
Key Takeaways
- Behavioral health SEO traffic stalls because pages mix intent shapes, leak data through pixels, and use urgency copy that collides with HIPAA, FTC, AMA, and ADA constraints 3, 6.
- Four regulatory regimes dictate on-page decisions: HIPAA governs forms and tracking, FTC governs outcome claims, AMA ethics shapes CTA tone, and WCAG sets the accessibility baseline 1, 4, 6, 7.
- E-E-A-T and patient evaluation criteria align around named clinician reviewers, real review dates, and primary-source citations, replacing generic 'medically reviewed by' badges that signal review theater 12.
- Multi-facility operators benefit most from a coordinated approval-gated loop where clinical, legal, accessibility, and SEO reviewers sign off on the same draft, cutting version drift and audit exposure.
Why Behavioral Health Search Traffic Rarely Converts to Admits
Organic visibility on behavioral health terms is not the constraint most admissions teams think it is. Sessions arrive, forms submit, and the call center still ends the week short of its admit target. The disconnect sits between the query and the intake handoff, where four regulatory regimes and a patient in clinical distress collide with a marketing funnel built for e-commerce logic.
Patients researching treatment do not behave like buyers. A systematic review of online health information seeking found that comprehension and follow-through vary sharply with age, education, and health literacy, meaning the same landing page produces wildly different downstream conversion depending on who lands on it 10. U.S. survey data shows online searching is now embedded in the care decision itself, not a pre-purchase activity that ends when the form posts 11. The inquiry is part of the clinical journey, and the page has to carry weight a product page never does.
Three structural factors keep traffic from converting:
- Content optimized for volume tends to attract informational queries that never had admit intent.
- Tracking and retargeting setups built for non-regulated industries either break under HHS/OCR online tracking guidance or quietly leak protected information through pixels 3.
- Copy written to maximize urgency runs straight into AMA prohibitions against aggressive advertising and inflated expectations 6.
The strategy that follows treats each of those as a design input, not a cleanup task.
The Four Regulatory Regimes That Shape Every On-Page Decision
HIPAA Marketing, Minimum Necessary, and the 2024 Tracking Vacatur
HIPAA defines marketing broadly enough that several artifacts on a typical behavioral health site sit close to the line. HHS treats a communication as marketing when it encourages the recipient to use a product or service, and the Privacy Rule requires written individual authorization before PHI is used for those purposes, with limited exceptions 1. A nurture email that recommends a partner sober living facility, a co-branded landing page with an outside lab, or a follow-up sequence promoting a new outpatient track can each trip that definition once the recipient list is built from intake data.
The minimum necessary standard sits underneath every form decision. Covered entities are expected to use, disclose, and request only the information needed to accomplish the purpose at hand 2. Intake forms that ask for diagnosis details, medication history, or insurance specifics before a clinical conversation has started fail that test, and they create downstream exposure for any analytics, CRM, or ad platform connected to the form.
The tracking question is the live one. HHS/OCR guidance on online tracking states that information collected by cookies, pixels, and analytics tools may constitute PHI when tied to a regulated entity and to past, present, or future health care, which would pull common Meta and Google Ads pixels into HIPAA's scope on a treatment-finder page 3. A federal court vacated part of that guidance on June 20, 2024, narrowing how aggressively OCR can treat unauthenticated page visits as PHI by default, but it did not erase the underlying framework 3.
The practical read for an admissions operation: third-party pixels on pages that disclose a user's interest in a specific condition or level of care still carry real risk, while server-side analytics and tools covered by a business associate agreement carry materially less.
A decision matrix is the cleanest way to hold that tradeoff in view. The chart below maps the common tracking choices, from third-party pixels at the high-risk end to BAA-covered analytics and server-side configurations at the lower-risk end, against the conditions HHS/OCR guidance and the partial vacatur left in place 3. Architecture choices made on that matrix determine which conversion events the admissions team can even measure.
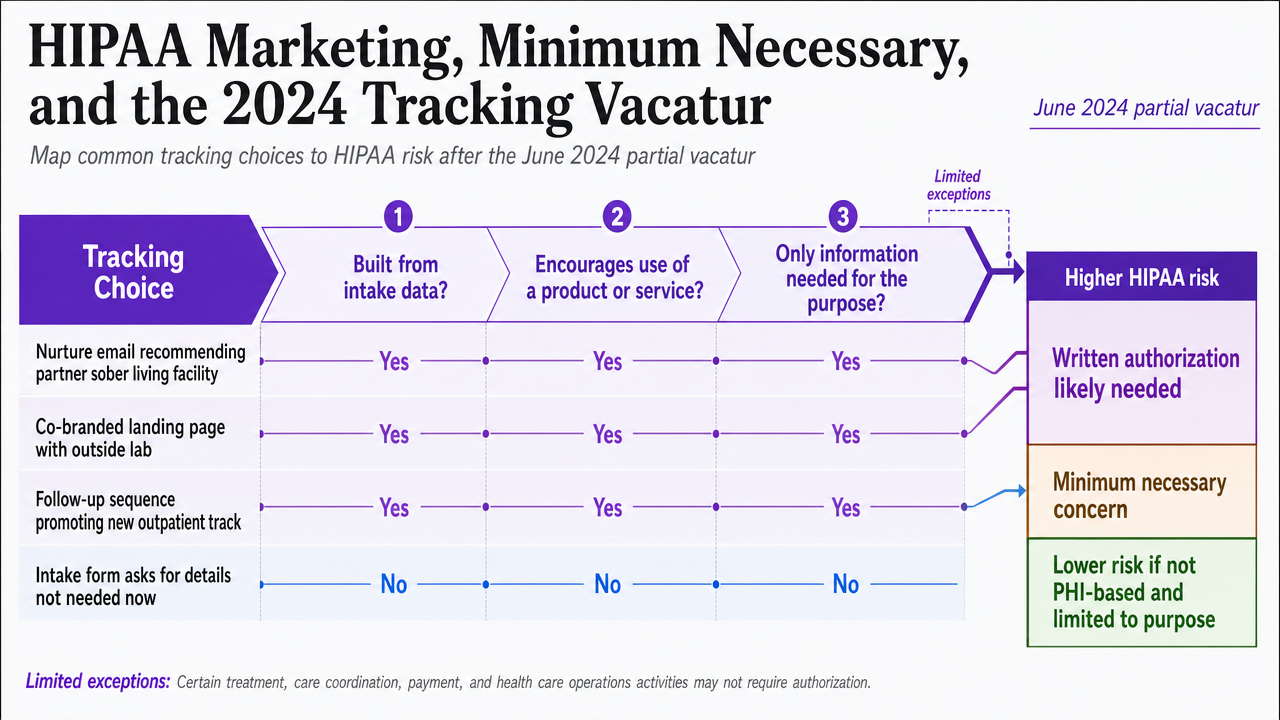 Help readers map common tracking choices against HIPAA risk levels after the June 2024 partial vacatur, directly supporting the section's architectural guidance
Help readers map common tracking choices against HIPAA risk levels after the June 2024 partial vacatur, directly supporting the section's architectural guidance
FTC Substantiation and AMA Ethics on Outcome Language
The FTC requires that health-related claims be truthful, non-misleading, and supported by competent and reliable scientific evidence, and it has applied that standard explicitly to websites, social media, and search advertising 4. The agency's guidance on health claims reinforces that companies must have solid proof for benefit statements, with no carve-out for educational-feeling content that still steers a consumer decision 5. For a behavioral health service page, that pulls every recovery rate, completion percentage, and outcome graphic into the substantiation conversation, including patient testimonials presented as typical experience.
The AMA's ethics opinion on advertising sits adjacent and tightens the screws on tone. Physicians are permitted to advertise, but the opinion warns against aggressive, high-pressure tactics and against communications that create unjustified medical expectations 6. Headlines promising lasting sobriety, CTAs built around manufactured urgency, and hero copy that implies a guaranteed clinical outcome each push against that line, regardless of how compelling they look in a CRO test.
The operational consequence is that outcome language has to be specific, dated, and attributable, or it has to come out. A service page can describe the modalities offered, the credentials of the clinical team, the levels of care available, and any peer-reviewed evidence supporting a particular treatment approach. It should not stack adjectival promises ("life-changing," "proven," "breakthrough") next to a phone number. Testimonials are usable when they are honest, representative, and accompanied by clear context about what was treated and over what timeframe, rather than presented as the default result 4.
Two artifacts deserve a standing review:
- Any statistics block on a treatment page — needs a source, a date, and a population description.
- Any urgency element in a CTA — needs to invite an intake conversation, not pressure a decision.
Both edits usually improve qualified inquiry rates because the visitor self-selects with better information.
ADA Title II, WCAG, and Quality as a Conversion Variable
The DOJ's 2024 ADA Title II rule requires state and local government web content and mobile apps to meet specific accessibility requirements aligned with WCAG, with phased compliance deadlines 7. The final rule's reasoning, set out in the Federal Register, treats inaccessible web content as exclusion from important programs and services, including health and human services 8. Title II does not directly bind private behavioral health providers, but it sets the baseline regulators, plaintiffs, and accreditors now reference when evaluating digital accessibility.
The conversion case for accessibility is separate from the legal case and arguably stronger. JMIR's framework for quality health websites positions accuracy, usability, and accessibility as interlocking dimensions, noting that poor usability undermines the value of accurate content 9. A treatment-finder that fails keyboard navigation, lacks alt text on level-of-care diagrams, or relies on color alone to mark availability loses inquiries from the exact population most likely to need help: visitors with cognitive load, situational impairments, or assistive technology in active use during a crisis search.
The infographic below consolidates the four regimes against the on-page artifacts each one constrains, so the rest of this strategy does not have to relitigate compliance section by section:
- HIPAA marketing and tracking guidance constrains intake forms, pixels, and follow-up communications 1, 3.
- FTC substantiation governs outcome copy, statistics blocks, and testimonials 4.
- ADA Title II and WCAG shape design, navigation, alt text, and media captions 7.
- AMA ethics discipline CTA tone, urgency cues, and headline promises 6.
From here forward, the constraints are inputs to design decisions rather than topics returned to.
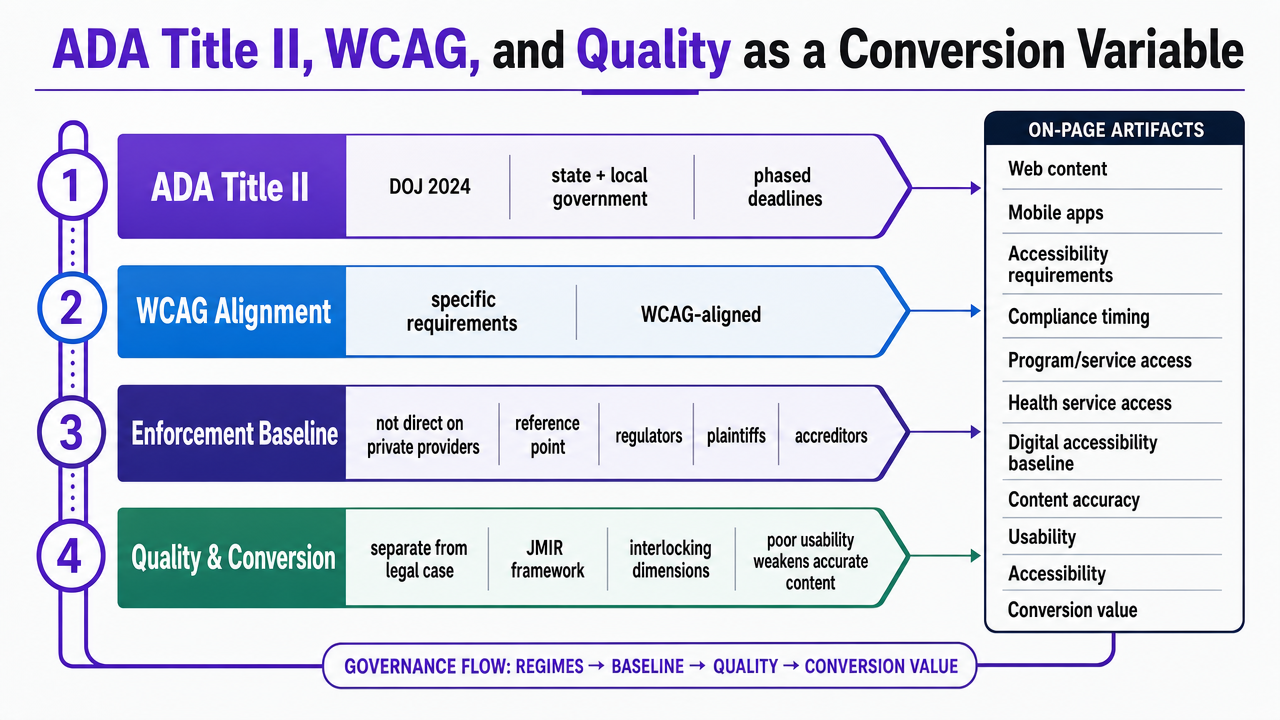 Consolidate the four regulatory regimes against the specific on-page artifacts each one constrains, as the section explicitly references this consolidated view as a governance reference
Consolidate the four regulatory regimes against the specific on-page artifacts each one constrains, as the section explicitly references this consolidated view as a governance reference
E-E-A-T as Patient Evaluation Infrastructure, Not a Ranking Trick
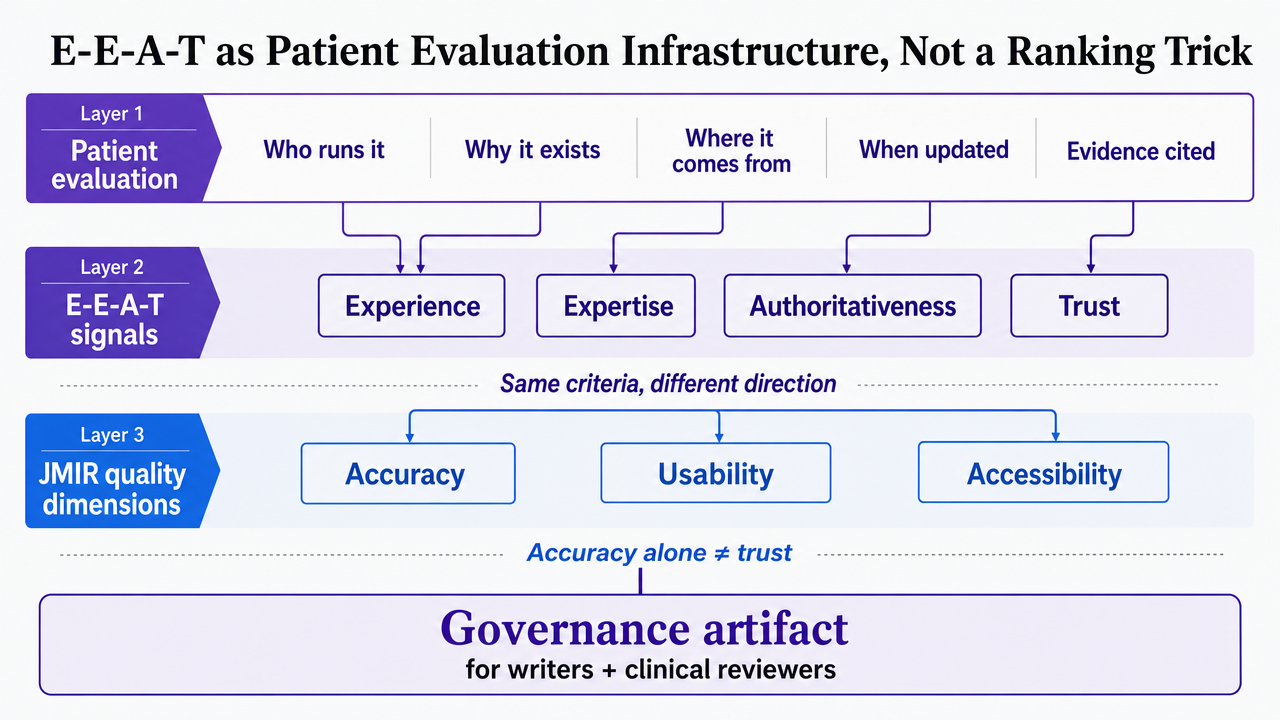
Google's quality signals and the criteria patients actually apply to a treatment page describe the same thing from two directions. MedlinePlus tells consumers evaluating online health information to check who runs the site, why it exists, where the information comes from, when it was updated, and whether the evidence is cited 12. Authority, accuracy, objectivity, and currency are the consumer-facing version of experience, expertise, authoritativeness, and trust. The JMIR quality framework adds the third axis: accuracy without usability and accessibility does not produce trust, it produces a page that visitors abandon before the trust signals load 9.
That alignment is the work, and the infographic below maps it directly so writers and clinical reviewers can use it as a governance artifact rather than a slide. Author bios on a behavioral health service page need a credentialed clinician name, license type, state, and a link to a verifiable profile. Update dates need to be real and recent, not a script-generated timestamp. Citations need to point to primary sources a patient could actually open, which is exactly how MedlinePlus curates its own outbound links: authority, accuracy, ease of understanding 13.
Two artifacts carry disproportionate weight:
- The author block on every clinical page, which should name the reviewing clinician, summarize their relevant experience with the condition or level of care described, and date the last clinical review.
- The references pattern at the bottom of any page making a claim about a treatment modality, which should cite peer-reviewed sources or federal health resources rather than internal blog posts.
Both artifacts double as substantiation evidence if an FTC inquiry ever arrives on outcome language 4.
One pattern worth removing: the generic "medically reviewed by" badge with no name, no date, and no link. It signals review theater rather than review, and it fails both the Google evaluator's read and the patient's. Replacing it with a named clinician, a date, and a link to credentials usually takes a single template change and produces measurable lifts in time-on-page and form completion on pages where the visitor is making a real decision rather than skimming.
 Map Google E-E-A-T signals to MedlinePlus patient evaluation criteria and JMIR quality dimensions, supporting the section's argument that these describe the same thing
Map Google E-E-A-T signals to MedlinePlus patient evaluation criteria and JMIR quality dimensions, supporting the section's argument that these describe the same thing
Test Data-Driven SEO for Medical Websites
Run a live campaign and evaluate real-time SEO results for your medical site during your trial.
Intent, Reading Level, and the Pre-Admission Decision Path
Behavioral health queries cluster into three intent shapes, and most service pages are written for the wrong one:
- Informational queries ("what is medication-assisted treatment," "signs of relapse") arrive from a curious or worried searcher who is not ready to call.
- Comparative queries ("PHP vs IOP," "residential treatment near me") arrive from someone narrowing options.
- Decision queries ("admissions [program name]," "insurance verification for [specific plan]") arrive from a person or family member already pointed at a door.
A page that tries to serve all three usually serves none, and the admit-intent visitor leaves to find one that respects where they are.
Reading level is the other variable being underweighted. The systematic review on online health information seeking found that comprehension and follow-through track closely with education and health literacy, with disparities wide enough to predict whether a visitor acts on what the page says 10. Public Health Reports data on U.S. adults links online searching to greater involvement in care decisions, which means a clearer page is not just easier to read, it changes whether a family member shows up to the intake call prepared to commit 11. A ninth-grade reading level is not a stylistic preference on a treatment page; it is a conversion variable.
The structural fix is to map content to the decision stage and write each stage to the audience actually present. Informational pages can carry depth, citations, and clinical nuance because the reader has time. Comparative pages need a clean side-by-side of levels of care, modalities, typical duration, and what insurance generally covers, with the conditional language FTC substantiation requires 4. Decision pages need three things and almost nothing else: who answers the phone, what happens on the call, and what the next 48 hours look like.
One practical edit pays off quickly. Service pages built for SEO often front-load symptom checklists and educational content above the intake path, which buries the decision-stage visitor under information they did not come for. Moving the intake conversation summary, clinician availability, and verification step into the first viewport, with the educational depth available below or on a linked page, respects the intent split without sacrificing the informational query. The page ranks for the same terms and converts a different visitor.
Instrumenting Qualified Inquiries Without Leaking PHI
Measurement is where most behavioral health programs quietly fail. The marketing team needs to know which keywords, pages, and campaigns produce admits, while HHS/OCR treats data captured by cookies, pixels, and analytics tools as potentially PHI when it is tied to a regulated entity and to a user's past, present, or future health care 3. The June 20, 2024 partial vacatur narrowed how aggressively that framework can be applied to unauthenticated page visits, but it did not remove the underlying exposure for pages that disclose interest in a specific condition or level of care 3. The instrumentation question is not whether to measure, it is where the measurement boundary sits.
A workable stack separates the page-level signal from the patient-level signal. On the page, server-side analytics and BAA-covered tools handle session, scroll, and form-start events without sending identifiers to ad platforms whose contracts do not extend to PHI. At the form, the only fields collected are the ones the intake conversation actually requires, which is the minimum necessary standard applied to a lead capture instead of a chart 2. Diagnosis dropdowns, medication history, and detailed insurance fields belong on a phone call with a clinician, not on a public form indexed by search.
The harder edge is the connection between the inquiry and the admit. Call tracking numbers, intake CRM records, and admit outcomes live inside the covered entity's protected environment. The marketing system gets a non-identifying signal back: campaign source, landing page, and a qualified-inquiry or admit flag with no clinical detail attached. That one-way handoff lets the admissions team see which content produces admits without pushing PHI into ad platforms that would treat the same data as fair game for lookalike modeling.
Two operating disciplines hold the architecture together:
- Business associate agreements with every vendor that touches form, call, or session data, including the analytics platform, the call tracking provider, and the CRM.
- Quarterly audits of every third-party script on treatment, condition, and level-of-care pages, because a marketing tag added for a campaign three months ago is the most common way a compliant stack stops being compliant. Anything that talks to a non-BAA endpoint from a page that signals clinical interest comes off.
See How Enterprise Teams Streamline SEO for Medical Websites With AI Precision
Connect with our experts to learn how digital marketing teams orchestrate multi-channel SEO strategies for medical sites, ensuring compliance, efficiency, and measurable lead quality at scale.
Telehealth and Levels-of-Care Pages as Intake Surface
Telehealth pages carry intake weight that residential and inpatient pages do not. A BMJ Open systematic review of telehealth and patient satisfaction found generally high satisfaction, with variability driven by the technology stack, communication quality, and usability of the appointment flow itself 14. That variability is the SEO point. A telehealth IOP or virtual outpatient page that ranks for the right intent but presents a clunky scheduling path forfeits inquiries the page already earned.
Three elements deserve dedicated real estate on a telehealth or virtual care page:
- Platform and device requirements stated plainly, so a visitor on a mid-range phone in a quiet room knows whether the session will work.
- Clinician availability window, with state licensure noted, since virtual care is bounded by where the clinician is licensed rather than where the patient sits.
- First-session sequence, including what gets discussed, how long it runs, and what insurance verification happens before the call.
Each element addresses a specific source of telehealth dissatisfaction the review identified 14.
Levels-of-care pages need the same intent discipline. PHP, IOP, residential, and detox each attract a different searcher, and a single combined page dilutes the signal for all of them. Separate pages with distinct clinical descriptions, admission criteria, and verification paths rank more cleanly and convert the visitor who arrived ready to act.
Operating Model: A Coordinated Approval-Gated Execution Loop
Where Clinical, Legal, and SEO Review Sit in the Workflow
The bottleneck in regulated SEO production is not writing speed. It is the queue between draft and publish, where clinical accuracy, FTC substantiation, accessibility checks, and HIPAA-aware tracking review each have a legitimate claim on the same page. When those reviews run in series through email threads and shared drives, a single service page can sit in approval limbo for weeks while the keyword opportunity decays.
A coordinated loop puts the four reviews on the same artifact at the same stage:
- SEO production drafts the page against the intent map and keyword brief.
- A licensed clinician reviews the clinical accuracy, the modality descriptions, and the outcome language against the substantiation standard the FTC applies to digital health claims 4.
- Legal or compliance reviews the form fields against the minimum necessary standard and confirms that no third-party script on the page sends identifiers to a non-BAA endpoint 2, 3.
- An accessibility check runs against WCAG criteria the DOJ rule treats as the baseline for inclusive web content 7.
Each reviewer signs off in the same workspace, on the same version, with comments tied to the specific element they touched. Nothing publishes without all four approvals, and every approval carries a name and a date that doubles as the audit trail if an OCR inquiry or FTC letter arrives later. The output is not faster review. It is fewer rounds, because the reviewers are looking at the same draft instead of four different ones.
If You Manage Multiple Facilities: Cost Categories and Two Operating Models
The economics shift once an admissions team is responsible for more than one facility, brand, or level of care. A single-location operator can absorb the coordination overhead of a distributed vendor stack. A multi-facility operator running ten service pages per location across PHP, IOP, residential, detox, and telehealth tracks ends up paying for the same compliance review, accessibility remediation, and analytics rebuild five or ten times over, with version drift between locations that makes audit response expensive.
Five cost categories drive the spread between operating models:
- Clinical content review
- Accessibility remediation against WCAG
- HIPAA-aware analytics configuration and BAA management
- Landing page production at the level-of-care granularity
- Call and intake QA tied back to qualified-inquiry signals
The table below holds those categories against two models without inventing benchmark dollars. Operators fill in their own hours, FTE allocations, and per-page costs.
| Cost category | Distributed agency and vendor stack | Coordinated approval-gated execution |
|---|---|---|
| Clinical content review | Per-page hours × locations × clinician rate; coordination via email | Per-page hours × locations × clinician rate; coordination inside the workflow |
| Accessibility remediation (WCAG) | Per-site audit fee plus per-issue remediation, repeated per vendor handoff 7 | Template-level fixes propagated across locations; audit recurs annually |
| HIPAA-aware analytics and BAA management | Per-vendor BAA review, script audit hours per quarter 3 | One stack, one quarterly audit, one BAA inventory |
| Landing page production | Per-page fee × levels of care × locations | Per-template build, per-location variant hours |
| Call and intake QA | Call tracking vendor fee plus QA FTE allocation | Call tracking inside the same stack; QA tied to attribution flag |
The trial cost reference for a coordinated platform is documented at $599 per month after a two-week trial, which gives multi-facility operators a fixed input against the variable column on the left. Whether the math works depends on how many pages, locations, and review cycles the team actually runs in a year. Vectoron is built for that comparison, with the specialist coordination and approval gating described above as the operating model rather than the marketing claim.
Frequently Asked Questions
References
- 1.Marketing (HIPAA Privacy Rule Guidance).
- 2.Summary of the HIPAA Privacy Rule.
- 3.Use of Online Tracking Technologies by HIPAA Covered Entities and Business Associates.
- 4.Health Products Compliance Guidance.
- 5.Health Claims.
- 6.Advertising & Publicity (AMA Code of Medical Ethics Opinion 9.6.1).
- 7.Fact Sheet: New Rule on the Accessibility of Web Content and Mobile Apps Provided by State and Local Governments.
- 8.Nondiscrimination on the Basis of Disability; Accessibility of Web Information and Services of State and Local Government Entities.
- 9.Making Quality Health Websites a National Public Health Priority: Toward Quality Standards.
- 10.Online Health Information Seeking Behavior: A Systematic Review.
- 11.Online Health Information Seeking Among US Adults: Measuring Progress Toward a Healthy People 2020 Objective.
- 12.Evaluating Health Information.
- 13.Guidelines for Links.
- 14.Telehealth and patient satisfaction: a systematic review and narrative analysis.