
Key Takeaways
- Medical marketing is the regulated discipline of communicating about healthcare products and services under four federal regimes: HIPAA for data use, FTC for claim truthfulness, FDA for drug and device promotion, and CMS for Medicare plan communications 1, 2, 3, 4.
- The legal definition is the first input to channel selection, not a final creative filter, because PHI use, claim substantiation, cleared device indications, and CMS review windows each gate what a campaign can say and to whom 1, 12, 13.
- Patient-centered communication is an operational lever on engagement and service quality, with clarity and comprehension driving kept-appointment rates while poor messaging surfaces as cancellations, refunds, and negative sentiment that erode acquisition economics 8, 10, 11.
- Multi-location operators reduce compliance drift by running account-level execution rather than per-location retainers, consolidating substantiation files, HIPAA segmentation policy, FDA claim reconciliation, and CMS review into one approval surface 1, 4, 12, 13.
The Legal Definition That Shapes Every Channel Decision
Most healthcare marketing definitions start with channels. The legal one starts with intent. Under the HIPAA Privacy Rule, the U.S. Department of Health and Human Services defines marketing as a communication about a product or service that encourages the recipient to purchase or use it, and protected health information generally cannot be used for that purpose without written patient authorization 1. That single sentence does more to constrain a healthcare marketing plan than any agency playbook.
The definition is operational, not academic. It separates routine care reminders, treatment communications, and certain plan-administration outreach from anything that crosses into promotion 1. The line determines whether a list segment can be activated, whether a campaign needs documented consent, and whether a vendor needs a business associate agreement before it touches data.
The federal frame extends beyond HIPAA. The Federal Trade Commission governs the truthfulness and substantiation of health claims across channels, including digital, social, and influencer placements 2. The Food and Drug Administration controls how prescription drugs and medical devices may be promoted, including the 2024 final rule on broadcast risk presentation 3. The Centers for Medicare & Medicaid Services regulates communications for Medicare Advantage and Part D plans 4.
Four federal authorities, four different triggers for jurisdiction. A healthcare marketing program that treats compliance as a legal review at the end of production has the sequence inverted. The legal definition is the first input to channel selection, not the last filter on creative.
Four Regulatory Regimes, Not One Compliance Bucket
HIPAA: When a Communication Becomes Marketing
HIPAA does not regulate marketing in the abstract. It regulates the use of protected health information for marketing. The trigger is the data flow, not the channel. A communication encouraging a patient to purchase or use a product or service becomes marketing under the Privacy Rule, and using PHI to deliver that communication generally requires written patient authorization 1.
The carve-outs matter as much as the rule. Treatment communications, case management, care coordination, and certain communications about health-related products or services already provided by the covered entity sit outside the marketing definition 1. A reminder for an annual exam from a patient's existing dental practice is not marketing. A campaign promoting a new aesthetic service line to that same patient list, paid for by a third party, almost certainly is.
For a multi-location operator, the operational consequence is that list segmentation and channel routing must be designed against the legal definition before campaign briefs are written. Email automations, SMS reminders, retargeting audiences built from website pixels, and CRM-driven outreach each touch PHI in different ways. The compliance question is not whether the message looks promotional. It is whether PHI was used to select, segment, or personalize the recipient, and whether the underlying purpose encourages a purchase decision 1.
FTC: Truthful, Substantiated, and Pre-Disseminated
Where HIPAA governs data, the Federal Trade Commission governs claims. The FTC standard for health-related advertising is that messages must be truthful, not misleading, and supported by competent and reliable scientific evidence across every channel, including digital, social, influencer, and native placements 2. The standard does not soften because a claim appears in a TikTok caption or a paid search ad.
The agency's substantiation policy adds a sequencing rule that healthcare marketers frequently miss. Under the reasonable-basis doctrine, a firm must have substantiation in hand before disseminating a claim, not after a complaint forces it to assemble one 13. Pre-claim evidence is not a defensive document. It is a precondition for running the ad.
The scope of enforcement is broad. FTC staff guidance notes that the agency has resolved more than 200 cases involving false or misleading health claims since 1998, spanning supplements, OTC products, devices, and services, and covering both traditional and digital channels 2. That number is a cumulative record across a quarter-century of enforcement, not an annual rate, and it includes a wide range of product categories rather than provider services alone. Read correctly, it signals that the FTC treats health claims as a sustained enforcement priority, not that any single provider category faces a defined risk percentage.
For benefit and outcome claims, the guidance generally points to randomized, controlled human clinical testing as the relevant evidence base 2. Marketing teams that promise clinical outcomes without that backing are operating outside the standard, regardless of how the claim is framed.
FDA: Drug and Device Promotion Is Gated by Pathway
The FDA regulates two distinct promotional surfaces: prescription drug advertising and medical device marketing. Both are gated by the product's regulatory status, which means promotional claims cannot be developed independently of the product's approval or clearance record.
For prescription drugs, the 2024 Clear, Conspicuous, and Neutral final rule changed how broadcast advertising must present risk information. The major statement in television and radio ads must now appear in consumer-friendly language and in a presentation at least as understandable as the rest of the ad, with audio and visual elements designed to reinforce rather than obscure the risk disclosure 3. The underlying rule text amends FDA advertising regulations to require clear, conspicuous, and neutral presentation, removing the design tactics that historically buried risk content under aggressive benefit framing 6.
For medical devices, the gating mechanism is the regulatory pathway. The FDA states that device marketing in the U.S. depends on the applicable pathway: 510(k), De Novo, PMA, HDE, or BLA 12. Each pathway carries different evidence requirements and different permitted claim scopes. A 510(k)-cleared device may be promoted for substantial equivalence to a predicate device's intended use. A PMA-approved device carries a more specific indication. A Humanitarian Device Exemption restricts promotion to the approved humanitarian use. The pathway is not an internal regulatory artifact. It is the ceiling on what marketing can claim.
The operational consequence for a healthcare brand promoting devices or partnering with device manufacturers is that claim libraries, paid search copy, and clinician-facing materials must be reconciled against the clearance or approval document. Promotional language that drifts beyond the cleared indication is not a creative problem. It is a regulatory exposure that can trigger warning letters and forced ad withdrawals, often after the campaign has already produced traffic and pipeline that must be unwound.
CMS: Medicare Advantage and Part D Communications
The Centers for Medicare & Medicaid Services operates the most prescriptive marketing regime of the four. The Medicare Marketing Guidelines set the agency's interpretation of marketing requirements for Medicare Advantage and Medicare Part D communications, covering everything from agent scripts to plan comparison language to call-recording obligations 4.
CMS also publishes standardized model documents and educational materials that plans and downstream entities are expected to use or align to, which compresses creative discretion in this segment far below what other healthcare verticals experience 5. Annual Notice of Change letters, Summary of Benefits materials, and enrollment communications follow templated structures that limit how plans differentiate on message.
For provider organizations that contract with Medicare Advantage plans or co-market services to dual-eligible populations, the practical implication is that any co-branded outreach inherits the plan's CMS obligations. A specialty group running a campaign to attract Medicare-eligible patients to a partnered MA network is not simply running a provider campaign. The content, the call scripts, and the digital landing pages fall inside the CMS marketing perimeter, which includes pre-submission review timelines for many materials 4. Production calendars built without that review window are production calendars that miss the open enrollment window.
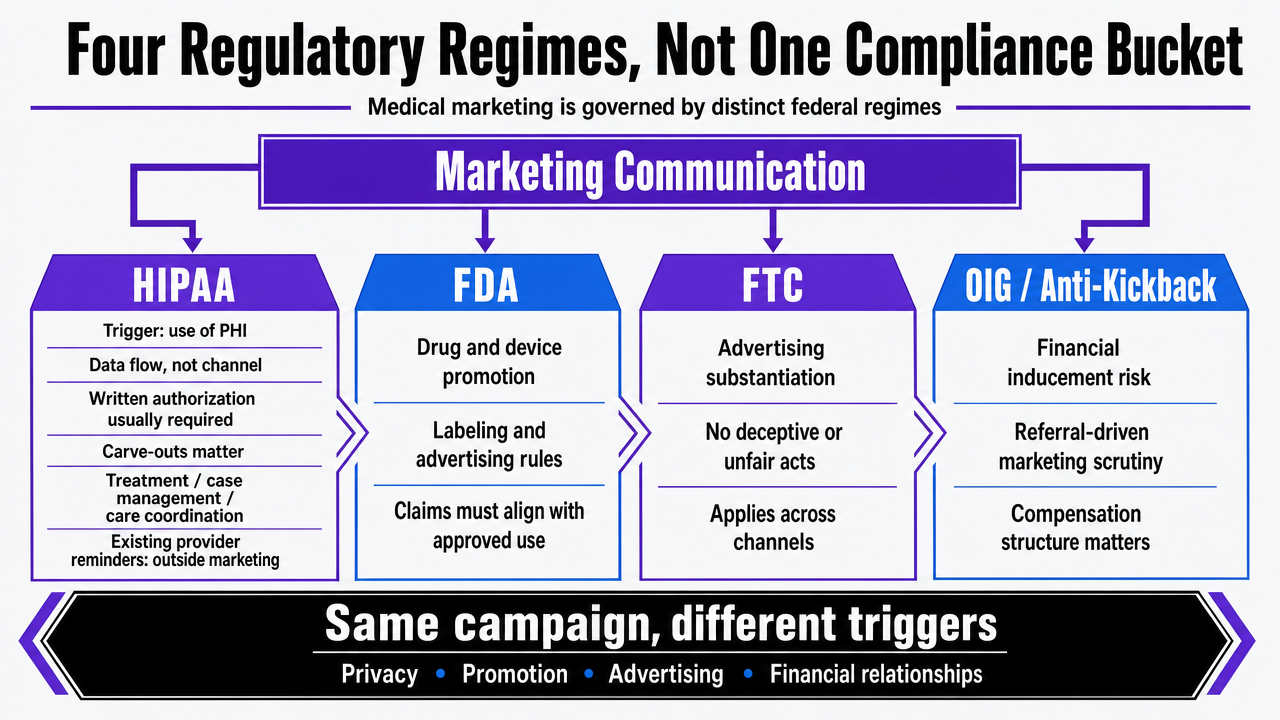 Visualize the four federal regulatory regimes governing medical marketing, which is the central framework explained across the section's four subsections
Visualize the four federal regulatory regimes governing medical marketing, which is the central framework explained across the section's four subsections
The Evidence Base: Why Patient-Centered Communication Outperforms Persuasion
Healthcare marketing borrows more usefully from clinical communication science than from consumer advertising. The evidence base is older than most digital marketing playbooks and points consistently in one direction: clarity, accuracy, and responsiveness to patient preferences produce the engagement metrics that paid persuasion struggles to sustain.
The best-practice review of patient-centered communication identifies six core functions of the discipline:
- fostering the clinician-patient relationship,
- exchanging information,
- responding to emotions,
- managing uncertainty,
- making decisions, and
- enabling patient self-management.
The review reports positive associations between these functions and patient recall of information, understanding of clinical content, and adherence to recommended care 8. Each of those outcomes maps directly to a marketing metric a healthcare VP already tracks: content comprehension scores, time-to-decision in funnel data, and downstream completion rates for booked appointments.
A separate study reports that patient-centered communication positively affected patient engagement, health-related quality of life, and service quality 10. Engagement and service quality are not soft outcomes in this context. They are the upstream conditions that determine whether a campaign converts a click into a kept appointment and whether that appointment generates the referral and review activity that feeds organic acquisition.
The decision-making function deserves separate weight. The NCBI chapter on patient-centered communication defines patient-centered care as care that is respectful of and responsive to individual patient preferences, needs, and values 9. Marketing that helps a prospective patient understand options, including when a service may not be appropriate, performs against a different standard than marketing that pushes a single service. The first is consistent with shared decision making. The second tends to produce the mismatch between expectation and experience that drives negative reviews and refund requests after the conversion event.
The practical implication is that creative review for medical marketing should run two tests, not one. The first is the regulatory test: does the claim meet HIPAA, FTC, FDA, and CMS requirements where they apply. The second is the comprehension test: would a patient at the targeted reading level leave the page understanding what the service is, what it costs, what evidence supports it, and what alternatives exist. Programs that pass the first test and fail the second tend to produce high cost-per-acquisition and low lifetime value, because the patients they convert are the ones least equipped to evaluate fit. The evidence base is consistent on this point: communication quality is an operational lever on engagement and service quality, not a brand-voice preference 8, 10.
Experience Unified Medical Marketing Execution Instantly
Test centralized campaign management and publish live content across your healthcare locations for seven days at no cost.
Marketing as Service Design, Not Promotion
The peer-reviewed review of marketing strategies in healthcare systems reframes the discipline in a way most agency decks do not. Healthcare marketing is more than advertising. It is service design, patient-needs analysis, and communication architecture, with promotion as a downstream output rather than the central activity 7. The framing has direct consequences for how a VP of Marketing allocates budget across the funnel.
Service design treats the patient journey as the product. Appointment booking flow, intake form length, pre-visit instructions, post-visit follow-up, and the readability of insurance and pricing pages all sit inside the marketing surface, because each one shapes whether a prospective patient completes the action a campaign was built to drive. The review specifically notes that healthcare marketing must balance patient-oriented value with institutional goals, which means the metric that matters is whether the service delivered matches the expectation the message created 7.
The reallocation implication is concrete. Spend that improves comprehension on a service-line landing page, reduces friction in a booking flow, or clarifies a pricing disclosure tends to compound across every paid and organic channel feeding that page. Spend that adds persuasion volume to a poorly designed conversion surface tends to inflate cost-per-acquisition without lifting kept-appointment rates. The first is service design. The second is promotion charged against a leaking funnel.
What Communication Failure Costs
The downside case is documented. A narrative review of healthcare communication links poor communication to discontinuity of care, patient safety issues, and dissatisfaction 11. Each of those outcomes sits on the marketing side of the ledger as well as the clinical side. Discontinuity shows up as no-shows and cancellations after the conversion event. Safety concerns surface in negative reviews and complaint volume. Dissatisfaction drives refund requests, chargebacks, and the kind of online sentiment that erodes paid and organic acquisition over the following quarters.
Messaging that confuses pricing, omits material risk, or overstates outcomes does not fail at the click. It fails at the appointment, the procedure, or the billing statement, and the cost lands in retention metrics rather than campaign reports. A campaign can hit its cost-per-lead target and still lose money once communication-driven attrition is counted.
The operational takeaway is to instrument the post-conversion surface. Track kept-appointment rates, post-visit review sentiment, and refund or dispute volume against the campaign and landing page that produced each patient. Communication failures are measurable upstream of the clinical record, and the data needed to catch them already lives in the marketing stack.
See How Leading Healthcare Marketers Standardize Medical Marketing Across Every Location
Get a detailed walkthrough of unified medical marketing execution—content, SEO, PPC, and backlinks—managed from a single platform for multi-site operations. Learn how enterprise brands and agencies streamline campaigns at scale.
If You Manage Multiple Locations: Operator Economics of Account-Level Execution
Why Per-Location Agency Models Create Compliance Drift
This section narrows to multi-location healthcare operators: DSOs, MSOs, hospital networks, specialty groups, and national service-line brands running marketing across more than one site. The compliance picture changes once the operating unit is a portfolio rather than a single practice.
The per-location agency model is the default in most healthcare verticals. Each site retains its own agency or in-house marketer, each agency runs its own creative calendar, and each calendar produces its own approval chain. The structure was built when marketing meant local print, local radio, and local search. It does not hold up against the four federal regimes that now govern the work.
The HIPAA marketing definition does not care which agency produced the email 1. The FTC substantiation standard does not soften because a paid social ad was localized by a contractor 13. When ten locations run ten parallel approval chains, the substantiation file for a benefit claim sits in ten different inboxes, the consent posture for PHI-driven segmentation varies by site, and a CMS-regulated co-marketing campaign at one location may inherit obligations the other nine ignore 4. Drift is the predictable output of fragmented approval, not a failure of any individual reviewer.
The cost surfaces as warning letters, forced ad withdrawals, and consent re-papering exercises that pause campaigns mid-flight. The retainer math hides it. The compliance ledger does not.
Account-Level Execution as a Compliance Posture
Account-level execution treats the portfolio as the unit of work. One strategy plan covers every site and service line. One claim library serves every paid and organic channel. One approval workflow routes every regulated asset through the same review. The model is a compliance posture before it is a cost structure.
The substantiation file for a benefit claim is built once and applied everywhere the claim runs, which matches the FTC reasonable-basis standard that requires pre-dissemination evidence in hand 13. The HIPAA boundary between treatment communications and marketing is enforced through a single segmentation policy, not ten interpretations 1. When a service line touches an FDA-cleared device, the cleared indication anchors the copy across every location, eliminating the per-site drift that produces off-label promotional language 12. For groups touching Medicare Advantage co-marketing, the CMS review window is built into one production calendar rather than negotiated locally 4.
The peer-reviewed framing of healthcare marketing as service design and communication architecture, not promotion volume, fits this model directly 7. A unified plan makes it possible to standardize the post-conversion surface, the comprehension level of landing pages, and the readability of pricing and consent disclosures across the portfolio.
Structural Comparison: Per-Location vs. Account-Level
The comparison below uses structural variables rather than industry-average dollar figures. Retainer averages, CAC benchmarks, and ROI multiples vary by vertical and are not supplied in the research base. The variables that do not vary are coordination cost, compliance approval surface, content reuse across locations, and attribution unification.
| Variable | Per-Location Agency Model | Account-Level Execution Model |
|---|---|---|
| Strategy plans in force | One per location | One per account, applied to all locations |
| Retainer count | One per location or service line | One program covering all sites |
| Substantiation file location | Distributed across agencies | Centralized, version-controlled 13 |
| HIPAA segmentation policy | Interpreted per site | One policy enforced across the portfolio 1 |
| FDA claim reconciliation | Per-campaign, per-agency | Anchored to the clearance document once 12 |
| CMS review windows | Negotiated locally | Built into one production calendar 4 |
| Content reuse across locations | Low; duplicated production | High; one asset adapted per market |
| Attribution surface | Location-by-location, often inconsistent | Unified at the account level |
| Approval cycle length | Multiplies with location count | Constant regardless of location count |
The structural reading is that per-location costs scale roughly linearly with site count, while account-level costs scale with channel and service-line count. For an operator with more than a handful of sites, the crossover happens early. Platforms that consolidate the work, such as Vectoron, price the program at the account level rather than the location level, which is the structural inverse of the legacy retainer model.
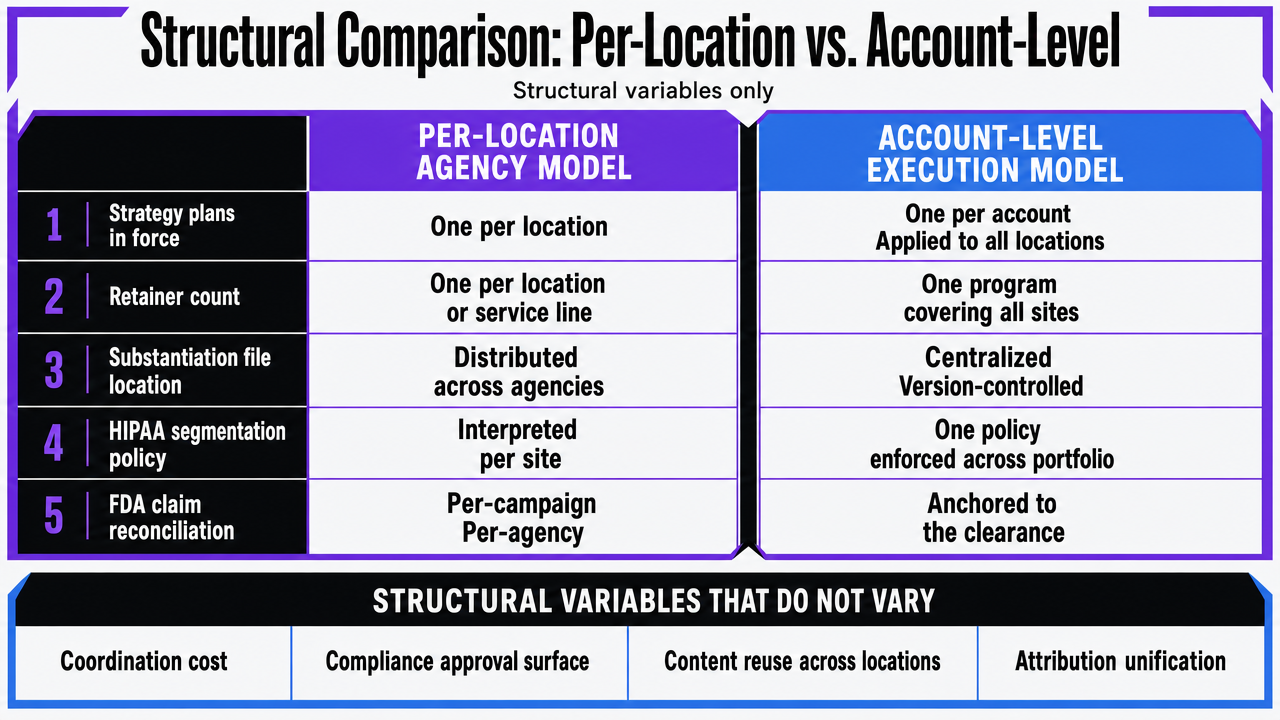 Visualize the side-by-side structural comparison between per-location agency models and account-level execution models, directly supporting the comparison table in this section
Visualize the side-by-side structural comparison between per-location agency models and account-level execution models, directly supporting the comparison table in this section
Operating Model Checklist for a Healthcare VP of Marketing
The work of running a compliant, evidence-grounded medical marketing program reduces to a short set of operating questions. Each one maps to a federal regime or to the patient-centered communication evidence base.
- Data flow: Is PHI being used to select, segment, or personalize any audience, and does each use sit inside a treatment, care coordination, or operations carve-out rather than the marketing definition that requires written authorization 1?
- Claim substantiation: Does every benefit or outcome claim have competent and reliable scientific evidence on file before the ad runs, with the file centralized rather than scattered across agencies 2, 13?
- Drug and device copy: Are broadcast prescription drug spots presenting the major statement clearly, conspicuously, and neutrally 3, and is device promotional language reconciled against the cleared or approved pathway document 12?
- Medicare communications: If any campaign touches Medicare Advantage or Part D, is the CMS review window built into the production calendar rather than negotiated per site 4?
- Comprehension test: Does each landing page let a patient at the targeted reading level identify what the service is, what it costs, what evidence supports it, and what alternatives exist 8, 9?
- Post-conversion instrumentation: Are kept-appointment rates, review sentiment, and dispute volume tied back to the campaign and page that produced each patient, so communication failures surface before they erode acquisition economics 11?
Six questions, one approval surface. Programs that can answer all six at the account level have already converted compliance from a downstream filter into an operating discipline.
Frequently Asked Questions
References
- 1.Marketing | HHS.gov.
- 2.Health Products Compliance Guidance - Federal Trade Commission.
- 3.Rx Drug Promotion and the Clear, Conspicuous, and Neutral Final Rule.
- 4.Medicare Marketing Guidelines - CMS.
- 5.Marketing Models, Standard Documents, and Educational Material.
- 6.Direct-to-Consumer Prescription Drug Advertisements: Presentation of the Major Statement in a Clear, Conspicuous, and Neutral Manner in Advertisements in Television and Radio Format Final Rule.
- 7.The impact of marketing strategies in healthcare systems - PMC - NIH.
- 8.“Best Practice” for Patient-Centered Communication - PMC - NIH.
- 9.Patient-Centered Communication and Shared Decision Making.
- 10.The Effects of Patient-Centered Communication on ... - PMC - NIH.
- 11.Communication in healthcare: a narrative review of the literature and ....
- 12.How to Study and Market Your Device | FDA.
- 13.FTC Policy Statement Regarding Advertising Substantiation.