
Key Takeaways
- Healthcare SEO past roughly ten locations becomes a coordination problem, requiring an account-level operating model that unifies content, technical SEO, local search, measurement, and compliance rather than stacking per-location retainers.
- E-E-A-T holds up at scale only when each service line has a clinical owner of record, with credentials referenced through structured author profiles and Physician schema that location pages pull from centrally.
- Tracking stacks must be designed against the authenticated-versus-unauthenticated boundary upfront, with BAAs on patient surfaces and de-identified aggregation feeding dashboards per HHS Safe Harbor or Expert Determination 5.
- Build the service-line by location matrix, the clinical author registry, and the HIPAA-aware measurement stack before content, schema, or link work, and extend the scorecard into scheduling and intake completion.
Why Healthcare SEO Breaks at the Location Count
Healthcare SEO scales cleanly up to roughly a handful of sites. Past that, the work stops behaving like marketing and starts behaving like an operations problem. Content briefs queue behind clinical review. Local pages drift out of sync with NAP records. Legal flags a tracking pixel that IT installed six months earlier. The marketing team is no longer running a campaign; it is running a coordination system, and the coordination system is what fails first.
The failure points are predictable. Health content sits inside Google's Your Money or Your Life category, which raises the bar for demonstrated expertise and authority across every service line and every location page. HIPAA constraints on tracking technologies shape what GA4, tag managers, and remarketing pixels can collect on unauthenticated marketing pages versus authenticated patient surfaces 3. FTC disclosure rules apply to organic landing pages the same way they apply to paid ads when testimonials, pricing, or promotional language appear 6. Each constraint is manageable in isolation. Stacked across 40 locations and seven service lines, they compound.
The thesis of this pillar is direct. Multi-location healthcare operators do not need a longer SEO checklist. They need an account-level operating model that treats content, technical SEO, local search, measurement, and compliance as one coordinated system rather than a portfolio of per-location campaigns held together by status meetings.
The Account-Level Operating Model
Per-Location Campaigns vs. Account-Level Coordination
The per-location model treats each site as its own marketing problem. A dental support organization with 60 offices ends up with 60 keyword research deliverables, 60 content calendars, and 60 conversations about why the Tuesday review meeting moved. Each location has its own retainer, its own agency contact, and its own version of the brand voice. The marketing leader becomes the integration layer between vendors who do not talk to each other.
Account-level coordination inverts the unit of work. The keyword universe is built once, at the service-line level, then mapped across the location footprint. Clinical review for an orthodontics page happens once per service line, not 60 times. Technical SEO fixes ship as platform updates rather than per-site tickets. Local signals — Google Business Profile attributes, NAP records, review responses — are governed by one playbook, executed against many endpoints.
The distinction is not cosmetic. It changes who owns what. Under the per-location model, the in-house team owns coordination, which means meetings and chase emails. Under the account-level model, the in-house team owns strategy approval and exception handling, which is the work a VP of Marketing was actually hired to do. The output gap shows up in deadline reliability, brand consistency across location pages, and how fast a new service line can be launched across the footprint.
Consolidation Economics: What VPs Take to the CFO
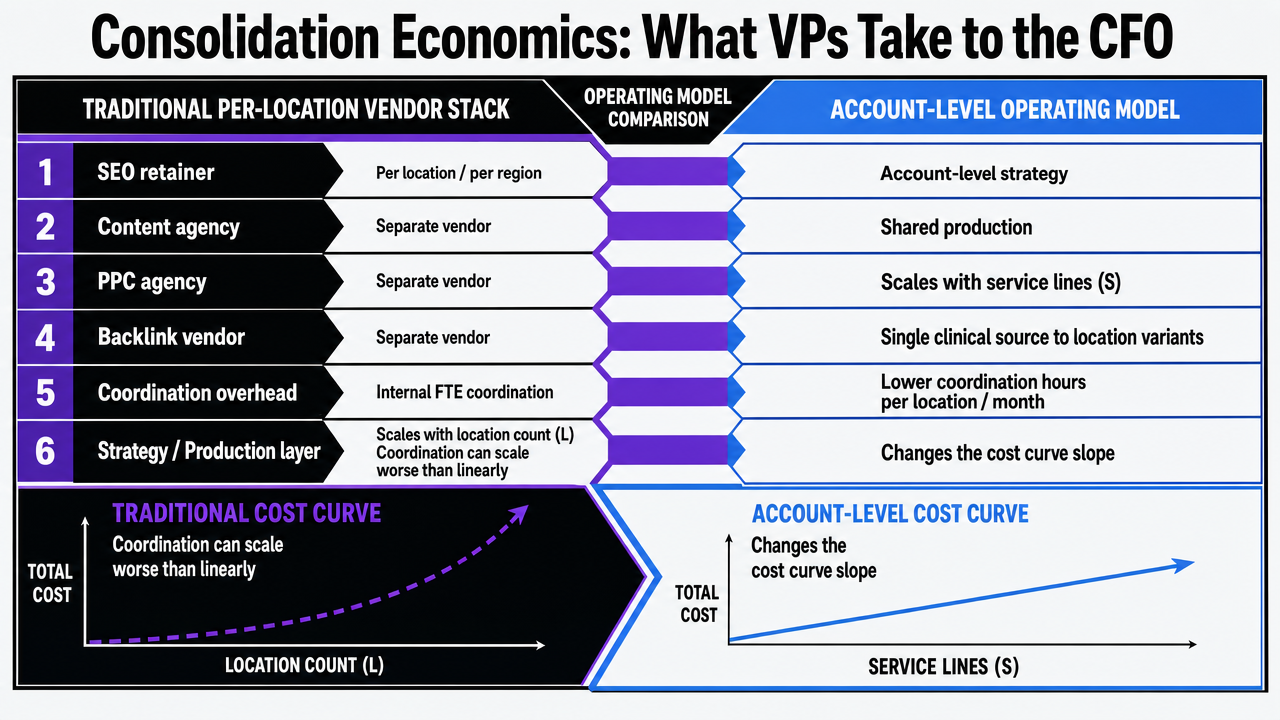
The CFO conversation is rarely about SEO tactics. It is about how marketing cost behaves as the location count grows. Under a traditional stack, a healthcare operator typically funds:
- an SEO retainer per location or per region,
- a separate content agency,
- a separate PPC agency,
- a backlink vendor, and
- internal FTE hours absorbed by coordination.
Each line item scales close to linearly with location count. Coordination overhead often scales worse than linearly, because every new vendor handoff adds an integration point.
Account-level operating models change the slope of that curve. The strategy layer is fixed across the footprint. The production layer scales with service lines (S), not raw location count (L), because most content briefs fan out into location variants from a single clinical source. Coordination hours per location per month drop because the marketing leader is approving work, not assembling it.
The infographic below frames the comparison in variables rather than invented dollar figures, since published benchmarks for healthcare-specific retainer ranges are not standardized across the industry. The variables a VP can fill in from internal data are:
- number of locations (L),
- number of service lines (S),
- monthly coordination hours per location,
- deadline slippage rate (percentage of planned content shipped on schedule), and
- marginal cost per added location.
| Dimension | Per-Location Vendor Stack | Account-Level Model |
|---|---|---|
| Strategy cost | Scales with L (per-site retainers) | Fixed across footprint |
| Content production | Scales with L × S | Scales with S; location variants fan out |
| Coordination hours / location / month | High; multiple vendor contacts | Low; single approval surface |
| Deadline slippage risk | Compounds with vendor count | Contained at one production layer |
| Marginal cost of adding a location | Near-linear | Sub-linear once S is covered |
| New service line launch time | Per-site rollout cycle | One brief, multi-site deployment |
The argument a marketing leader takes upstairs is not that account-level coordination is cheaper line-for-line. It is that the cost curve bends at higher L, deadline reliability becomes a measurable variable rather than a complaint, and adding the 41st location does not require hiring the next coordinator.
 Visualize the comparison table contrasting per-location vendor stacks with the account-level operating model across six cost and coordination dimensions referenced in the section
Visualize the comparison table contrasting per-location vendor stacks with the account-level operating model across six cost and coordination dimensions referenced in the section
YMYL and E-E-A-T as Architecture, Not Editorial Polish
Clinical Author Governance Across Service Lines
Google evaluates health pages against a higher bar because the wrong information can harm a patient. Most multi-location operators try to clear that bar with bylines added after the fact. A staff writer drafts a page on root canals, a clinician's name gets attached, and the page ships. That is editorial polish, not author governance, and it does not survive a quality rater's reading of who actually stands behind the content.
Author governance starts upstream. Each service line is assigned a clinical owner of record — typically a senior practitioner who reviews the source brief once and signs off on the medical claims, dosing ranges, contraindications, and outcome language that will then propagate across every location variant. Their credentials, NPI, board certifications, and practice history live on a structured author profile page that location pages reference, not on a one-off bio block.
The operational rule is one clinical reviewer per service line, not one per page. That keeps review hours manageable at 60 or 200 locations while preserving a defensible chain of expertise. Pages without an assigned clinical owner do not enter the production queue. This is the cleanest way to make E-E-A-T something the org actually maintains, rather than a checklist a writer pastes onto a draft.
Health Literacy as a Ranking Input
Patient-facing pages that read like discharge summaries underperform on both comprehension and search behavior. Bounce rates climb when a reader cannot parse the first 200 words. Dwell time collapses when the call-to-action sits beneath three paragraphs of clinical phrasing the patient was never taught to decode.
The CDC Clear Communication Index gives healthcare marketing teams a scorable standard for fixing this. The Index evaluates main message clarity, call-to-action specificity, plain-language usage, risk presentation, and behavioral recommendations, among other criteria 7. It was built for public health communication, but the scoring logic transfers directly to symptom pages, condition pages, and procedure pages that need to convert search visitors into appointment bookings.
Multi-location operators benefit from running every patient-facing template through an Index review once, at the template level, rather than auditing thousands of location variants. A condition page template that scores well on main message, plain language, and call-to-action clarity carries those properties into every location it populates. That converts health literacy from a soft editorial concern into a measurable input that protects both YMYL ranking signals and conversion rates on the same page.
Structured Data That Reflects Real Clinical Authority
Schema markup on a healthcare site does more than improve rich results. It tells search engines who the practitioner is, where they practice, what credentials they hold, and which conditions or procedures they treat. When that markup contradicts the on-page content — or worse, references a clinician who no longer works at the location — the credibility signal turns negative.
The structured data layer should mirror the author governance model. Physician schema objects live in a central directory, keyed to the clinical owner of record for each service line and to each practitioner's active locations. MedicalCondition, MedicalProcedure, and MedicalWebPage objects on service-line pages reference those physician objects rather than duplicating their attributes inline. NAP fields, hours, and accepted insurance pull from the same source of truth that feeds Google Business Profile.
Maintained this way, structured data stops being a one-time SEO deliverable and becomes a live representation of clinical authority across the footprint. When a practitioner leaves, one record changes, and every page reflects it.
Test Account-Level SEO Execution Workflows Instantly
Experience unified multi-location healthcare SEO strategy and live content publishing on your own sites during the trial.
HIPAA-Aware Measurement: Designing the Analytics Stack Before the Campaign
Authenticated vs. Unauthenticated Pages and the June 2024 Vacatur
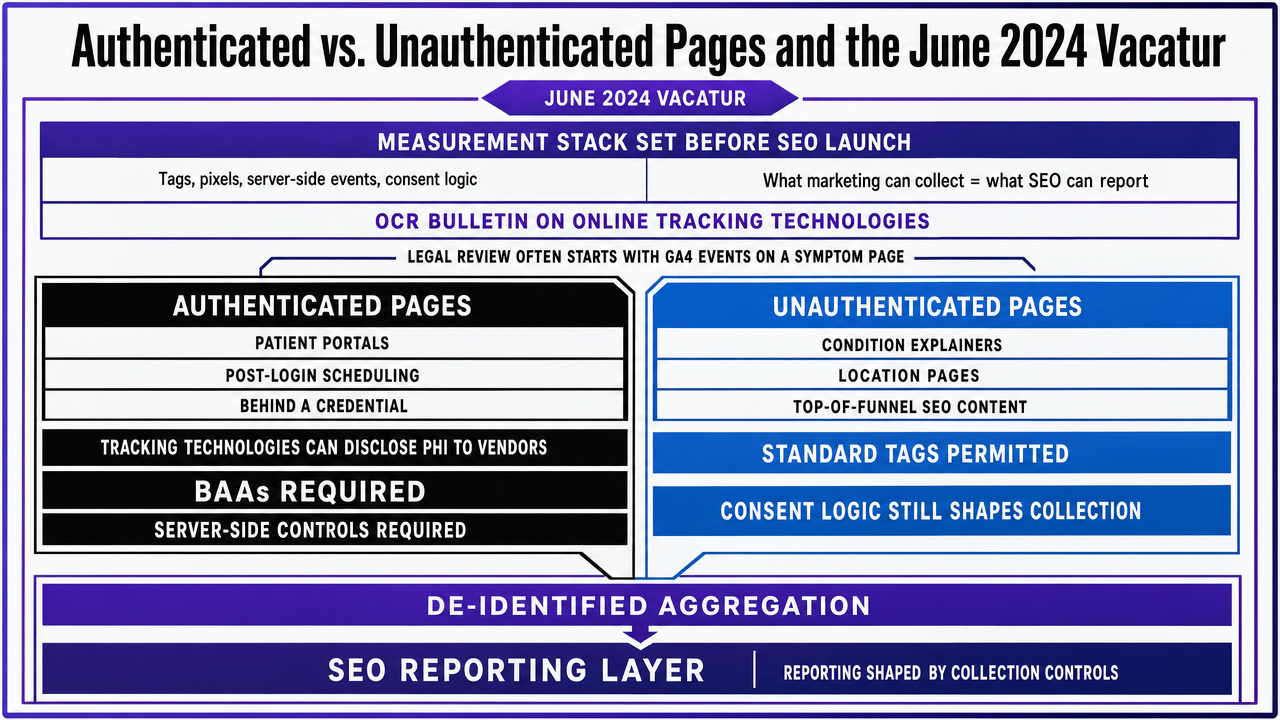
The measurement stack on a healthcare site cannot be retrofitted after the SEO campaign launches. Tag managers, pixels, server-side events, and consent logic shape what data the marketing team can legally collect, which means they shape what an SEO leader can report on. Most healthcare operators discover this after legal reviews a screenshot of GA4 events firing on a symptom page.
OCR's bulletin on online tracking technologies is the governing document. It separates authenticated pages — patient portals, post-login scheduling, anything behind a credential — from unauthenticated public pages such as condition explainers, location pages, and top-of-funnel SEO content 3. On authenticated surfaces, tracking technologies routinely create disclosures of PHI to vendors and require business associate agreements with those vendors, along with full Security Rule safeguards 4. On unauthenticated pages, the analysis is narrower: identifiers combined with health-related URLs can still constitute PHI in specific contexts, but the blanket assumption that any visit to a public health page generates PHI was the part the courts pushed back on.
In June 2024, a federal court vacated the portion of the bulletin that treated combinations of IP addresses and visits to unauthenticated public webpages as PHI in all cases 3. The rest of the guidance stands. The practical consequence for SEO teams: standard analytics on unauthenticated marketing pages sit on firmer ground than they did in 2023, while anything touching authenticated patient surfaces still demands BAAs, server-side controls, and PHI-aware event design.
The infographic below maps the stack: which page types permit standard GA4 and ad pixels, which require BAA-covered vendors and server-side configurations, and how de-identified aggregation per HHS Safe Harbor or Expert Determination 5 feeds the SEO reporting layer without pulling PHI into dashboards. This is the diagram that ends the recurring argument between marketing, legal, and IT.
 Map the HIPAA-aware measurement stack across authenticated versus unauthenticated page types, showing where standard tags are permitted, where BAAs and server-side controls are required, and how de-identified aggregation feeds the SEO reporting layer
Map the HIPAA-aware measurement stack across authenticated versus unauthenticated page types, showing where standard tags are permitted, where BAAs and server-side controls are required, and how de-identified aggregation feeds the SEO reporting layer
De-Identified Reporting and What Counts as PHI in Search Behavior
The reporting layer is where most healthcare SEO programs accidentally create compliance exposure. A dashboard that ties a specific IP address to a sequence of visits across an oncology condition page, a provider profile, and an appointment request form is doing something different from a dashboard that reports aggregate sessions on those URLs. The first looks like a record of an identifiable individual seeking treatment. The second is operational analytics.
HHS recognizes two paths to keep reporting outside PHI:
- Safe Harbor, which requires removal of 18 specified identifiers, and
- Expert Determination, which requires a qualified statistician to certify that re-identification risk is very small 5.
SEO programs should design the reporting layer against one of these standards from the start, not as a retroactive scrub.
The operational pattern that works at scale: raw event data lives in a controlled environment governed by BAAs where required, while the SEO reporting surface — the dashboards a VP of Marketing actually reads — pulls aggregated, de-identified metrics. Session counts by service-line template, conversion rate by location cluster, organic-to-booking yield by condition category. None of those require a single identifiable patient to appear in a marketing report.
FTC Disclosure Rules on Organic Landing Pages
HIPAA is not the only regulator with an interest in healthcare landing pages. The FTC's .com Disclosures guide applies the same consumer-protection standards to organic landing pages that it applies to paid ads when those pages carry testimonials, before-and-after imagery, pricing, financing offers, or efficacy language 6. The staff report behind that guide makes the underlying point explicit: existing prohibitions on unfair or deceptive practices apply fully to advertising and sales made via the internet, regardless of whether traffic arrives through paid or organic channels 10.
For SEO teams, three categories of organic page need disclosure review before they ship:
- Patient testimonial sections require clear language about whether results are typical.
- Pricing or financing modules need the terms, limitations, and any qualifying conditions placed near the offer rather than buried in a footer.
- Outcome or efficacy claims on procedure pages need substantiation that the legal team can produce on request.
Building this into the content template once is cheaper than auditing 200 location variants after a complaint.
Local Search at Footprint Scale
The Service-Line by Location Matrix
Most multi-location operators discover the matrix problem when a regional VP asks why the pediatric dentistry page in Phoenix ranks while the same service in Tucson does not. The answer is almost always that no one ever decided which service lines each location actually offers, in writing, with that decision feeding the page architecture.
The unit of planning at footprint scale is not a page. It is the service-line by location matrix: rows for each service the organization delivers (orthodontics, endodontics, pediatric dentistry, oral surgery), columns for each location, and a populated cell only where that location has a credentialed provider, equipment, and capacity to actually treat the condition. A 60-office DSO with eight service lines has up to 480 cells. In practice, perhaps 220 are real. The other 260 must not generate pages.
This matrix governs everything downstream. URL structures map cleanly to populated cells. Internal linking flows from service-line hubs to qualifying location pages, not to every location. Schema declarations on each location page list only the procedures that location performs, which keeps MedicalProcedure markup honest and prevents the credibility hit when a patient books a service the office cannot deliver.
NAP Integrity, GBP Hygiene, and Review Velocity Across Dozens of Sites
Name, address, and phone consistency is a solved problem at five locations and an unsolved problem at fifty. The failure mode is well documented: a location moves a suite number, the website CMS updates, the Google Business Profile updates two weeks later, the third-party directory aggregators update never, and the location's local pack ranking drops without anyone noticing until a quarterly audit.
The operating rule is one source of truth, propagated outward. Location records live in a master directory keyed to internal location IDs, with NAP, hours, accepted insurance, languages spoken, and assigned clinicians as structured fields. The website, GBP, schema markup, and citation feeds all read from that source. When a suite number changes, one record changes, and the change ships everywhere that record feeds.
Google Business Profile hygiene at scale is the same discipline applied to a different surface. Service categories on each profile must match the populated cells in the service-line matrix. Photos need refresh cadence per location, not per brand. Q&A entries need monitored response, since unanswered patient questions sit on the profile indefinitely.
Review velocity is the variable that compounds. Local pack ranking responds to both review count and recency, which means a location with 400 lifetime reviews and none in the last six months underperforms a location with 80 reviews collected steadily across the same period. The operational target is a review request workflow triggered at the point of service for every completed visit, with response SLAs on every review the location receives, positive or negative. At 60 locations, that is a process specification, not a marketing campaign.
See How Leading Healthcare Networks Achieve Consistent SEO at Scale
Request a walkthrough of unified, AI-driven SEO workflows that synchronize keyword, content, and backlink strategies across every healthcare location—eliminating manual coordination and accelerating measurable growth.
Search Is Now Part of the Downstream Patient Journey
Organic search used to end at the appointment request form. That handoff is now where the conversion math actually gets decided. A patient who arrives from a condition page, sees a scheduling widget that asks for insurance verification through three steps, and bounces to a competitor with one-tap booking has not failed the SEO program — the SEO program failed to account for what the search visitor does next.
McKinsey's 2024 Consumer Retail Health Survey, which polled US healthcare consumers across generational cohorts, reported that 27% of Gen Z respondents had switched doctors, compared with 23% of all respondents 9. The figure is narrow in scope — one consumer survey, one year, US sample — but the directional signal matters for SEO leaders modeling lifetime patient value against acquisition cost. Younger cohorts churn faster, and they judge providers on the digital experience that begins with the search result and continues through scheduling, intake, symptom triage, and virtual visit options.
The American Hospital Association has framed the same dynamic from the provider side. Mobile digital health tools — online scheduling, symptom checkers, virtual care — increasingly determine whether the engagement that started with a search query becomes a booked, retained patient relationship, and inconsistent digital journeys are where multi-location systems lose ground 8. For a VP of Marketing, the operational consequence is that organic conversion rate cannot be optimized in isolation from the scheduling stack, the patient portal, and the intake forms that load on the next click. The SEO scorecard either expands to include downstream completion rates, or it stops correlating with revenue as the patient population shifts.
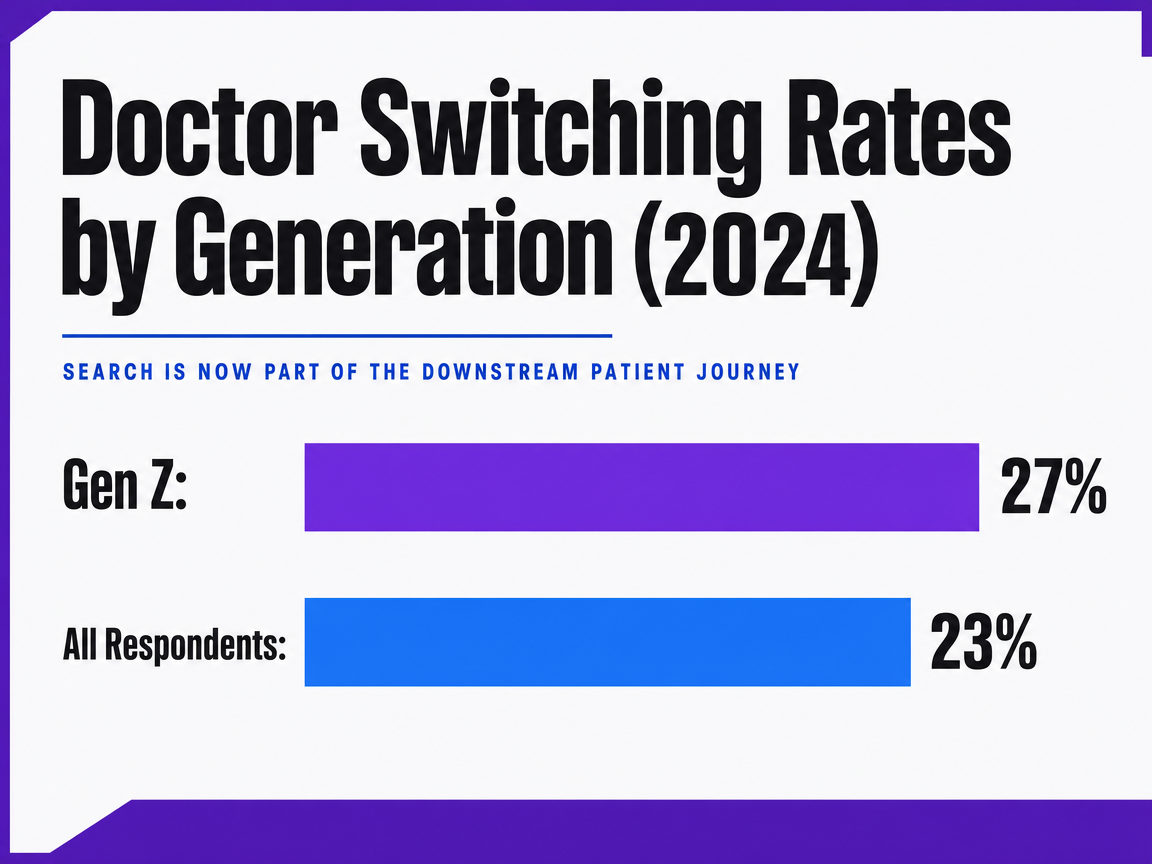 Doctor Switching Rates by Generation (2024)
Doctor Switching Rates by Generation (2024)
A bar chart comparing the percentage of Gen Z respondents who have switched doctors versus the percentage for all respondents from McKinsey's 2024 Consumer Retail Health Survey.
What to Build First, and What to Stop Doing
Sequencing matters more than scope. Healthcare marketing leaders staring at a 60-location footprint and a year of backlogged SEO debt should build three things before anything else:
- the service-line by location matrix,
- the clinical author registry, and
- the HIPAA-aware measurement stack.
Without those, every downstream tactic — content production, schema, local pages, link acquisition — compounds errors rather than fixes them.
The matrix decides which pages exist. The author registry decides who stands behind them. The measurement stack decides what can be reported without exposing PHI 3. Everything else — template-level health literacy review against the CDC Index 7, FTC disclosure patterns on testimonial blocks 6, review velocity workflows — slots into a system that already knows its own constraints.
Three practices to stop:
- Funding separate per-location SEO retainers that duplicate strategy work across the footprint.
- Retrofitting tracking pixels after legal review instead of designing the stack against the authenticated-versus-unauthenticated boundary upfront.
- Treating organic conversion rate as the terminal metric when the scheduling stack and intake flow are where younger patient cohorts actually decide whether to book 8.
Platforms like Vectoron exist to run that coordinated layer; the operating model is the point, regardless of which tool executes it.
Frequently Asked Questions
References
- 1.Marketing | HHS.gov.
- 2.Marketing FAQ | HHS.gov.
- 3.Use of Online Tracking Technologies by HIPAA Covered Entities and Business Associates.
- 4.Use of Online Tracking Technologies (OCR Bulletin PDF).
- 5.Guidance Regarding Methods for De-identification of Protected Health Information in Accordance with the HIPAA Privacy Rule.
- 6..com Disclosures: How to Make Effective Disclosures in Digital Advertising.
- 7.Clear Communication Index User Guide.
- 8.Advancing Digital Patient Engagement — Opportunities for Differentiation.
- 9.Meet Gen Z: Social media and digital tools are key in healthcare.
- 10.Dot Com Disclosures: Staff Report – May 2000.