
Key Takeaways
- Define the governance scope before issuing an RFP, documenting which FTC, HHS, and DOJ obligations the engagement must satisfy so every later filter ties back to federal exposure 1, 3, 4.
- Shortlist vendors on artifacts rather than pitches, requiring substantiation logs, disclosure templates, tracking configuration maps, and accessibility checkpoints as preconditions that separate qualified providers from marketing language.
- Stress-test multi-location execution by reviewing a finalist's quarterly production schedule and staffing model, since retainer structures that scale headcount linearly with site count break consistency at the portfolio level.
- Audit editorial governance against a live content sample, scoring citation visibility, readability, Spanish-language coverage, and clinical sign-off because ranking does not certify medical accuracy 8, 10, 11.
- Model unit economics at the current footprint, the 12-month plan, and a doubled footprint, since per-location pricing compounds against acquisitive growth while account-level structures flatten marginal cost.
- Lock substantiation logs, BAA coverage, accessibility checkpoints, and clinical reviewer sign-off into the contract as deliverables; vendors who resist contractual commitments are signaling where the engagement will fail.
Why SEO procurement in healthcare is a governance decision
Selecting an SEO partner for a U.S. healthcare operator no longer resembles a marketing purchase. It looks closer to a procurement decision sitting between legal, compliance, IT, and growth. Three federal regimes now intersect on the same web page: the FTC requires competent and reliable scientific evidence behind health claims in any digital advertising, including organic content 1, 14; HHS warns that tracking technologies on condition or appointment pages can transmit protected health information to third parties without proper safeguards 3; and the DOJ's 2024 web accessibility rule signals where private-sector expectations are moving on WCAG conformance for site templates and navigation 4.
A vendor that produces strong content but cannot document substantiation, configure analytics around PHI exposure, or preserve accessibility through template changes is not a low-quality SEO partner. It is an unbudgeted compliance liability spread across every location it touches.
That reframes the buying question. The VP of Marketing is not shopping for keyword research or link building as discrete services. The decision is which operating model will govern content, technical SEO, and measurement across a multi-site footprint consistently enough that legal, clinical, and brand standards hold on the 47th landing page the same way they held on the first. Ranking is downstream of that choice, not separate from it.
The three federal pressures that filter every vendor
FTC substantiation and disclosure for health claims
The FTC treats SEO content as advertising. Page copy, schema, meta descriptions, blog posts, and landing pages all fall inside the same truth-in-advertising regime that governs television spots and paid media 14. That means any organic page describing a treatment outcome, recovery timeline, success rate, or comparative claim must be backed by competent and reliable scientific evidence — a standard the FTC applies with particular rigor to health products and services 1.
Two practical filters fall out of this. First, an SEO vendor needs a documented substantiation workflow: who reviews the clinical claims on a service-line page, what evidence file supports each claim, and how that file is preserved when copy is refreshed for ranking. Most agencies cannot produce this artifact on request. Second, disclosure hygiene on conversion-oriented pages must meet the FTC's clear-and-conspicuous standard, including on mobile viewports where qualifying language often gets buried below the fold 15. Financial qualifiers on elective procedures, individual-results caveats, and sponsorship indicators all sit inside this surface area.
A related risk lives on hybrid pages that mix editorial content with sponsored or paid placements. The FTC's native advertising guidance warns against formats that lead patients to read promotional material as neutral medical recommendation 2. SEO providers proposing content hubs, partner directories, or comparison pages should be asked how they distinguish editorial from paid surface area at the template level.
HHS guidance on online tracking and PHI
HHS guidance on tracking technologies reaches deeper into the SEO stack than most marketing teams expect. The agency has warned that IP addresses, device identifiers, and browsing behavior on pages tied to specific conditions or appointment flows can constitute protected health information, even without a patient's name attached 3. That brings standard analytics pixels, ad retargeting tags, heatmap tools, and conversion trackers into the HIPAA conversation whenever they fire on condition pages or scheduling funnels.
A 2024 court decision partially vacated portions of the guidance, but HHS has continued to signal that covered entities should evaluate tracking configurations carefully and confirm business associate coverage where vendors receive identifiable data 3. The legal posture is unsettled; the operational expectation is not.
For an SEO selection process, this translates into specific vendor questions:
- Which tags does the agency install by default on service-line templates?
- How does it route conversions when the destination page describes a specific diagnosis?
- Does it sign a BAA when its tooling touches user-level data?
Vendors who answer these questions with marketing language rather than a configuration map are transferring legal exposure back to the operator on every page they touch.
The 2024 DOJ ADA web rule and the accessibility trajectory
The DOJ's 2024 Title II final rule sets explicit WCAG-based requirements for the web and mobile content of state and local government entities 4. Private healthcare operators sit outside its direct reach, but the rule marks where federal expectations are heading, and many systems are adopting comparable standards to limit ADA litigation exposure and meet patient access expectations 4.
The selection consequence is concrete. SEO engagements routinely touch the elements that govern accessibility: heading hierarchy, alt text, link labeling, color contrast on call-to-action elements, focus order on forms, and template-level navigation. A redesign or content refresh executed for ranking can quietly degrade WCAG conformance if the vendor lacks accessibility checkpoints in its publishing workflow. Asking how a provider handles alt-text generation for medical imagery, contrast on procedure-page CTAs, and keyboard navigation on appointment forms separates vendors who treat accessibility as a parallel discipline from those who treat it as someone else's problem.
Read together, the FTC substantiation and disclosure standards 1, 14, 15, HHS tracking guidance 3, and the DOJ accessibility trajectory 4 form three filters every SEO deliverable must clear before publish. A vendor that cannot describe how its workflow handles all three is not yet a candidate.
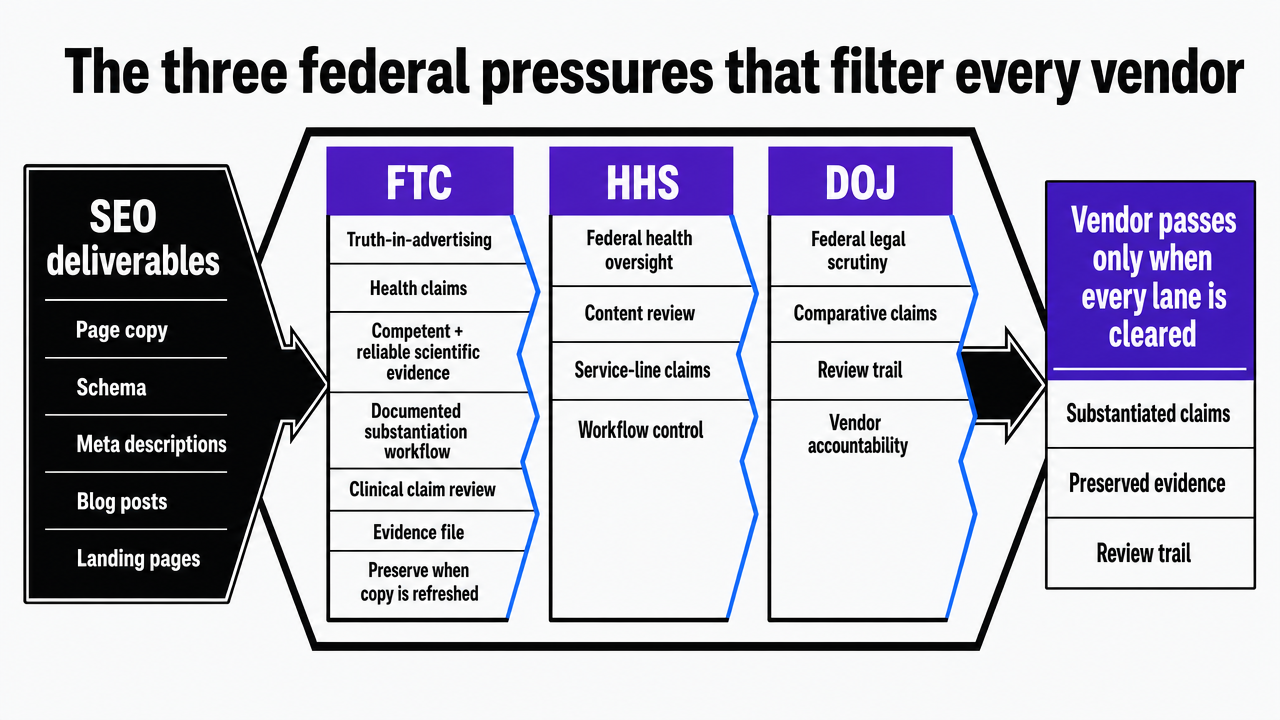 Visualize the three federal compliance regimes (FTC, HHS, DOJ) as parallel filters every SEO deliverable must clear, directly mapping to the section's three subsections
Visualize the three federal compliance regimes (FTC, HHS, DOJ) as parallel filters every SEO deliverable must clear, directly mapping to the section's three subsections
Ranking is not the bar: medical accuracy, readability, and review surfaces
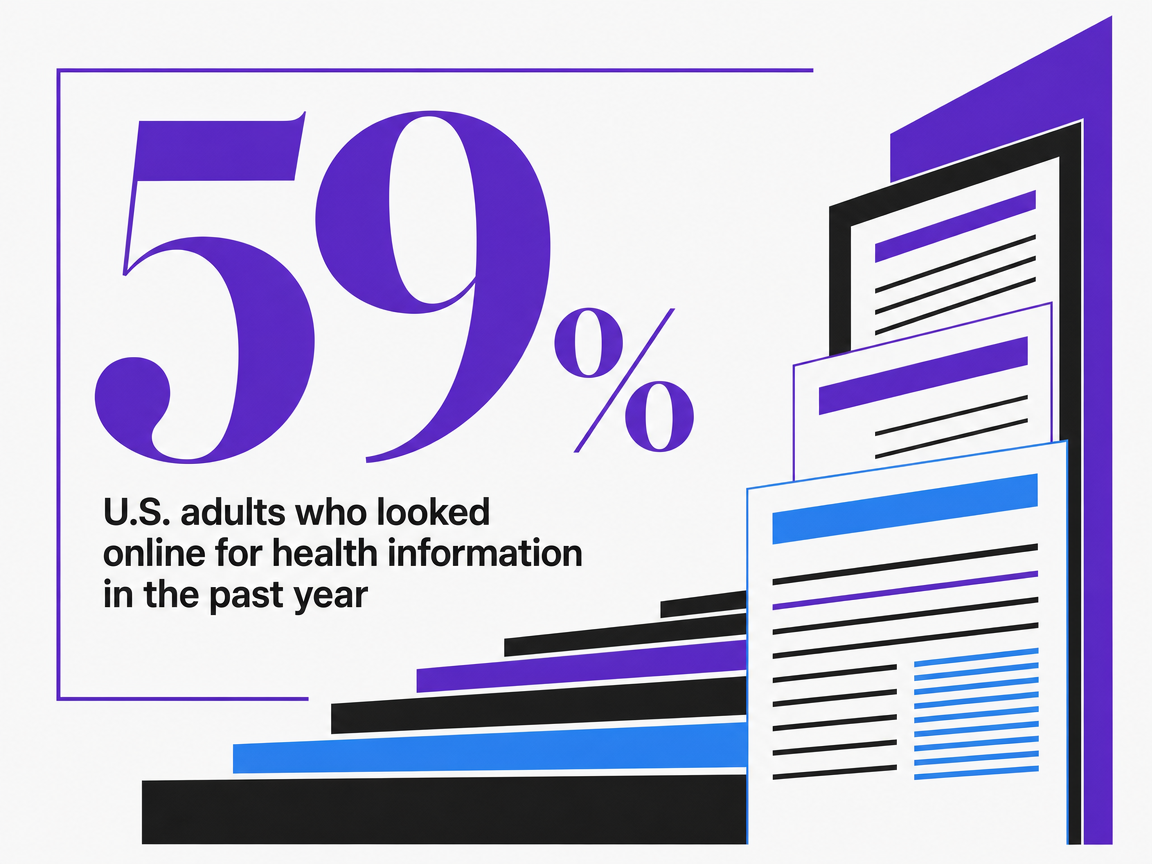
Search engines remain the front door to healthcare decisions. A 2013 Pew Research Center study found that 59% of U.S. adults had looked online for health information in the prior year, and 77% of those online health seekers began their session at a search engine 5. The data is old enough to deserve a qualifier — it predates the mobile-first index, voice search, and generative answer engines — but the directional pattern has held across every subsequent behavioral study of patient research 7, 12. SEO is where patient acquisition starts.
That fact is often misread as a mandate to chase rankings. The evidence does not support that conclusion. A study of search engine results for varicose veins found that top-ranked pages frequently scored poorly on medical quality and exceeded recommended readability levels for patient education 8. A separate evaluation of COVID-19 health information online documented that a substantial portion of highly visible content contained inaccurate or misleading statements 10. A broader literature review on healthcare misinformation reached the same conclusion: ranking does not certify accuracy, and patients struggle to tell them apart 11.
For a multi-location operator, that gap is the selection criterion most agencies will not surface on their own. The right SEO partner has to rank, but it also has to clear a second bar: medically accurate content reviewed against current standards, written at a reading level appropriate for general patient audiences, and available in Spanish where the service footprint requires it 6. Qualitative research on how patients actually evaluate health pages shows they lean on heuristics like design quality and perceived authority because they cannot verify clinical content directly 12. Those heuristics are exactly what review surfaces — Google Business Profiles, third-party directories, physician profile schema — reinforce or undermine 9.
The operational implication is specific. SEO scopes that stop at keyword targeting and on-page optimization leave the accuracy, readability, and reputation layers ungoverned. Vendor evaluation should require:
- A sample content piece reviewed for medical claims substantiation
- A Flesch-Kincaid or comparable readability score on existing client work
- A Spanish-language sample if the footprint demands it
- A documented workflow for review and directory consistency across every location
A provider that can rank a page but cannot show its editorial controls is solving a smaller problem than the one a multi-site operator actually has.
 U.S. adults who looked online for health information in the past year
U.S. adults who looked online for health information in the past year
U.S. adults who looked online for health information in the past year
Test enterprise-level SEO execution before you commit
Experience seamless, multi-location SEO strategy and content publishing with real results during your free trial.
A scoring framework for evaluating SEO providers
Compliance documentation and substantiation workflow
The first scoring axis is whether a provider can produce its compliance artifacts on demand, not whether it can describe them in a pitch deck. Three documents separate qualified vendors from the rest.
The first is a substantiation log. For any service-line page making a claim about outcomes, recovery, success rates, or comparative effectiveness, the vendor should be able to show which clinical sources support each claim and who signed off on the mapping. The FTC applies its competent-and-reliable-scientific-evidence standard with particular rigor to health products and services, and treats organic content as advertising subject to the same rules as paid media 1, 14. A substantiation log is the operational expression of that standard.
The second is a disclosure template library. Pages on elective procedures, financing, or individual-results claims require qualifying language that meets the FTC's clear-and-conspicuous standard across desktop and mobile viewports 15. Vendors should show their default placements, font treatments, and proximity rules, not improvise per page.
The third is a native-versus-editorial policy. Comparison pages, partner directories, and sponsored hubs must distinguish promotional surface area from neutral medical information 2. A provider that scores well here can hand a procurement team binders, not assurances.
Multi-location execution capacity and turnaround cadence
Capacity is the axis where most healthcare SEO engagements quietly fail. A vendor that can rank one flagship site rarely runs the same playbook across 30 location pages, 12 service-line hubs, and a refresh queue without losing consistency.
Three signals reveal real execution capacity:
- A documented per-asset turnaround time for new location pages, service-line updates, and review-driven copy changes — measured in business days, not quarters.
- An account-level content calendar that shows how many simultaneous assets the vendor can move through brief, draft, clinical review, accessibility check, and publish each month.
- A staffing model that does not scale headcount linearly with locations; if adding ten sites means adding ten account managers, the cost curve will break before the second year of the engagement.
VPs running 20-plus sites should ask for a sample production schedule across a recent quarter, including how many pieces were blocked in clinical review and for how long. Bottlenecks are where the multi-location promise dies. Vendors who treat each location as a separate project, rather than a fan-out from a single account plan, will not hold quality at scale.
Evidence governance, citations, and editorial review
The third axis covers what happens inside the content itself. Research on healthcare misinformation shows that inaccurate or misleading material appears in highly visible sources across topics from varicose veins to COVID-19, and that patients lean on design and authority cues rather than verifying clinical content directly 8, 10, 11, 12. SEO content built without editorial governance contributes to that pattern.
A qualified vendor scores well on three controls:
- Citations to primary clinical or regulatory sources appear inside content, not buried in a footer.
- Each service-line and condition page passes through a named clinical reviewer with documented credentials and a sign-off timestamp.
- Readability is measured before publish — a Flesch-Kincaid score appropriate for general patient audiences, with Spanish-language coverage where the service footprint requires it 6.
Procurement teams should request three artifacts: a sample piece with visible citations, a clinical reviewer roster with sign-off records, and readability scores on the vendor's existing client work. A provider that cannot produce these is selling ranking without governance.
Unit economics: account-level vs. per-location billing
The final axis is how the engagement is priced and what that pricing structure does to scaling decisions. Per-location retainers create a cost curve that rises in step with the footprint and a coordination load that rises faster, because every location adds its own approvals, reporting cycle, and account manager touchpoint.
Account-level execution prices the program against the account, not the site count. The same governance workflows — substantiation log, disclosure templates, clinical review, accessibility checkpoints, tracking configuration — run once and fan out to every location and service line. The marginal cost of adding the 31st location is closer to data ingestion than to a new retainer.
Three questions surface the real economics:
- What does the engagement cost when the operator opens five new sites mid-contract?
- How does the vendor's headcount scale to support that growth?
- Which compliance reviews become chokepoints when location count doubles?
Operators scoring this axis should weight pricing structures that decouple program cost from footprint expansion, because the alternative compounds against them with every acquisition.
If you manage five or more sites: operating-model economics
For operators running five or more sites, the SEO selection question stops being about vendor quality and starts being about operating model. The work itself — keyword mapping, content production, technical fixes, link acquisition, review surface management — does not change much across providers at the senior level of the market. What changes is how the work is billed, who governs compliance, and what happens to unit costs when the footprint grows from 12 sites to 30.
Three operating models dominate the buying decision:
- The traditional per-location SEO retainer prices each site as its own engagement, with parallel account teams running parallel workflows.
- A centralized in-house SEO team using point tools consolidates strategy under one roof but absorbs the headcount and tooling cost directly.
- Account-level AI execution platforms price against the account and fan a single governance plan out to every site and service line.
Each model carries different consequences across the four scoring axes already defined.
| Dimension | Per-location retainer | In-house team + point tools | Account-level AI execution |
|---|---|---|---|
| Billing structure | Billed per location; cost scales linearly with footprint | Fixed payroll plus tool stack; semi-fixed | Fixed account-level subscription independent of site count |
| Headcount to scale to N locations | Adds account managers per site cohort | Adds specialists per discipline as load grows | No linear headcount addition tied to site count |
| FTC substantiation workflow 1 | Distributed across vendor teams; consistency varies | Centralized but capacity-bound by reviewer availability | Centralized; same substantiation library applies to every page |
| HHS tracking configuration 3 | Configured per site; drift common across cohorts | Standardized if governance discipline holds | Configured once at the account level; applied to all templates |
| ADA/WCAG handling 4 | Often outside scope or treated per project | Depends on in-house accessibility skill set | Built into template-level publishing checks |
| Compliance review chokepoint | Multiple parallel approval queues | Single queue; capacity-limited | Single queue; capacity scales with automation, not headcount |
| Turnaround cadence as footprint grows | Degrades as coordination load compounds | Stable until reviewer or specialist capacity hits ceiling | Stable; marginal site added is data ingestion, not new engagement |
The retainer model's weakness is not quality on any single site. It is consistency across the portfolio. When the substantiation log for one service line lives in one agency's project folder and the substantiation log for the same service line at a sister location lives in another folder, an FTC inquiry surfaces inconsistencies the operator did not know existed 1, 14. The in-house model fixes the consistency problem and creates a capacity one: a single accessibility reviewer or clinical editor becomes the bottleneck the entire publishing calendar bends around. Account-level execution platforms attempt to break that tradeoff by running governance once and applying it everywhere, with the operator's Command Center holding strategy approval rather than coordinating handoffs.
The economics question for a VP of Marketing is which model's cost curve matches the operator's growth plan. A system holding at 8 locations behaves differently than a DSO platform acquiring two practices a quarter. Per-location retainers compound against acquisitive growth. Account-level models flatten the marginal cost of each new site but require the operator to centralize governance decisions that may currently sit at the practice level.
See Unified SEO Execution for Multi-Location Healthcare and Enterprise Brands
Connect with experts to review how centralized SEO, PPC, and content workflows drive measurable results across all your locations—without traditional agency overhead.
A step-by-step selection sequence for the procurement team
The selection sequence that produces a defensible vendor decision runs through six steps, executed in order. Skipping any of them tends to surface as rework six months into the engagement.
- Step one: define the governance scope before the RFP. The procurement team should document which federal regimes the engagement must satisfy — FTC substantiation and disclosure for any treatment, outcome, or comparative claim 1, 14, 15, HHS tracking guidance on every condition and appointment page 3, and WCAG-aligned accessibility on templates the vendor will touch 4. This scope becomes the filter the rest of the process applies.
- Step two: shortlist on artifacts, not pitches. Request the substantiation log, disclosure template library, native-versus-editorial policy, tracking configuration map, and accessibility checkpoint list as preconditions for shortlisting. Vendors who cannot produce these in two weeks are not shortlist candidates regardless of case study strength.
- Step three: stress-test multi-location execution. Ask each finalist for a sample quarterly production schedule across an existing multi-site client, with clinical review blocks and turnaround times visible. Verify the staffing model does not scale headcount linearly with location count.
- Step four: audit editorial governance against a live sample. Have the vendor produce one service-line page on a topic in the operator's footprint. Score it for citation visibility, readability, Spanish-language coverage where applicable 6, and clinical reviewer sign-off. Research on healthcare misinformation shows ranking does not certify accuracy 8, 10, 11, so the audit must read the content, not the metrics.
- Step five: model the unit economics across the growth plan. Price each finalist's engagement at the current footprint, the 12-month projection, and a double-the-footprint scenario. Per-location structures compound; account-level structures flatten. The procurement decision lives in the slope of that curve.
- Step six: lock the governance artifacts into the contract. Substantiation logs, BAA coverage where tracking touches PHI, accessibility checkpoints, and clinical reviewer sign-off should be contractual deliverables, not best-effort commitments. A vendor that resists making them contractual is signaling where the engagement will fail.
Where AI execution platforms change the buying decision
AI execution platforms belong in the buying decision as a distinct operating model, not as a tool the agency uses behind the scenes. The difference matters. A retainer agency that adopts generative tools internally still bills per location, still routes approvals through account managers, and still concentrates substantiation knowledge in whichever team produced the last asset. A platform built around account-level execution treats the substantiation log, disclosure templates, tracking configuration, accessibility checks, and clinical review queue as shared infrastructure that fans out to every site and service line under one plan 1, 3, 4.
That shift has three practical consequences for a healthcare growth program:
- Editorial governance becomes enforceable at the template level rather than negotiated per project, which reduces the drift the misinformation literature documents in scaled content operations 11.
- Tracking configuration runs once against a documented policy rather than being reassembled on each new landing page, which narrows the HHS exposure surface 3.
- The unit economics decouple from site count, so the marginal cost of adding the next location resembles data ingestion rather than a new engagement.
The procurement question is whether the operator is prepared to centralize governance decisions. Platforms like Vectoron assume that centralization; per-location retainers assume it away.
 Online health seekers who started with a search engine
Online health seekers who started with a search engine
Online health seekers who started with a search engine
Frequently Asked Questions
References
- 1.Health Claims.
- 2.Native Advertising: A Guide for Businesses.
- 3.Use of Online Tracking Technologies by HIPAA Covered Entities and Business Associates.
- 4.Fact Sheet: New Rule on the Accessibility of Web Content and Mobile Apps Provided by State and Local Governments.
- 5.Majority of Adults Look Online for Health Information.
- 6.Health information on the Internet: accessibility, quality, and readability in English and Spanish.
- 7.E-patients: How they use the internet for healthcare.
- 8.Search engine ranking, quality, and readability of web pages about varicose veins.
- 9.Search Engine Optimization and Online Reputation Management for Physicians.
- 10.Evaluating the quality and accuracy of online health information in the era of COVID-19.
- 11.Online information and misinformation on healthcare: a literature review.
- 12.How We Use the Web When We Have Health Problems: Qualitative Study.
- 13.Search engine optimization for public health organizations: A primer.
- 14.Online Advertising and Marketing.
- 15.How to Make Effective Disclosures in Digital Advertising.