between fragmented per-vendor stack and consolidated execution layer described in this section's table
Measurement: Connecting Organic Signals to Consult-to-Procedure Rate
Measurement is where many aesthetic SEO programs falter. Agencies report rankings and sessions, the CRM reports booked consults, and the surgical schedule reports procedures performed. These systems rarely communicate, leading to budget decisions based on incomplete data.
Closing the loop requires a single record that tracks a visitor from the organic landing page to a booked consult and then to a performed procedure. Source tracking on every form submission and call—captured via dynamic number insertion and UTM parameters preserved in the CRM—is the minimum infrastructure. Without it, attribution defaults to last-click, and the procedure pages doing the persuasion work are credited to the last channel the patient touched.
The critical program-level metrics are:
- organic booked consults by procedure,
- consult-to-procedure rate for organic traffic versus paid,
- revenue per organic booked consult, and
- median time from first visit to booked consult.
Research on web-based patient decision-making found that information quality and trust signals influence whether digital interactions lead to action 5, making consult-to-procedure rate the clearest measure of whether the site attracts qualified intent or merely noise. A rising consult volume with a falling procedure conversion rate indicates a content problem, not just a traffic problem. Marketing leads should review the entire chain monthly and disregard ranking reports that do not align with these conversion metrics.
Frequently Asked Questions
References
- 1.Online Reviews and Hospital Choices.
- 2.The Utilization and Influence of Online Review Websites in Plastic Surgery.
- 3.The New Era of Marketing in Plastic Surgery: A Systematic Review Part 1: Esthetic Practices.
- 4.New study identifies most important factors in aesthetic surgery patient decisions.
- 5.Examining Different Factors in Web-Based Patients' Decision Making: A Literature Review and Classification.
- 6.Comparing the Impact of Online Ratings and Report Cards on Patient Choice of Physician.
- 7.Healthcare Consumers Find Little Information Online.
- 8.Themes affecting health-care consumers' choice of a hospital for elective surgery when receiving web-based comparative consumer information.
- 9.How Online Reviews Influence Doctor Selection [Quality Insights].
- 10.Effect of Negative Online Reviews and Physician Responses on Patients’ Choice: An Experimental Study.
- 11.The New Era of Marketing in Plastic Surgery: A Systematic Review Part 1: Esthetic Practices.